PM154 Lecture 6 - Coronary Heart Disease
Learning Objectives
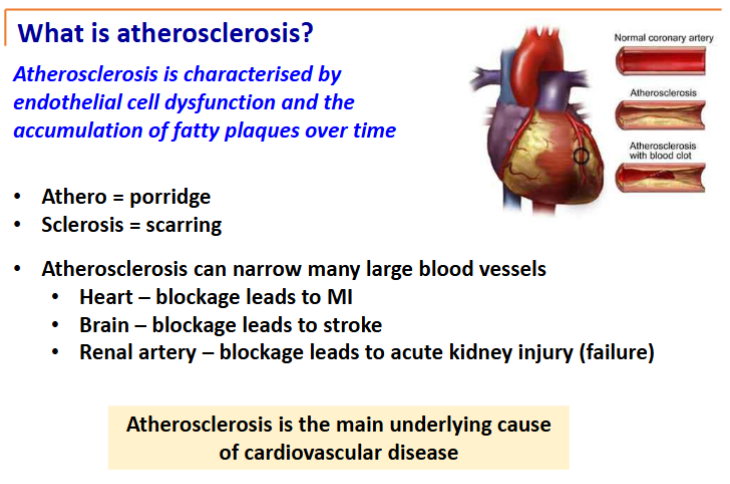
Explain the pathophysiology of atherosclerosis, coronary heart disease (CHD) and myocardial infarction (MI).
Artery structure
Endothelial cells line the lumen of all blood vessels acting as a barrier to keep circulating factors in the bloodstream
All blood vessels have 3 layers: intima - endothelial cells, media - smooth muscle and elastic tissue, adventitia - structural support
Layers present in all vessels but more obvious in large arteries & veins and depending on the vessel they have different amounts of each layer
Veins are “storage” for extra blood and have valves
Arteries have thick smooth muscle and elastic tissue for high pressure
Arterial walls are thicker than corresponding veins to accommodate pulsatile blood flow and higher blood pressure
Vocabulary
HDL (the good cholesterol) - goes around mopping up LDL (the bad cholesterol) and liver processes LDL and kicks it out.
Nitric oxide (NO) - vasodilates blood vessels and lets white blood cells to move around better
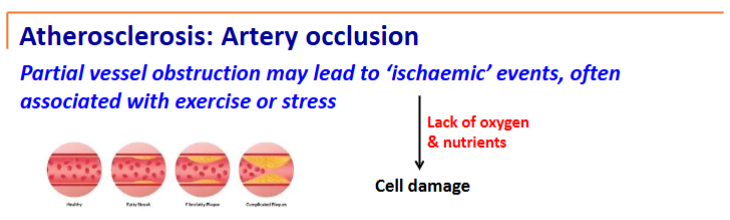
ischaemia - lack of blood/
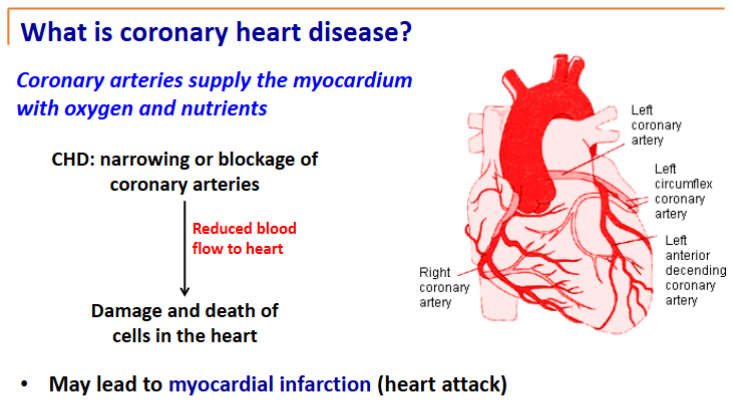
Coronary Heart Disease
Stable angina (pain on exertion) is the first step
Stress related - narrowing, but narrowing hasn’t exploded
Followed by unstable angina. Chest pain when not doing anything specific
Finally followed by a myocardial infarction (lack of blood supply and death to tissues of heart)
ECG changes as well as cells do not conduct signal as well
Risk factors
Non-modifiable
age, gender
lipid (cholesterol) profile
Modifiable
hypertension
activity levels
smoking/vaping
exercise
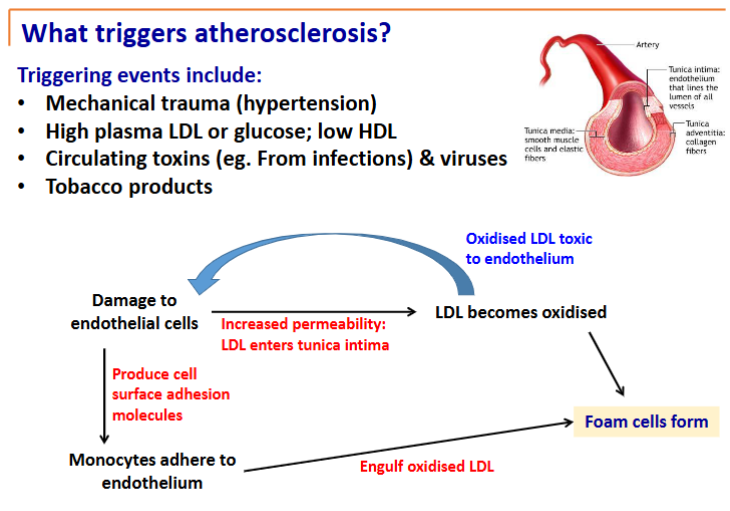
What triggers atherosclerosis?
Begins early and there is nothing we can do but it can be advanced by things that trigger atherosclerosis (above)
Elevated glucose over a long time binds to endothelial cells
GI flora that naturally live in colon/intestine - if taking antibiotics or poor diet they may change and produce toxins that enter the blood
Damage to endothelial cells
LDL can slip under endothelial cells to smooth muscle layer
High LDL levels = more LDL underneath
That LDL gets oxidised from metabolites from cells which then damages endothelial cells more
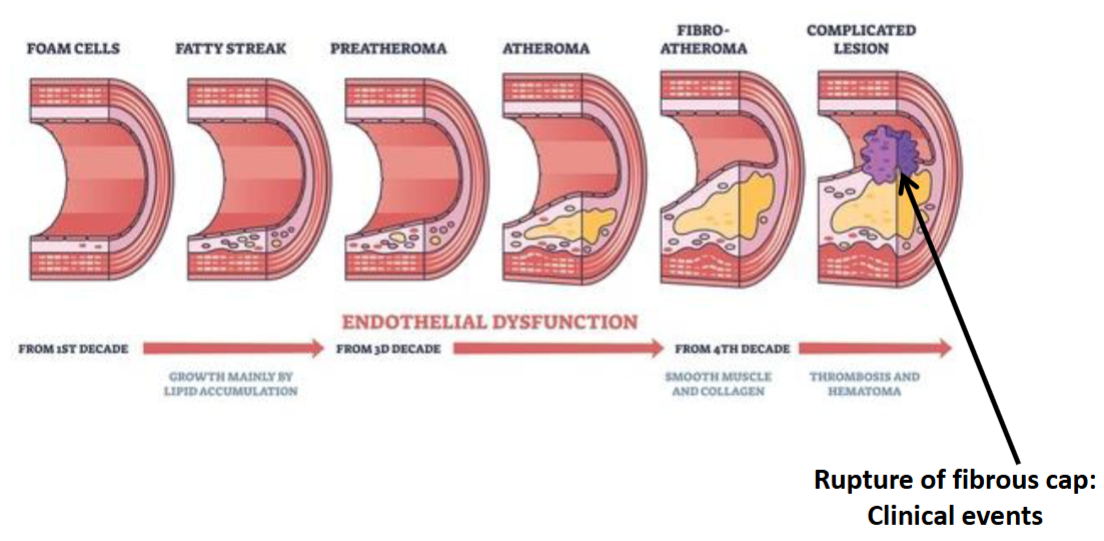
Damaged endothelial cells bring monocytes underneath them and monocytes eat the lipids and become really big becoming foam cells
at this point you still have wide arteries
Lipid core forms under endothelial cells with plaque formed over it
Vessel gets narrower
Potentially bursts
First place the blood goes from the aorta is the heart
But a narrowing in the arteries over a long period can lead to myocardial infarction
Stable angina - predictable chest pain, usually on exertion/stress; something that increases the demand of the heart
Unstable Angina - chest pain that occurs unpredictably
Myocardial infarction - heart does not get enough oxygen for a prolonged period leading to heart muscle death
if an artery is blocked for ~20 minutes, the tissues it supplies will die and form scar tissue
ischaemic cardiomyopathy - lots of things going on leading to reduced heart muscle efficiency; leading towards heart failure
Angina
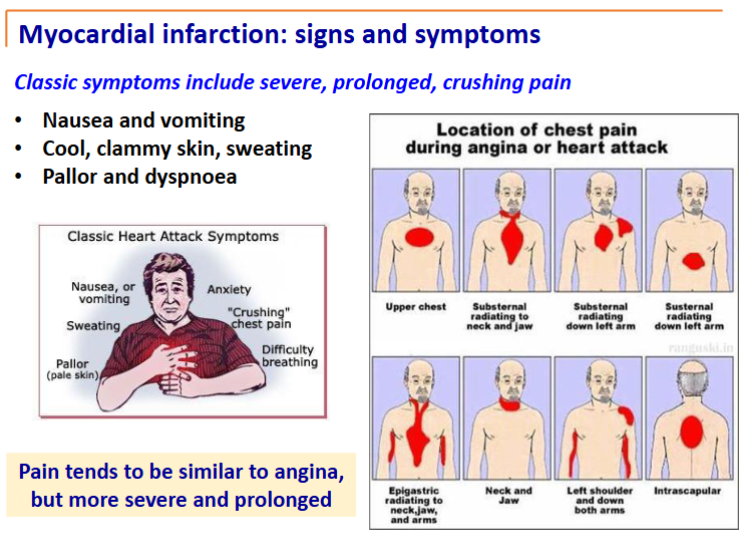
pain associated with angina is caused by myocardial ischaemia - pain lasts 3-5 minutes and may radiate to neck, lower jaw, left arm and shoulder
key thing whether stable or unstable: no permanent damage after pain recedes
stable angina
pain on physical exertion/stress/anything that requires increased nutrient delivery to heart
unstable angina
rupturing of an atherosclerotic plaque
dissolves away - intermittent reduction in blood flow which leads to pain
unstable and unpredictable - doesn’t have to be triggered by stress or exercise
how do you reduce the risk of angina?
taking aspirin with heart disease
inhibits platelets that form clots from clotting which makes it less likely to clot from a plaque
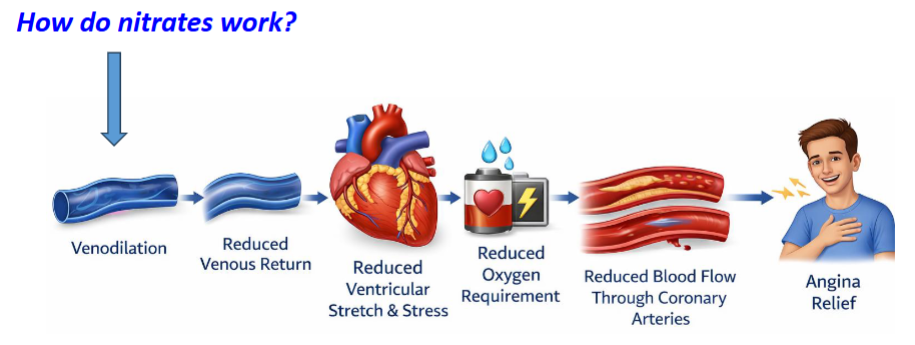
taking nitrates - causes venodilation (dilation of veins); more blood remains in veins (storage) so less blood goes back to the heart, therefore the heart stretches out less, so it requires less energy to pump out again
reduces oxygen demand of heart
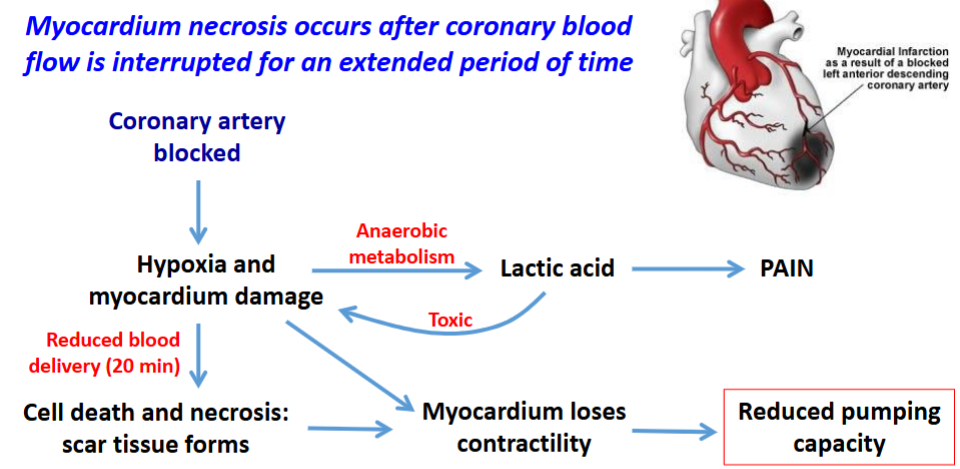
Myocardial Infarction (MI)
myocardium necrosis results from coronary blood flow being interrupted for an extended period of time
less oxygen
lactic acid and other chemicals released, causing damage
can’t contract as well - loses contractility
leads to uncontrolled cell death
scar tissue forms from affected myocardium - electrical currents don’t pass through scar tissue leading to arrythmias and potential heart failure
a heart attack activates the sympathetic nervous system
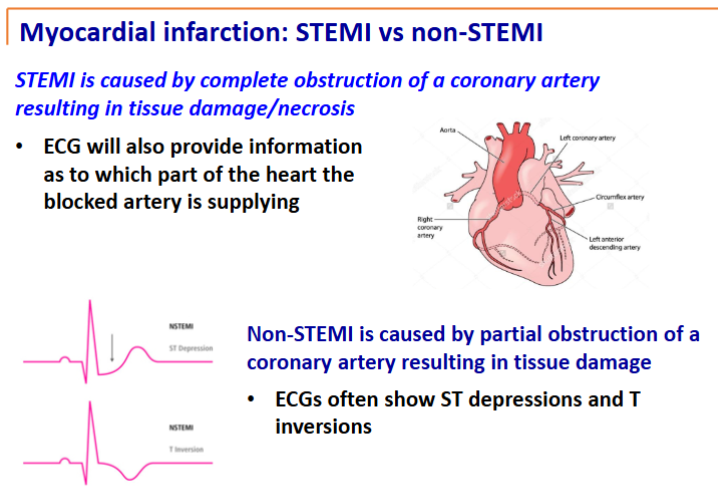
two major types of MI
STEMI (ST elevation MI)
Non-STEMI
electrocardiogram: an ECG will tell where the blockage is and whether the MI is STEMI or non-STEMI
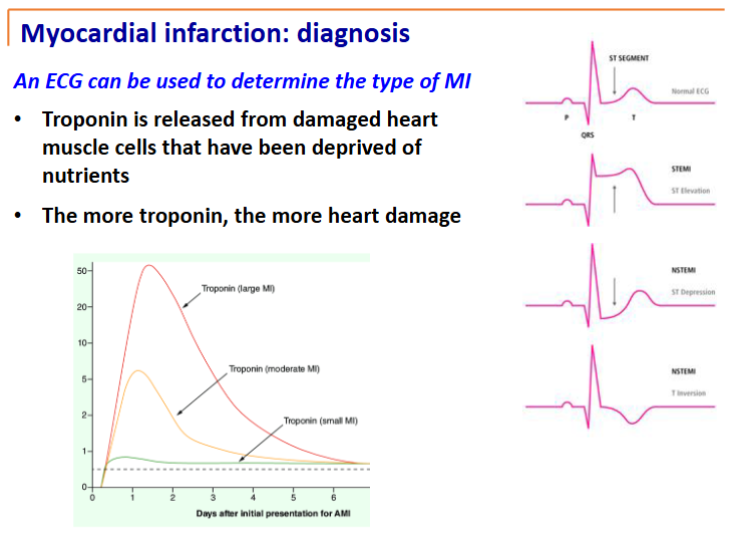
troponin is definitive, specific marker of heart damage
the more troponin, the more damage has been done
Angina vs Myocardial Infarction (heart attack)
Clammy skin that doesn’t evaporate
More prolonged than angina
Sharper pain
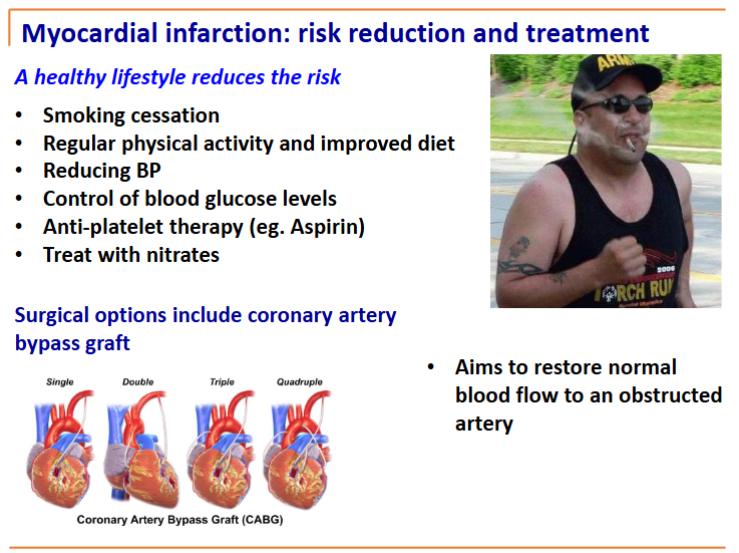
bypass graft takes blood from before the block and puts it in a place after the block