4.1 physical growth and infancy
what’s physical development like in the first 2 years?
• The section reviews physical development during infancy, from birth to two years, highlighting rapid growth in height, weight, and brain development.
• It discusses reflexes present at birth, explaining how involuntary movements evolve into voluntary motor skills through experience, enabling actions like grasping, rolling over, and walking.
• The development of the baby's senses is explored, noting that all senses operate at birth and how infants process sensory information into meaningful insights.
• The significance of early physical growth is addressed, emphasizing the critical role of nutrition due to the severe consequences of neglect.
physical growth and brain development in infancy
overall physical growth
• By 4 months old, an infant usually doubles its birth weight.
• By 1 year old, the infant typically has tripled its birth weight.
• By age 2, the weight has quadrupled.
• The average length for a 12-month-old is typically 28.5-30.5 inches.
• The average length for a 24-month-old is around 33.2-35.4 inches (CDC, 2010).
monitoring physical growth
• Rapid growth in infancy necessitates careful monitoring due to the severe consequences of neglect.
• Growth measurements at well-baby check-ups are often expressed in percentiles, comparing a baby's growth to peers of the same age.
• A percentile indicates the relative weight of a baby; for instance, the 40th percentile means the baby weighs more than 40% of peers.
• Changes in growth percentiles can alert pediatricians and parents to potential health issues.
• A significant drop in percentile, like moving from the 50th to the 20th, may indicate failure to thrive, warranting early intervention.
• Early detection of growth concerns allows for timely support for both the infant and caregiver.
body proportions
• A significant physical change occurs in body proportions during the first years of life.
• In the womb, the head accounts for approximately 50% of the total length.
• At birth, the head comprises about 25% of a person's length.
• By adulthood, the head reduces to about 15% of total length.
• This change poses challenges for infants, particularly when trying to raise their heads during the early months of life.
the brain in the first 2 years
• At birth, the brain is approximately 25% of its adult weight.
• By age 2, the brain reaches about 75% of its adult weight.
• The brain grows to 95% of its adult weight by age 6.
• By age 7, the brain achieves its full adult weight (100%).
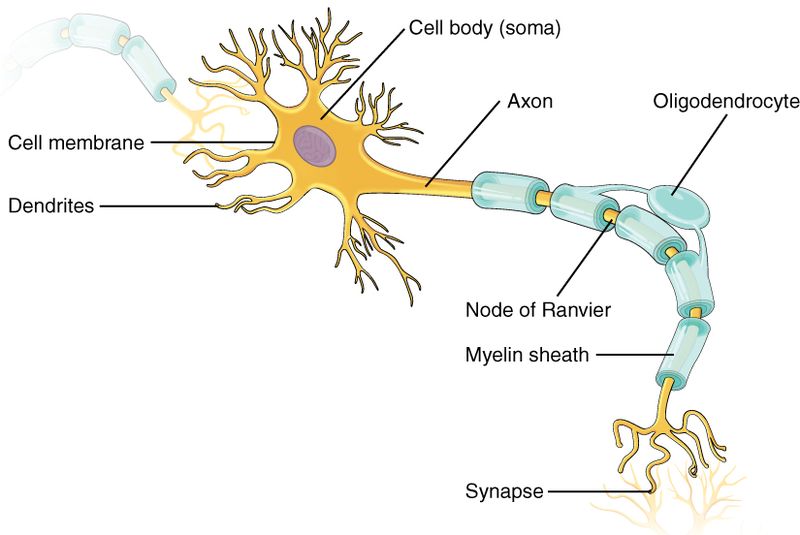
• Communication in the central nervous system (CNS) involves neurons, which connect via axons and dendrites.
• Neurons have one axon and multiple dendrites, resembling tree branches or fingers.
• Communication occurs at synapses, where electrical impulses release neurotransmitters, transmitting information between neurons.
• Most of the brain's neurons are present at birth but remain immature, forming new connections during infancy and toddlerhood.
• Dendritic connections experience transient exuberance, a period of rapid growth during the first two years, resulting in thousands of connections per neuron.
• After peak growth, pruning eliminates unused neural pathways, enhancing the efficiency of functioning and skill mastery.
• Pruning continues through childhood and adolescence, primarily in the cortex, which is vital for voluntary activity and thinking.
• The prefrontal cortex, found behind the forehead, matures throughout childhood, with significant development occurring during adolescence and comprising 85% of brain weight.
• About 40% of neural connections in the prefrontal cortex are lost as it matures, influenced by experiences.
• This maturation enables emotional regulation, planning, strategizing, and improved judgment in children, continuing through adolescence.
• Another significant change in the central nervous system is myelination, the fatty coating around neuron axons that insulates and speeds up impulse transmission.
• Myelin development enhances neural pathway formation, coordination, and thought processes, especially during the early years of life, and continues into adolescence.
motor and sensory development
from reflexes to voluntary movements
• Basic motor skills develop during the first two years of life, starting with reflexes.
• Infants have several reflexes essential for survival, including:
- Breathing reflex (maintaining oxygen supply).
- Reflexes for body temperature regulation (crying, shivering, tucking legs, pushing away blankets).
- Sucking reflex (automatically sucking objects touching the lips).
- Rooting reflex (turning towards objects touching the cheek for feeding).
• There are non-survival reflexes that indicate brain and body function, such as:
- Babinski reflex (toes fan upward when feet are stroked).
- Stepping reflex (legs move as if to walk when feet touch a surface).
- Palmar grasp (tight grasp on objects placed in the palm).
- Moro reflex (arms fling out when a loud noise is heard).
• These reflexes are automatic and indicate healthy neurological functioning.
• Reflexes are gradually replaced by voluntary movements within the first several weeks of life.
motor development
• Motor development in infants progresses from reflexive reactions to advanced motor skills in an orderly sequence.
• Development follows a cephalocaudal (head-down) and proximodistal (center-out) pattern.
• Milestones include:
- Holding head up: Average age 6 weeks, range 3 weeks to 4 months.
- Sitting alone: Average age 7 months, range 5 to 9 months.
• Delays in achieving milestones may indicate developmental concerns; parents should consult a pediatrician.
• Early intervention can address certain developmental delays.
gross motor skills
• Gross motor skills involve voluntary movements using large muscle groups, primarily in the arms, legs, head, and torso.
• These skills are among the first to develop in infants.
• Examples include lifting the chin when lying on the stomach and rocking on hands and knees.
• Infants may also use their feet to explore objects as early as 8 weeks of age while seated in a carrier.
• This foot movement can be easier than reaching with hands, which requires more practice.
• It is not uncommon for infants to crawl towards an object and unexpectedly move backward due to stronger arm muscles compared to leg muscles (Berk, 2007).
fine motor skills
• Fine motor skills involve precise movements of hands and fingers, focusing on small muscle coordination.
• These skills include reaching and grasping, essential for actions like toy manipulation, writing, and using utensils.
• Newborns initially cannot grasp objects voluntarily and will wave arms towards interesting items.
• By 4 months, infants can reach for objects with both arms, then transition to using one arm.
• The grasping method at this stage does not involve thumbs, utilizing only fingers and the palm.
• The thumb's functional use for grasping develops around 9 months, allowing infants to use the pincer grasp.
• This advancement significantly increases an infant's ability to control and manipulate objects, leading to engaging play like picking up small items and placing them in containers.
• By 9 months, infants also demonstrate the ability to follow and reach for moving objects, showcasing complex coordination compared to earlier months.
• 2 months: Can hold head upright; smiles at familiar voices and follows movement with eyes.
• 3 months: Raises head and chest while prone; smiles at others; grasps objects; rolls from side to back.
• 4-5 months: Babbles, laughs, tries to imitate sounds; begins rolling from back to side.
• 6 months: Moves objects between hands.
• 7-8 months: Sits without support; may start crawling; responds to own name; finds partially hidden objects.
• 8-9 months: Walks while holding on; babbles "mama" and "dada"; claps.
• 11-12 months: Stands alone; begins walking; says at least one word; can stack two blocks.
• 18 months: Walks independently; drinks from a cup; says at least 15 words; points to body parts.
• 2 years: Runs and jumps; uses two-word sentences; follows simple instructions; begins make-believe play.
• 3 years: Speaks in multi-word sentences; sorts objects by shape and color.
• 4 years: Draws circles and squares; rides a tricycle; socializes with people outside of the family; gets dressed.
• 5 years: Can jump, hop, and skip; knows name and address; counts ten or more objects.
sensory development
• Senses are crucial for infants and children in stimulating cognitive development and environmental observation.
• Sensation refers to the interaction of information with sensory receptors.
• Perception is the interpretation process of what is sensed.
• Individuals can sense without necessarily perceiving.
• As infants grow, their ability to perceive enhances, increasing their awareness and opportunities to interact with their environment.
vision
• Newborn infants possess significant sensory abilities, though not fully developed.
• Vision is the least developed sense at birth, with newborns seeing only 8 to 16 inches away and struggling to follow moving objects.
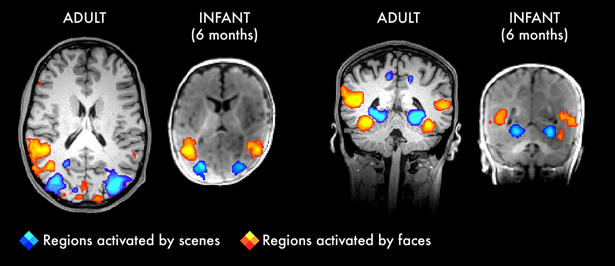
• Newborns detect contrast better than color differences and show a preference for faces.
• Initially, newborns look at less detailed parts of the face but begin focusing on more detailed features by 2 to 3 months.
• By 3 months, infants prefer unusual images, patterns over solids, faces over patterns, and three-dimensional objects over flat images.
• Color discrimination develops within a few months, achieving adult-like capabilities.
• Depth perception develops around 2 months, becoming more perceptible by 6 months.
• Infants who crawl tend to pay more attention to visual cues of depth and adjust their actions accordingly.
hearing
• Infants have a keen sense of hearing at birth, noted as early as the 5th month of prenatal development.
• They can distinguish between similar sounds as early as one month after birth.
• Infants show a preference for human voices, listening longer to speech over other sounds.
• They prefer their mother's voice over a stranger's voice very early on.
• A study revealed that 3-week-old babies sucked more strongly on pacifiers that played their mother's voice compared to a stranger's voice.
• By 7 or 8 months, infants begin to lose some sensitivity to unfamiliar sounds as they become accustomed to the sounds of their native language.
pain and touch
• Newborns are sensitive to touch, temperature, and pain, showing distress through crying and physiological responses.
• Circumcision without anesthesia causes pain, as evidenced by increased blood pressure and heart rate, along with decreased blood oxygen and elevated stress hormones.
• The American Academy of Pediatrics (AAP) acknowledges both medical benefits and risks associated with circumcision, advising against routine procedures but allowing parental choice due to potential benefits.
• Acute touch sensitivity in infants is vital for developing physical skills, cognitive abilities, and social-emotional competencies.
• Positive gentle touch has immediate and long-term developmental benefits, influencing bonding with caregivers and communication of needs.
• Touch is particularly beneficial for premature infants and has significant impacts on all children's development.
• A case study of Romanian orphans highlighted the detrimental effects of insufficient touch and interaction, leading to developmental delays.
• Touch plays a crucial role in fostering safety, protection, trust, and secure attachments between infants and caregivers.
taste and smell
• Infants are sensitive to touch and can differentiate between various flavors: sour, bitter, sweet, and salty.
• Newborns show a preference for sweet flavors.
• They can recognize their mother’s scent, preferring it over others.
• When placed on the mother’s chest, a newborn will move towards the mother’s breast, which emits a strong maternal odor.
• Even at birth, infants are attracted to their mother's odor, which has a calming effect when they cry (Sullivan et al., 2011).
sleep and health
infant sleep
• Infants aged 0 to 2 years average 12.8 hours of sleep per day, with gradual developmental changes.
• Newborns sleep 14 to 17 hours daily during the first three months, becoming increasingly alert over time.
• Approximately 50% of infant sleep consists of REM sleep, starting with REM cycles rather than non-REM.
• Parents often worry about infants' sleep patterns, which vary significantly among individuals.
• A 2018 study indicated that at 6 months, 62% of infants slept at least six hours nightly, while 38% did not achieve six uninterrupted hours.
• At 12 months, 28% of children still struggled to sleep six hours, with 78% achieving that mark and 56% sleeping at least eight hours.
• Nighttime waking is the most reported sleep issue by parents, leading to significant sleep loss for new parents, especially mothers.
• Sleep disruption for parents can last until the child is around six years old.
• By six months, infants generally sleep 14-15 hours a day, including 3-4 hours of daytime naps.
• Naps decrease with age, typically transitioning to two naps a day between 9-18 months and often leading to one longer nap by 18 months.
• Changes in sleep habits may occur during periods of rapid weight gain or new developmental skills like crawling or walking.
sudden unexpected infant deaths (SUID)
• Approximately 3,500 Sudden Unexpected Infant Deaths (SUID) occur annually in the U.S. among infants under one year of age.
• SUID types include:
- Sudden Infant Death Syndrome (SIDS): Leading cause of death in infants up to 12 months. About 1,400 infants died from SIDS in 2020. Risk peaks at 4 to 6 weeks. Possible cause relates to brainstem abnormalities affecting breathing regulation. Key risk factors include low birth weight, previous SIDS in siblings, sleep apnea, ethnicity, low socioeconomic status, and smoking in the home.
- Unknown Cause: Deaths after an investigation fails to determine cause.
- Accidental Suffocation and Strangulation: Causes include soft bedding, being rolled on by another person, wedging, and strangulation between crib components.
• In the 1970s, research indicated higher death rates for face-down sleeping.
• Following 1992 AAP safe sleep recommendations to place infants on their backs, combined SUID rates reduced significantly.
• The Back to Sleep Campaign in 1994 helped lower the SIDS rate from 130 per 100,000 live births in 1990 to 40 in 2015.
• Risk factors often involve a mix of biological and social conditions; stomach sleeping has been widely addressed in education campaigns.
co-sleeping
• The location of infant sleep varies by age and culture, with bed-sharing and co-sleeping being common in some societies (Esposito et al., 2015).
• Colvin et al. (2014) analyzed 8,207 child deaths, revealing higher risks associated with bed-sharing, especially in infants aged 0-3 months.
• Carpenter et al. (2013) found that infants under three months sleeping in the same bed as parents are five times more likely to die from SIDS than those in separate sleep spaces.
• The American Academy of Pediatrics (AAP) updated safe sleep recommendations in 2016, advising infants to always sleep on their backs on a firm surface and to avoid soft bedding.
• Joint recommendations include room-sharing without bed-sharing, ideally until the baby is one year old, which can reduce SIDS risk by 50%.
• Breastfeeding is advised, along with avoiding exposure to smoke, alcohol, and drugs.
• New evidence supports the practice of skin-to-skin care for newborns.
nutrition
• Good nutrition and a supportive environment are essential for healthy infant growth and development.
• Infants triple their weight and increase their height by half in the first year, necessitating proper nutrition.
• Exclusively breast milk or formula is recommended for the first 6 months.
• Establishing healthy nutrition practices early fosters positive dietary habits in children.
• Infants require adequate nutrients to support their rapid physical growth.
• Malnutrition can lead to physical, cognitive, and social issues, hindering an infant's growth potential.
introducing solid foods
• Breast milk or formula is the sole nutrition for newborns; exclusive breastfeeding is advised for the first six months.
• Solid foods can be introduced around six months when infants have developed sitting and oral feeding skills.
• Solid foods should supplement breast milk or formula rather than replace them.
• By six months, the gastrointestinal tract matures, allows easier digestion of solids, and reduces allergic reactions.
• Teeth typically begin to develop around this age, aiding in chewing.
• Iron-fortified infant cereal (rice, barley, or oatmeal) is often the first solid food introduced due to high iron content.
• Avoid salt, sugar, processed meats, juices, and canned foods for infants.
• Solid foods are usually consumed more frequently as toddlers grow, starting between 4 to 6 months.
• Pediatricians recommend introducing new foods one at a time for a few days to monitor for allergies.
• It is crucial to offer a variety of foods rich in essential vitamins and nutrients, including iron, calcium, and vitamin D, as toddlers can be picky eaters.
immunizations
• Preventing communicable diseases in infants is a key task for the Public Health System in the USA.
• Infants explore by mouthing objects, leading to exposure to potential contaminants.
• Immunizations serve as a critical method of disease prevention, enabling the immune system to defend against pathogens.
• Historical struggles with diseases like Polio and whooping cough highlight the importance of vaccinations.
• A significant number of children remain unvaccinated due to personal or religious beliefs, affecting public health.
• The concept of herd immunity indicates that when 90% of a community is vaccinated, disease transmission decreases significantly.
• In 2017, California implemented regulations limiting exemptions from vaccinations to only medical reasons, impacting childcare personnel requirements.