Mood
MOA A/B destroys NE. GABA-T destroys GABA.
GABA y, phasic, benzo sensitive
GABA a, tonic, benzo INsensitive
flumazenil - benzo od reversal, GABA antag
GABAA receptors with α2 and/ or α3 subunits may be most important for regulating anxiety and are the presumed targets of the anxiolytic and sedative hypnotic benzodiazepines. a1 sleep
Changes in structural and functional outcomes in depression in fact may be potentially reversible when captured at the stage of loss of synapses without loss of neurons, and that is what rapid-acting drugs for depression, which act on glutamate and GABA systems, hold promise for doing: namely, triggering the formation of new synapses
tx w/ GABA/glutamate targeting drugs can be neurorestorative to synapses, possible neurogensis. rapid acting to restore synapses, potential for future.
The idea is that whenever adjustment of specific neurotransmitter-mediated neurotransmission can enhance the efficiency of information processing in the hypothetically malfunctioning circuits for each specific symptom, it will relieve that symptom. If successful, this targeting of neurotransmitters in specific brain areas could even eliminate all symptoms and cause a major depressive episode to go into remission
symptom based/targeted tx (addressing circuits assoc w/ the symptoms) attempts to address the individual patient’s needs and thereby provide relief of the specific symptoms of that individual patient rather than treating all patients with a given diagnosis the same
DRUGS
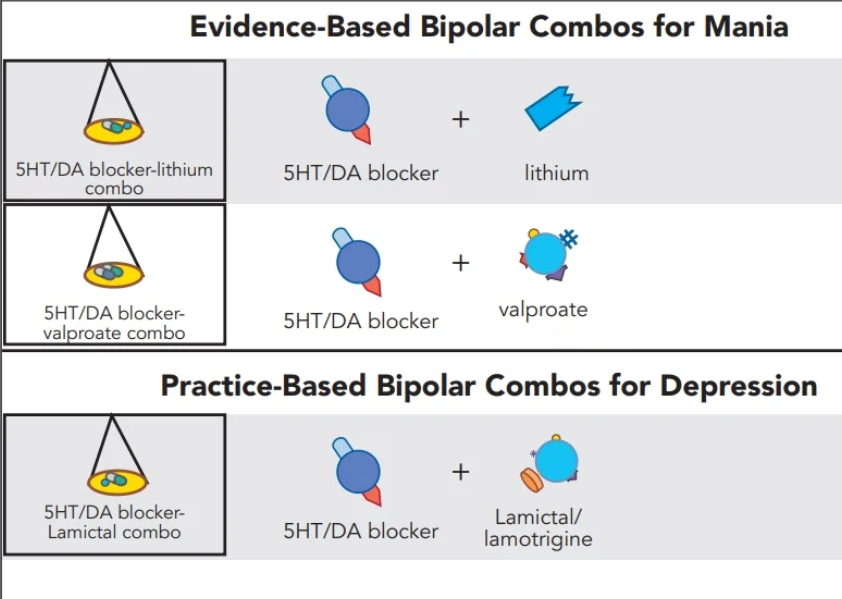
acute bipolar mania is treated with serotonin/dopamine blockers in much the same manner as acute psychosis is treated in schizophrenia, including dosing and expected onset of action within minutes to hours
lithium and valporate are commonly used in conjunction with those dopamine/serotonin blockers approved for mania but not schizo, bc lith/val dont augment the blockers in schizo
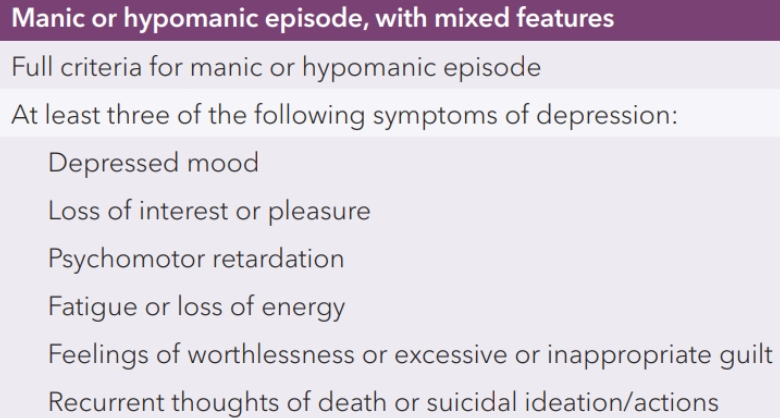
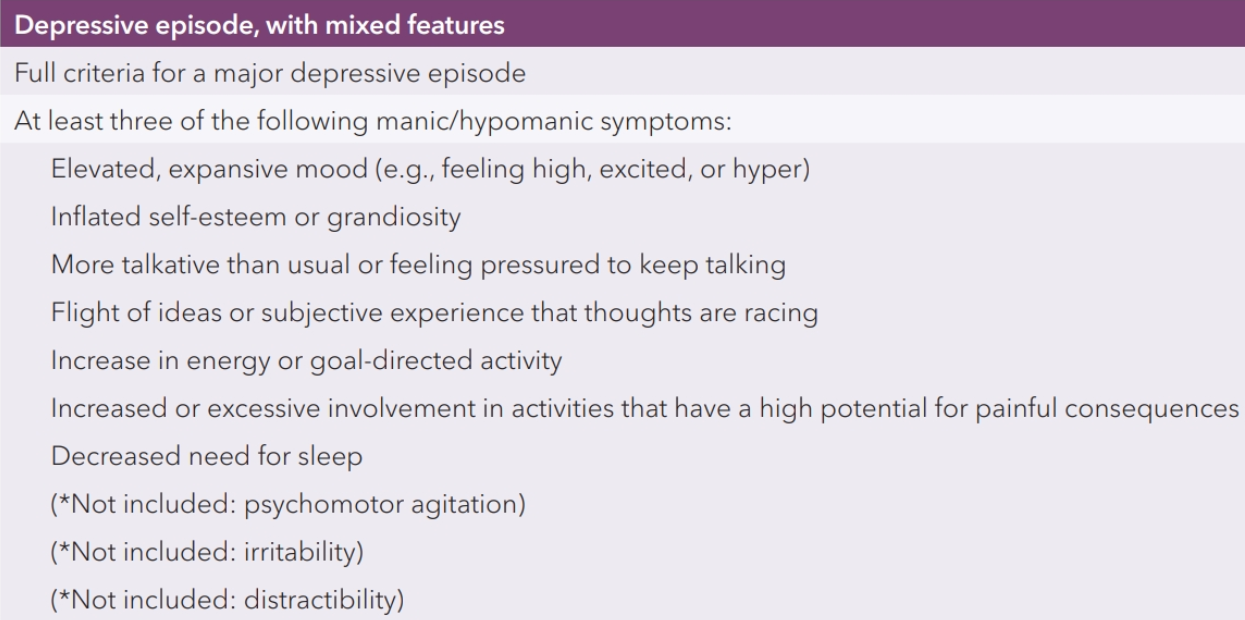
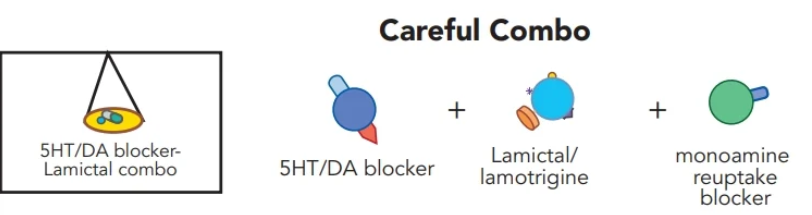
first-line treatment is one of the specifically approved serotonin/dopamine blockers, not a monoamine reuptake inhibitor (for dpn w/ mixed features or bipolar)
Olanzapine (5HT/DA blocker/antag 2nd gen antipsychotic) – Fluoxetine (SSRI) - approved for schizophrenia, bipolar mania, treatment-resistant unipolar depression, and bipolar depression.
Quietapine (5-HT2A/D2 antagonism and 5-HT1A partial agonism 2nd gen atypical antipyschotic) - approved for schizophrenia, bipolar mania, and for augmentation of SSRIs/SNRIs in treatment-resistant unipolar depression, bipolar dpn.
Like olanzapine, D2 antagonism by quetiapine could theoretically help keep the lid on treatment from below so it doesn’t spill over into activation and mania
Lurasidone (DA/5HT/a2 blocker/antag some agonist action at 5HT1 second gen atypical antipsychotic) - approved for the treatment of schizophrenia. Lurasidone is prescribed for bipolar depression and for mixed features at doses lower than those generally used for the treatment of psychosis in schizophrenia, and is generally well tolerated with little propensity for weight gain or metabolic disturbances and is one of the most widely prescribed agents for bipolar depression
Cariprazine (D3/D2/5HT1A partial agonist 2nd or 3rd gen atypical antipsychotic) - approved for the treatment of acute bipolar mania and for acute bipolar depression, with ongoing trials as an adjunct to SSRI/SNRIs in unipolar depression. α1 and α2 antagonist actions aka anti dpn properties. UNIQUE D3 HIGH AFFINITY. blocking these disinhibits DA release into the PFC, explains anti dpn action and reduction in negative symptoms of schizo. causes Improvement in energy, motivation, and “brightening” observable beh
Lithium (antimanic/mood stabilizer mech of action unclear - interaction with downstream signal transduction cascades) - proven effective in manic episodes, and in maintenance of recurrence, especially for manic episodes and, perhaps to a lesser extent, for depressive episodes. established to help prevent suicide. SE issues and monitoring burden.often utilized now as one member of a portfolio of treatments, often allowing once-daily administration and at lower doses when combined with other mood stabilizers as opposed to euphoric mania monotherapy. SE - gastrointestinal symptoms such as dyspepsia, nausea, vomiting, and diarrhea, as well as weight gain, hair loss, acne, tremor, sedation, decreased cognition, and incoordination. potential long term kidney/thyroid dmg. THERAPEUTIC RANGE - .8 - 1.2
carbamazepine and valproate proved effective in treating the manic phase of bipolar disorder
ANTICONVULSANTS FOR MD
Valporic acid (possible MoA inhibiting voltage-sensitive sodium channels, boosting the actions of the neurotransmitter GABA, and regulating downstream signal transduction cascades) - proven effective for the acute manic phase of bipolar disorder, and is commonly used long-term to prevent recurrence of mania, although its prophylactic effects have not been as well established. Some experts believe valproic acid is more effective than lithium for rapid cycling and mixed episodes of mania. SE such as hair loss, weight gain, and sedation, COMPLIANCE issues? possible preg concerns and SE assoc w/ chronic use.
Carbamazepine (hypothesized to act by blocking voltage-sensitive sodium channels (VSSCs)) - shown to be effective in the manic phase of bipolar disorder. more profound immediate suppressant effects upon the bone marrow (than valporic), requiring initial monitoring of blood counts (blood counts including platelets should also be periodically monitored on valproate), and notable induction of the cytochrome P450 enzyme
V and C can cause fetal toxicity such as neural-tube defects. valproate is proven effective in migraine, but carbamazepine is proven effective in neuropathic pain
Lamotrigine (VSSC inhibition and dec release of glutamate) - approved to prevent recurrence of both mania and depression in bipolar disorder. generally well tolerated EXCEPT rash that could lead to SJS.
Oxcarbazepine/Eslicarbazepine (binding to the open-channel conformation of the VSSC at a site within the channel itself on the α subunit) - less sedating, having less bone marrow toxicity, and also having less CYP450 3A4 interactions than carbamazepine. Less proven for manic episodes but used off label for tolerability.
Topiramate (blocking voltage-gated sodium channels to reduce neuronal excitability, enhancing the activity of the inhibitory neurotransmitter GABA at GABA-A receptors, and antagonizing glutamate receptors) - approved as an anticonvulsant and for migraine, and recently, in combination with bupropion, for weight loss in obesity. Can be given w/ antipsychotic for weight concerns. ambiguous results
Gabapentin and Pregabalin (a2 ligands) - These anticonvulsants seem to have little or no action as mood stabilizers, yet are robust treatments for various pain conditions, from neuropathic pain to fibromyalgia, and for various anxiety disorders
Calcium Channel Blockers (L-Type) - evidence suggests that calcium channel blockers, especially dihydropyridine-type calcium channel blockers, may be useful for some patients with bipolar disorder
Riluzole (binds to VSSCs and prevents glutamate release) - developed to slow ALS progression
combinations are the Standard for Treating Bipolar Disorder
Dextromethorphan–Bupropion/Dextromethorphan–Bupropion and Dextromethorphan–Quinidine - NMDA receptor antagonist dextromethorphan with the CYP450 2D6 inhibitor and NDRI bupropion/ CYP450 2D6 inhibitor quinidine. Dextro needs inhib or it’s metab too quickly. In trials for tx resistant dpn ESPECIALLY NDRI version (fast track by FDA). Also alzheimers trails.
Dextromethadone (μ-opioid agonist) - NMDA shepherd effect. NMDA antag being explored as it gives rapid anti-dpn effects
Hallucinogen-Assisted Psychotherapy
3,4-Methylene-dioxymethamphetamine MDMA (transforms into a powerful serotonin reuptake inhibitor with VMAT2 inhibition causing enhanced serotonin release as well. hallucinogen)
psilocybin - bind to a number of serotonin receptor subtypes. Psilocybin has been designated a breakthrough therapy by the US FDA for treatment of depression