Essentials of Population Health in Canada
Introduction
The development of Population Health in Canada: Reports and Conferences
- Lalonde Report, 1976
- The minister of Nation Health and Welfare wrote A New Perspective on the Health of Canadians
- Is the first document to acknowledge that health is based on more than just biology
- Alma-Ata Conference, 1978
- WHO held a conference for global cooperation
- Where the slogan “Health for All” came from
- The Conference’s 10-point states declaration state health is a fundamental right
- Ottawa Charter for Health Promotion, 1986
- Was to add to statements from the Alma-Ata Conference
- They were going to make real changes by 2000
- The Lalonde Report was also brought in to reinforce the up-and-coming changes
- EPP Report, 1986
- Focused on healthcare for disadvantaged groups
- Disease prevention and management
- Recommend it to be supported by all levels of government
- The Public Health Program Initiative
- Proved health was decided by multiple factors
- Diet
- Exercise
- Income
- Toward a Healthy Future: Report on the Health of Canadians, 1996
- First to recognize and incorporate the determinant of health into its findings and recommendations
- Concluded that Canadians had one of the healthiest populations
- National Forum, 1994-1997
- The beliefs and values of people across the country were sought for input
- Two reports were published saying that more concrete evidence is needed
- The Mazankowski Report: A framework for reform (2001)
- Purpose to preserve healthcare services for Alberta
- By letting doctors perform privately after x number of years
- Making elective services out of pocket
- Creating province-wide records and health Cards
- Alberta pays too high taxes
- 2003 Alberta has province-wide records and health cards
- Kirby report: The Health of Canadians- Federal Role (2002)
- Purpose: Canadian Health Care system about healthcare the Federal Government
- Like the Mazankowski Report
- Unsustainable to be left alone
- Taxes gauged on income
- Creating wait times; then shipping patients elsewhere to receive treatment (reasonable Access) all paid for by the government
- Government funding for medications depends on income
- $4.5 billion to go towards information technology and advanced medical equipment
- Government incentive to come and work in Canadian healthcare
- Ontario adopted taxes gaged on income
- The Romanow Report: Building on Values: The Future of Health Care in Canada (2002)
- Purpose: Adapt Canada’s Health Care System, create disease prevention and awareness to promote health
- Like the Mazankowski Report
- Got Canadian opinions through forums and meetings held across the country
- The belief that Universal health care was sustainable but needed to figure out how (readjusting)
- Opposed private healthcare
- Create a council to improve health care, maintain the system, and report to the citizens
- Accountability to the Canadian Health Act
- Coverage for homecare, diagnostic testing, palliative care, and mental health care
- EI and job security to extending family for taking care of loved ones
- Drug costs are subject to the terms and conditions covered
- New drugs should be monitored and tested federally; drug prices are kept within a range
- Wait times be monitored but not limited
- (2004) $10 billion will be put into health care over ten years
- (2004) Council was created and funds health care, postsecondary education, and welfare
- Wait times have been limited and monitored
- Funding for information and technology as well as EI/job security
- Drug prices have been monitored in most provinces and tested federally
Determinants of Health
- Most people fail to see the socioecological aspects of health
- The Public Health Agency recognizes 12 determinants of health
- Income and social status
1. Poorer one lives the sicker they are and the shorter they are expected to live
- Social Support Networks
1. Those who have networks where they can trust each other makes them feel safer and happier 2. They tend to feel they have more of a purpose
- Education and Literacy
1. Higher education equates to more money later on meaning they have a higher socioeconomic standing 2. Can mean less stress more rounded, individual 3. Higher education may give them more of a purpose
- Employment and Working Conditions
1. Ones with high stress, low wages, and menial jobs have a higher mortality rate 2. People with high-stress rates in the home have more mental illness 3. Without work means they are missing general health care benefits 4. The majority of single people working alone have 2 part-time jobs
- Social Environment
1. How people behave 2. Gender, culture, and ethnic group all affect their education and roles in the workforce 3. Having a small tight-knit group of friends makes for a healthy work-life balance 4. Volunteering creates a sense of family as well as accomplishments making them generally live longer and healthier
- Physical Environment
1. Includes:
1. Food 2. Water 3. Air 4. Homes 5. School 6. Roads
- How much population they breathe in and the amount of radiate in the area
- Personal Health and Practices and Coping Skills
1. These are self-imposed risks
1. Smoking 2. Driving over the speed limit 3. Drinking 2. Coping-skills
1. How people deal with their problems 2. Those who adjust well to change, deal with stress easily have good coping skills
- Healthy Child Development
1. Begins at conception 2. What the mother does while she is pregnant
1. E.g. if she drinks, smokes, and between about healthcare eats healthy all affect the baby 3. Researchers are still looking for more links between social determinants of health to the development of the children
- Biology and Genetic Endowment
1. All the attributes inherited by parents 2. The socioeconomic and environmental structure may affect biology
- Health Services
1. Diagnose and treatment 2. Greater availability of primary care services could lead to more preventative measures
1. Leading to a healthier population
- Gender
1. Lesbian: female attracted to another female 2. Gay: an individual (either male or female) attracted to someone of the same sex and/or gender 3. Bisexual: an individual attracted to both male and female people. 4. Transgender (or trans): an umbrella term that refers to an individual who does not identify (fully or in part) with the gender they were assigned at birth 5. Transsexual: a person whose gender identity does not correspond with the sex they were assigned at birth. Some transsexual people have, for example, sex reassignment surgery and/or hormone therapy. 6. Queer: historically, a derogatory term for homosexuality. Some members of today's LGBTQ community have reclaimed this term. 7. Questioning: an individual who is unsure of or still exploring their sexual orientation or gender identity and may want to avoid using another label. 8. Two Spirit: a modern umbrella term used by some Indigenous people instead of other terms (lesbian, gay, bisexual, trans, queer). The term reflects how all aspects of identity are interrelated (Eagle Canada Human Rights Trust, 2018). 9. affect effect how they react to their surroundings
- Culture: a way of life
1. Different cultures may find it hard to ask for help in a new country
1. It could be because of
1. Fear 2. Language barrier 3. Isolation 2. They may feel overlooked, isolated, stressed, and mentally, emotionally, and physically drained
Population Health Approach
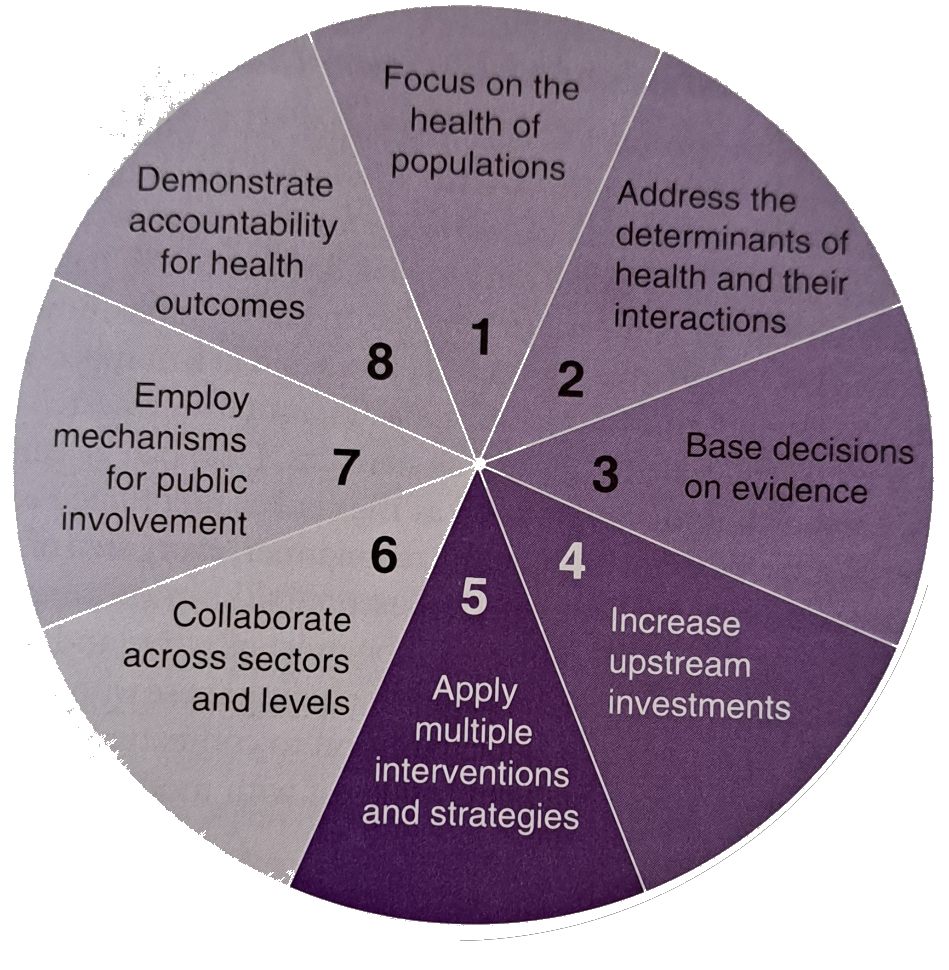
Key Elements
- Focus on the Health of the Target Population
- Address the Determinants of Health and their Interactions
- One thing leads to another, leads to another is the cause is caught when the population can gets healthier
- Use Evidence-formed Decision Making
- Evidence-informed decision making: All stages of a population health approach-selecting issues, choosing interventions, deciding to implement and continue this interventions-are supported by decisions based on the most current best evidence available.
- Quantitative research: deals with the numbers that are typically used in statistic
- Increase Upstream Investments
- Upstream Investments: the process of making decisions that will benefit the health of a population before there is a problem
- Short and long-term goals are set to prioritize evidence-based decision making
- Apply Multiple Strategies
- Once a goal is set steps are made to complete the goal
- Collaboration is essential
- Collaborate Actions Sectors and levels
- Intersectoral collaboration: developing partnerships between different segments of society to improve health
- Engage the Public
- Public involvement is the best and easiest way to do well
- They want to know where their tax dollars are going
- Helps to build trust and transparency
- Demonstrate Accountability for Health Outcomes
- This is done by
- Determine baseline measures
- Setting targets
- Monitoring progress
- Once information is gathered it will be publicized with the evaluation’s results
Population Health Promotion Model
- The integrated model of population health organizes it into three areas
- What-looking to the health determinants to measure the health of populations
- How-creating and implementing prioritized strategies to improve health
- Who-engaging multiple stakeholders to participate in health improvement strategies
- Demonstrates the complexity of health promotion
- Health promotion policies are made using three criteria
- Research and studies on health issues
- Knowledge gained through experience
- Reflect back to anticipate for future events
Population Health in Canada and Abroad
- PHAC continues to work and strengthen the healthy population
- The work gathered and distribute information to better ourselves