1. Paralytic/Incomitant Strabismus Part 1
Introduction to Paralytic/Incomitant Strabismus
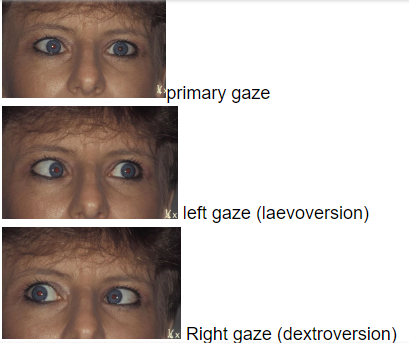
Definition: A paralytic or incomitant type of strabismus where the angle of deviation changes depending on the direction of gaze.
Primary Deviation: The strabismus observed in the affected eye when the unaffected eye is fixating.
Secondary Deviation: The angle of strabismus is larger when the affected eye is fixating.
generally secondary > primary = incomitant
secondary = primary = comitant
Potential Causes: Paralytic strabismus can result from pathology or injury to:
The brain
Cranial nerves
Neuromuscular junction
Extraocular muscles
Orbit
Optometric Role: While treatment options from an optometric perspective are limited, the primary responsibility of an optometrist is to identify recent and potentially urgent cases. This is crucial because such cases may indicate significant, potentially life-threatening, neurological causes.
Differentiating Terms
Paralysis: Refers to a complete loss or impairment of function.
Paresis: Denotes an incomplete or partial paralysis.
Palsy: Also refers to an incomplete or partial paralysis.
Interchangeable Use: These terms (paralysis, paresis, palsy) tend to be used interchangeably in clinical practice.
Aetiology of Paralytic Strabismus
Congenital: Present at birth or shortly thereafter, often due to a developmental anomaly of the motor system, anatomy, muscles, or nerves.
typically are asymptomatic - vision system compensates for the problem.
Acquired: Occurs due to injury or disease affecting the ocular motor system (brain, nerves, neuromuscular junction, extraocular muscles, orbit).
typically present with acute onset of diplopia.
Detailed Causes of Acquired Paralytic Strabismus
Patients with acquired paralytic strabismus frequently present to optometrists. Many involved conditions can be serious or life-threatening:
Trauma:
Cranial trauma
Birth trauma (e.g., forceps injury leading to VI nerve damage)
Perforating wounds to the orbit
Orbital fractures
Orbital haemorrhage
Inflammation:
Cellulitis
Cavernous sinus thrombosis
Sinusitis
Syphilis
Encephalitis
Vascular Disease – Metabolic:
Diabetes
Atherosclerosis
Thyroid eye disease
Idiopathic: The cause is unknown.
Tumours/Masses:
Intracranial tumours
Aneurysms
Orbit or optic nerve (ON) tumours
Secondary invasion of the orbit by tumours (e.g., from sinuses)
Choroidal melanoma
Toxic:
Acute infectious disease
Exposure to lead or alcohol
Anaesthesia applied to the spine
Neuromuscular Junction Disease:
Myasthenia Gravis: Characterized by signs and symptoms that worsen as the day progresses.
Understanding Extraocular Muscle Actions
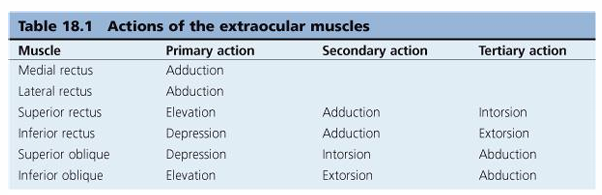
Table 18.1 Actions of the Extraocular Muscles:
Medial Rectus:
Primary action: Adduction
Lateral Rectus:
Primary action: Abduction
Superior Rectus:
Primary action: Elevation
Secondary action: Adduction
Tertiary action: Intorsion
Inferior Rectus:
Primary action: Depression
Secondary action: Adduction
Tertiary action: Extorsion
Superior Oblique:
Primary action: Depression
Secondary action: Intorsion
Tertiary action: Abduction
Inferior Oblique:
Primary action: Elevation
Secondary action: Extorsion
Tertiary action: Abduction
Definition of Isolated Action: These actions describe the movement caused by an individual muscle acting alone from the primary position.
Clinical Testing of Ocular Motility
Context of Muscle Function: In clinical assessment, extraocular muscles do not work in isolation and are often not in primary gaze.
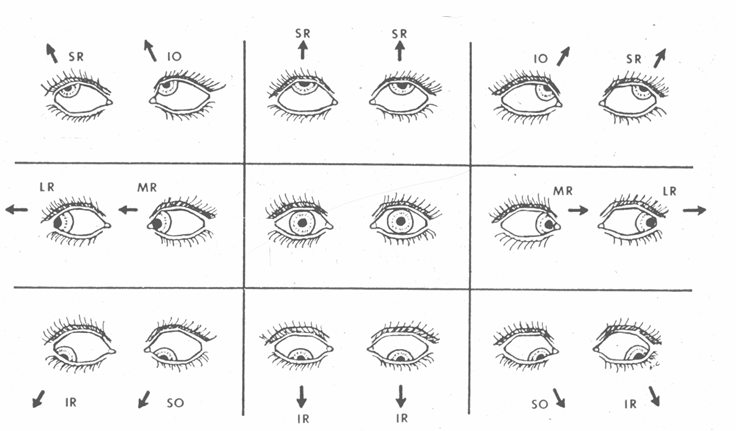
Field of Action: It is crucial to consider a muscle's "field of action." This is defined as the direction in which the muscle's line of pull has the greatest mechanical advantage. Paralysis of a muscle will typically be most evident when the eye is looking in its field of action.
Horizontal Muscles:
Lateral Rectus (LR): Abduction (outward gaze)
Medial Rectus (MR): Adduction (inward gaze)
Vertical & Oblique Muscles: Their primary action is most effective depending on whether the eye is in abduction or adduction.
Superior Oblique (SO): Depression in adduction (down and in)
Inferior Oblique (IO): Elevation in adduction (up and in)
Inferior Rectus (IR): Depression in abduction (down and out)
Superior Rectus (SR): Elevation in abduction (up and out)
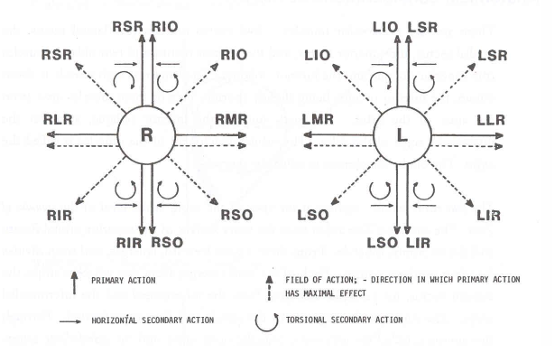
Yoke Muscles: Muscles in different eyes that work together to produce conjugate gaze in a specific direction (e.g., Right Superior Rectus (RSR) and Left Inferior Oblique (LIO) are yoke muscles for upward gaze to the right).
Diagnostic Action Fields: Visual representations (e.g., Hess screen diagrams) illustrate the directions of gaze where primary muscle actions have maximal effect, including horizontal, secondary, and torsional actions.
Investigation of Paralytic Strabismus
Careful Case History and Symptoms: Essential for understanding the patient's experience.
Comprehensive Ocular Examination: Includes external eye examination and fundus inspection.
Ocular Motility Assessment: Evaluation of eye movements in all directions of gaze.
Cover Test: Used to detect and measure strabismus.
Hess Screen: A diagnostic tool to plot the field of action of each extraocular muscle and identify underactions/overactions.
Old Photographs: Can be useful to identify if an abnormal head posture or strabismus has been long-standing.
Symptoms during History Taking
Recent Onset Acquired Cases: Symptoms may be sudden and dramatic.
Major Symptom: Usually Diplopia (double vision).
Diplopia isn't necessarily present in the primary position of gaze.
May be difficult to elicit from younger children.
Long-standing cases might show few or no symptoms due to adaptation.
Other Symptoms:
Diplopia (often with a vertical component)
Abnormal head position (compensatory head tilt or turn)
Blurred vision (especially with IIIrd nerve palsy)
History of injury or disease of the eye and orbit
Symptoms from an underlying pathology (e.g., headache, vertigo).
Differentiating Old vs. New Ocular Motor Palsy
Sign/Symptom | Long-standing Ocular Motor Palsy | Recent-onset Ocular Motor Palsy |
|---|---|---|
Diplopia | Rare | Almost always present |
Onset | Generally unknown | Usually sudden |
Amblyopia | Common | Rare |
Recent Trauma? | Not usual | Common |
Symptoms | Not usual | Common and extreme |
Comitance | Spread of comitance may obscure original palsy | Always incomitant |
Abnormal Head Posture | If present, well established and difficult to alter. | Can be marked but easy to alter. Covering paretic eye eliminates problem |
Past-pointing | Absent | Present |
General Health | Not usually a factor | Current health may be a significant issue |
Diplopia History: Key Questions
When a patient reports diplopia, asking these four questions can guide diagnosis:
Monocular or Binocular?
Method: Cover one eye. Does the diplopia persist?
Monocular Diplopia: If diplopia persists, it's monocular.
Potential Causes: Cataract, high astigmatism, corneal scar, keratoconus
MONOCULAR = not paralytic
Horizontal or Vertical?
Horizontal Diplopia: Images appear side by side. Often indicates issues with horizontal recti muscles (Medial Rectus or Lateral Rectus).
Vertical Diplopia: One image appears on top of the other. Often indicates issues with vertical recti or oblique muscles.
Combination: If both are present, ask which component (horizontal or vertical) is greater.
Worse in Certain Directions of Gaze?
Horizontal Diplopia: e.g., Worse when looking to the right suggests issues with the Right Lateral Rectus (RLR) or Left Medial Rectus (LMR).
isolated paralysis of MR is rare due to innervation of IIIrd nerve.
more likely to be the RLR that is just innervated by the 6th CN.
Vertical Diplopia: e.g., Worse when looking to the right suggests issues with the Right Superior Rectus (RSR), Right Inferior Rectus (RIR), Left Inferior Oblique (LIO), or Left Superior Oblique (LSO).
most likely to be LSO due to being innervated by the 4th CN
Greater at Distance or Near?
Horizontal Diplopia: e.g., Worse looking right and straight ahead (distance) suggests a problem with the Right Lateral Rectus (RLR).
Vertical Diplopia: e.g., Worse looking right and near suggests a problem with the Left Superior Oblique (LSO).