Week 9 - 7MNT0004 - Vitamin D
Vitamin D Overview
Course Information
Module: Vitamin D 7MNT0004
Date: Nov 27th, 2025
Instructor: Dr. Karen O'Callaghan
Institution: School of Life Course & Population Sciences, Faculty of Life Sciences & Medicine
Learning Outcomes
Understand sources of vitamin D
Understand current recommendations for vitamin D intake in the UK
Understand the risk factors for vitamin D deficiency
Understand the consequences of vitamin D deficiency
Vitamin D Metabolism
Definition: Vitamin D is a seco-sterol and a fat-soluble vitamin.
Types of Vitamin D:
Ergocalciferol: Vitamin D2
Cholecalciferol: Vitamin D3
Production of Vitamin D:
D3: Produced endogenously in the skin.
D2 and D3: Found in a limited number of foods.
Hydroxylation Reactions
Overview: Vitamin D undergoes two hydroxylation reactions for activation.
First Hydroxylation:
Location: Liver
Reaction: Vitamin D → 25-hydroxyvitamin D
Product: 25(OH)D [main circulating metabolite]
Enzyme: Catalyzed by cytochrome P450 enzyme CYP2R1 and other 25-hydroxylases.
Second Hydroxylation:
Location: Kidney
Reaction: 25(OH)D → 1,25-dihydroxyvitamin D
Product: 1,25(OH)2D [active hormonal metabolite]
Enzyme: Catalyzed by mitochondrial enzyme CYP27B1.
Mechanism of Action
Receptor Binding:
1,25(OH)2D binds to intracellular vitamin D receptor (VDR) in target tissues.
Exerts biological effects via gene transcription.
Inactivation:
Subsequent hydroxylation reactions yield inactive metabolites.
Enzymes involved: 24-hydroxylase converts to 24,25-dihydroxyvitamin D and 1,24,25-trihydroxyvitamin D.
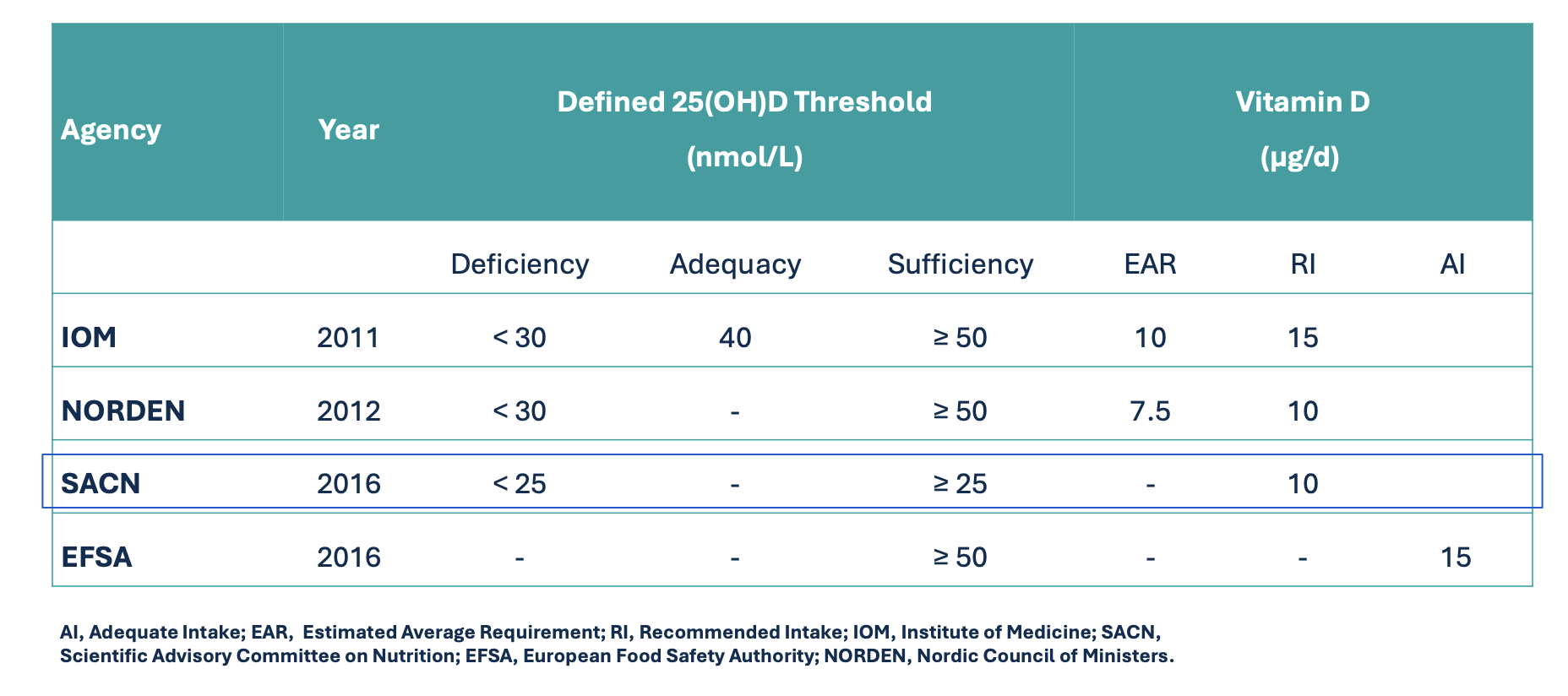
Dietary Reference Values (DRVs) for Adults
Dietary Sources of Vitamin D
UK Context:
Dairy fortification is not mandatory.
Some plant-based milks are fortified.
Importance of fortified cereals, especially for children.
Food Sources:
Limited sources of vitamin D include:
Egg yolk
Oily fish
Liver
Trace amounts found in some plant foods.
Cereals when fortified, may aid children
Sunlight as a Source of Vitamin D
Overview: Sunlight is the most significant source of vitamin D in the UK.
Process: Photochemical reaction involving UVB converting 7-dehydrocholesterol to pre-vitamin D3.
Wavelength Requirement: Needs UVB rays in the wavelength range of 290-320 nm.
Seasonal Consideration:
Vitamin D production is latitude-dependent.
Limited vitamin D production above 40°N or Southern latitude.
In the UK, sunlight conversion occurs only from approximately April to September.
October to March referred to as “Vitamin D Winter”
Supplementation Recommendation:
Daily vitamin D supplementation of 400 IU (10 µg) recommended from October to March.
Recommendations from SACN
Serum 25(OH)D Concentration: Should be ≥ 25 nmol/L year-round.
Sunlight Exposure: No specific recommendations on the amount of sunlight exposure to maintain serum concentrations.
Recommended Nutrient Intake (RNI) for Vitamin D:
10 µg/d from all dietary sources for the UK population aged > 4 years.
Assumes minimal UVB exposure.
Applicable throughout the year.
Pregnant and Lactating Women: RNI is equivalent to non-pregnant adults.
Children < 4 years: Data insufficient to set RNI; safe intake is 8.5-10 µg/d for infants (0-1 years) and 10 µg/d for ages 1-4 years.
The median intake in UK adults is around 3µg
Risk Factors for Vitamin D Deficiency
Analysis: Refers to studies and population surveys assessing vitamin D levels.
Low Dietary Vit D Intake
Vegan/vegetarian w/o supplementation
Exclusive breastfeeding w/o infantile supplementation
Reduced Skin Exposure to sunlight
High latitude
Clothing
Skin pigmentation
Suncream
Environmental Pollution
Ageing: Reduction in dermal 7-dehydrocholesterol
Smokers
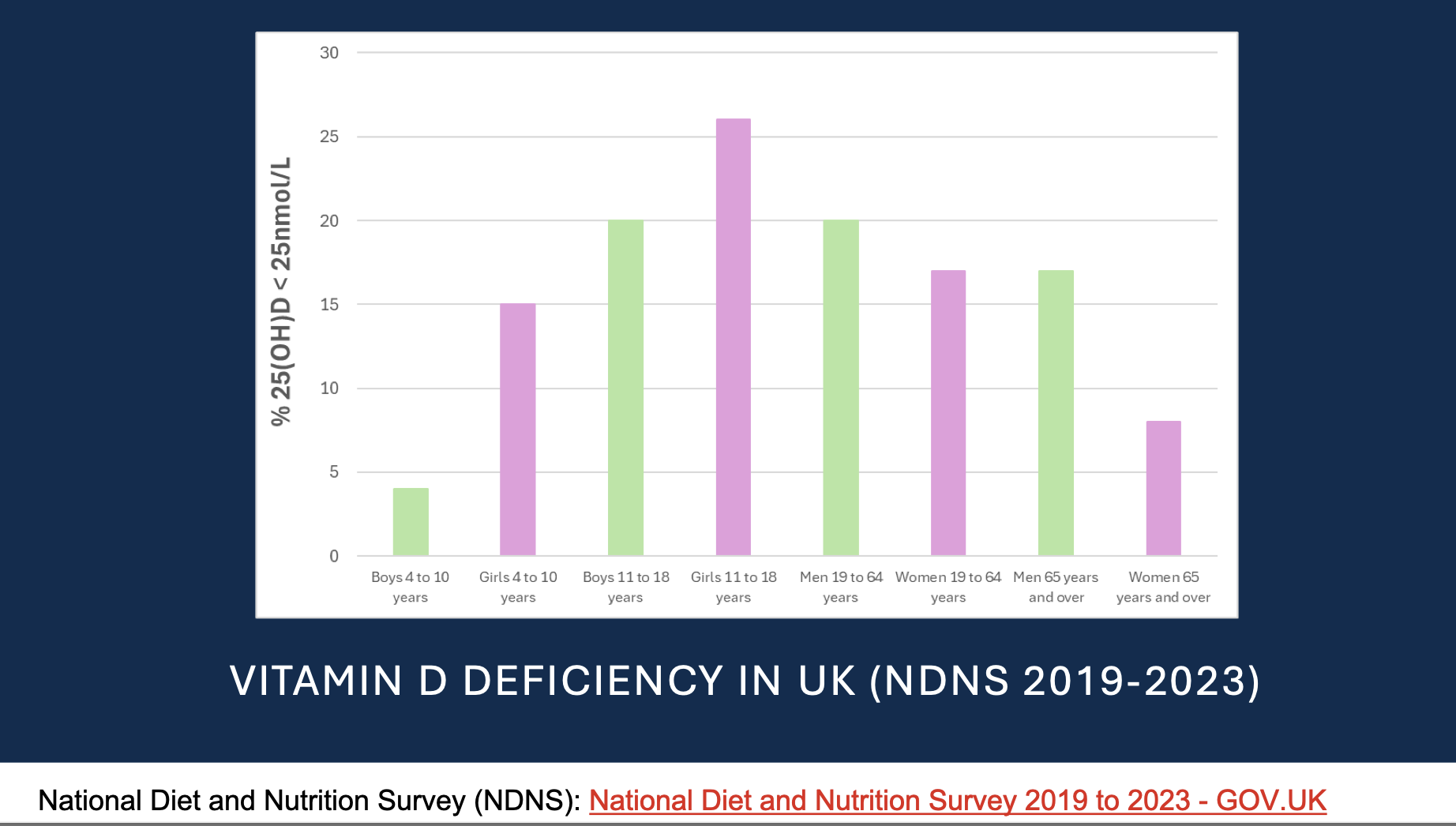
Vitamin D Deficiency in the UK (NDNS 2019-2023)
Source: National Diet and Nutrition Survey (NDNS) 2019-2023, provided by UK Government.
Geographical Variation in Vitamin D Status
Data from UK Biobank (2006-2010) among adults ages 40-69:
Trend: 25(OH)D highest in southern regions.
Findings: Highest prevalence of deficiency (25(OH)D < 25 nmol/L) noted in Scotland.
Seasonal Variation in Vitamin D Status
Proportion of individuals with 25(OH)D < 25 nmol/L by season.
Winter: Highest deficiency rates observed due to limited sunlight exposure.
Spring: Gradual improvement in vitamin D levels as sunlight increases.
Summer: Peak vitamin D levels recorded, with lower deficiency rates.
Autumn: Levels begin to decline again, with a rise in deficiencies as days shorten.
Demographic Variation in Vitamin D Status
Vitamin D deficiency varies by:
Ethnicity Prevalence:
Asian: 54%
Black: 35%
Chinese: 27%
White: 12%
Smoking Status:
Current smokers: 22%
Non-smokers: 13%
Socio-Economic Status:
Least deprived: 10%
Most deprived: 20%
Vitamin D Toxicity / Hypervitaminosis D
Status: Vitamin D is a fat-soluble vitamin.
Half-life: Approximately 15 days for 25(OH)D.
Toxicity Threshold: Typically associated with 25(OH)D concentrations > 375 – 500 nmol/L1.2.
Tolerable Upper Intake Level: Established at 4000 IU/d or 100 µg/d.
Consequences of Toxicity:
Characteristic feature is hypercalcemia (high blood calcium levels) or hypercalciuria (high urinary calcium).
Long-term toxicity may lead to cardiovascular and renal damage due to tissue calcification.
Causes of Toxicity:
Prolonged dietary exposure (high dose supplementation).
Skin synthesis of vitamin D ceases once skin reddening occurs; therefore, prolonged sun exposure does not result in toxicity.
Role of Vitamin D and Consequences of Deficiency
Vitamin D and Bone Health
Main Role: Maintenance of calcium and phosphate homeostasis.
Aids in absorption of calcium and phosphorus.
Triggers mobilization of calcium from bones when blood calcium is low.
Activation of osteoclasts to dissolve bone matrix.
Facilitates renal calcium reabsorption.
Mechanism Overview:
Increased parathyroid hormone (PTH) when serum calcium is low stimulates calcium absorption and renal reabsorption.
Higher levels of 1,25(OH)2D lead to decreased PTH levels.
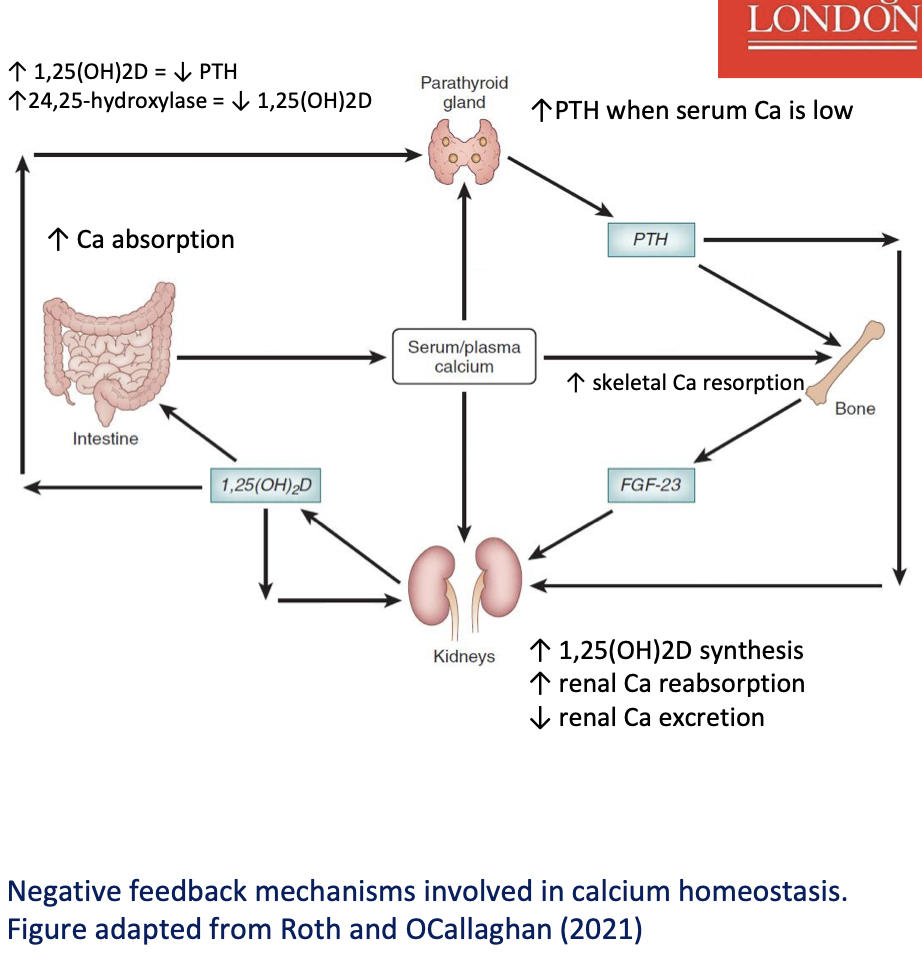
When serum calcium (Ca²⁺) is low, the parathyroid gland increases parathyroid hormone (PTH) secretion.
PTH acts on three main targets to restore blood calcium:
1. Kidneys
↑ Renal Ca reabsorption → ↓ urinary Ca loss
↑ 1α-hydroxylase activity → ↑ production of 1,25(OH)₂D (active vitamin D)
↓ Renal Ca excretion
2. Intestine (via 1,25(OH)₂D)
1,25(OH)₂D increases intestinal Ca absorption
This raises serum/plasma calcium
3. Bone
PTH stimulates skeletal Ca resorption (osteoclast activity)
Ca is released from bone into the blood
Negative feedback regulation
As serum Ca rises, it:
Suppresses PTH secretion
Reduces further Ca release and conservation
1,25(OH)₂D also suppresses PTH and:
Stimulates 24,25-hydroxylase, which breaks down active vitamin D (termination mechanism)
FGF-23 (from bone) acts on kidneys to:
Reduce 1,25(OH)₂D synthesis
Fine-tune mineral balance
Clinical Features of Vitamin D Deficiency
Common Symptoms:
Characteristic feature is an under-mineralized or under-calcified bone matrix.
Secondary hyperparathyroidism.
Severe deficiency leads to hypocalcemia causing muscle cramps and twitching.
Conditions Due to Deficiency:
Adults: Osteomalacia.
Children/Adolescents: Rickets.
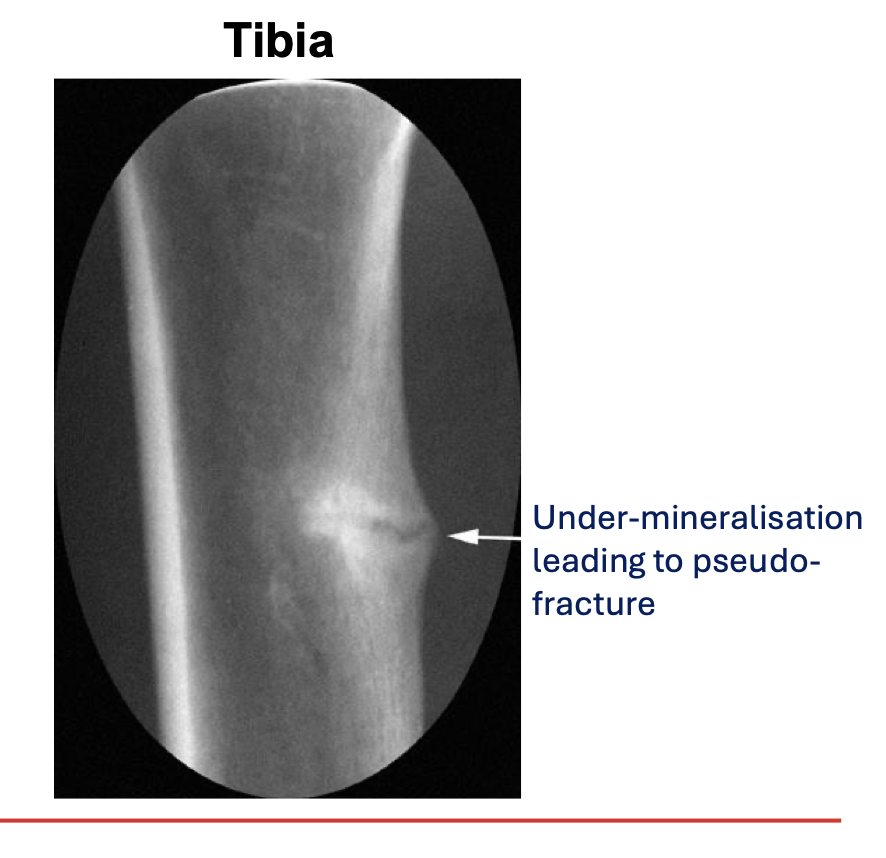
Osteomalacia Symptoms
Description: “Softening of the bones”.
Impaired bone remodeling due to lack of vitamin D.
Typical findings:
Low 25(OH)D.
High PTH.
Serum calcium often maintained within normal range due to regulation by PTH.
Pseudo-fractures resulting from under-mineralized bone.
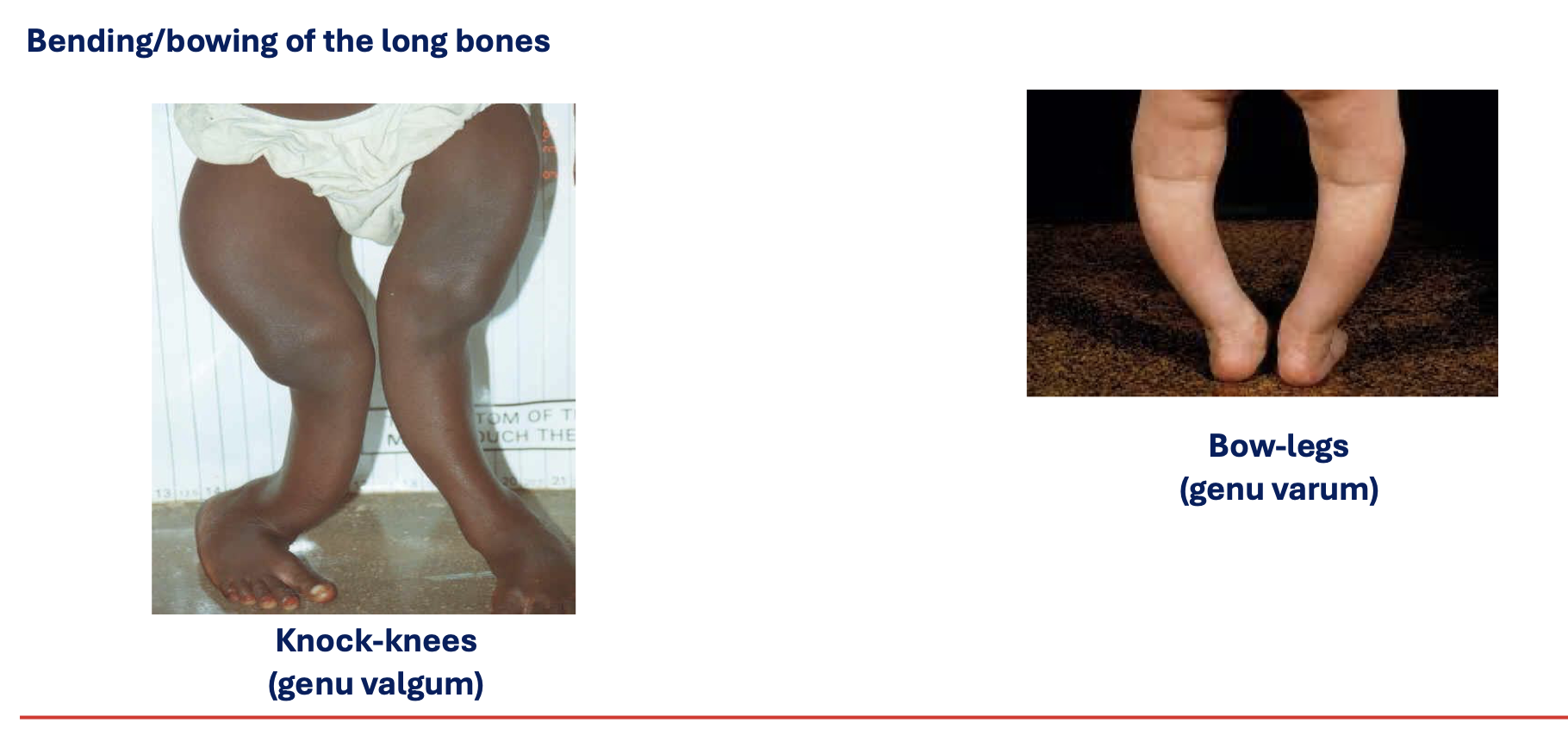
Rickets Symptoms (Disorder of growth plates)
Clinical features include:
Bending/bowing of the long bones.
Bow-legs (genu varum)
Knock-knees (genu valgum).
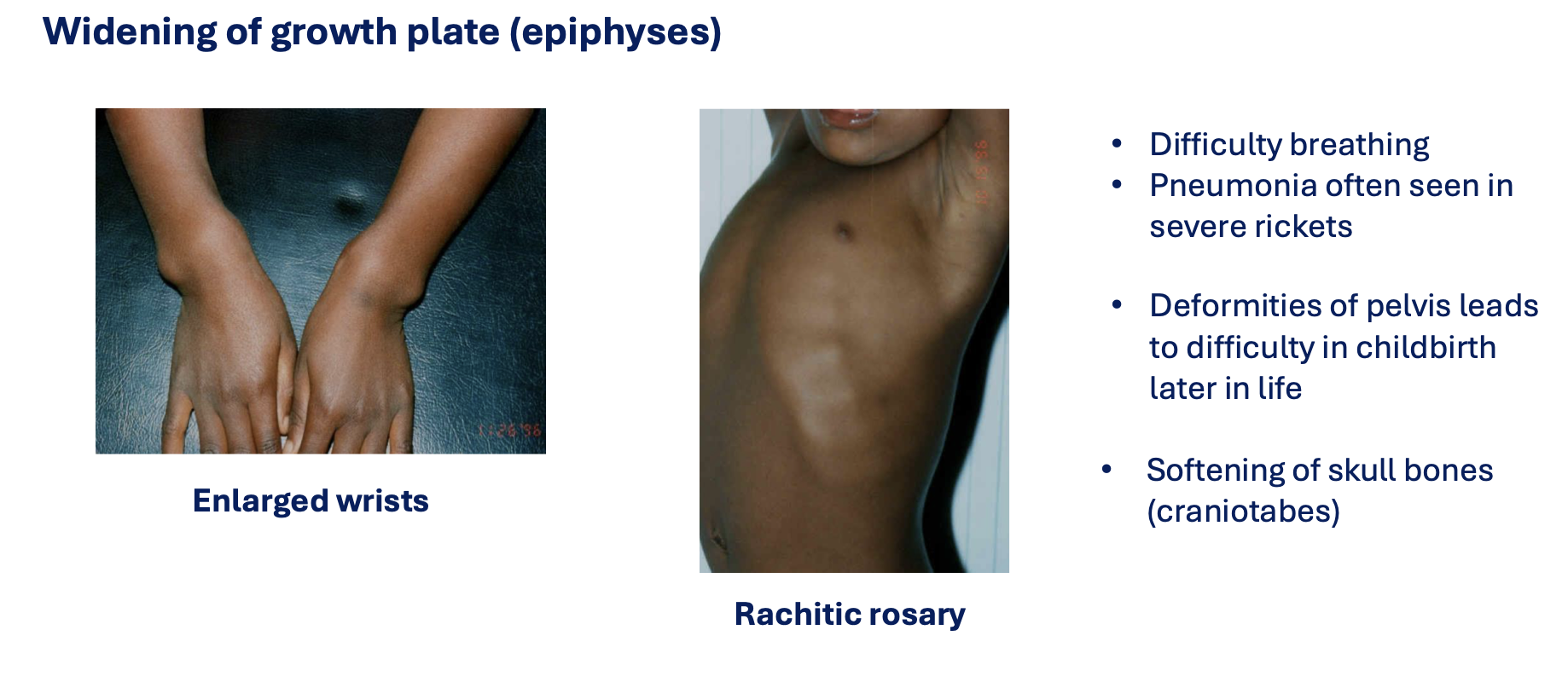
Enlarged wrists.
Rachitic rosary.
Difficulty breathing; severe cases may lead to pneumonia.
Deformities of pelvis impacting childbirth.
Softening of skull bones (craniotabes).
Widening of growth plate (epiphyses).
It is essentially impaired bone mineralization and long bone growth
It is treated with Vitamin D (+Calcium)
Historical Context of Vitamin D Deficiency
Industrial revolution (18th and 19th centuries) linked to lower sun exposure and increased nutritional rickets in northern European cities.
Rickets is caused by impaired bone mineralization and long bone growth, often treated with vitamin D and calcium supplementation.
Treatment and Prevention of Rickets
UV Light Exposure: Used historically for treatment.
Effective elimination of rickets as illuminated by Hernigou et al. 2019.
Vitamin D Supplementation in Infancy
Policy: Routine vitamin D supplementation for infants <1 year to prevent nutritional rickets (5-10 µg/d).
In the UK, 8.5-10 µg/d recommended for:
Breastfed infants
Infants receiving <500ml/d of infant formula.
Children aged 1-4 years recommended to take 10 µg/d.
Free supplements available through the Healthy Start scheme.
Non-Skeletal Roles of Vitamin D
Vitamin D Receptor (VDR): Found in various cell types; plays a significant role in gene expression regulation.
Local expression 1-alpha hydroxylase suggests 1,25 (OH)2D production and regulation of VDR-mediated gene expression is important for functioning of various tissues.
Health Correlations:
Epidemiological studies link lower 25(OH)D levels with increased risks of cardiovascular diseases, certain cancers, and autoimmune diseases.
Causation from observational data is not confirmed, as low vitamin D may also result from poor health.
RCTs often show no effects from additional vitamin D on health outcomes.
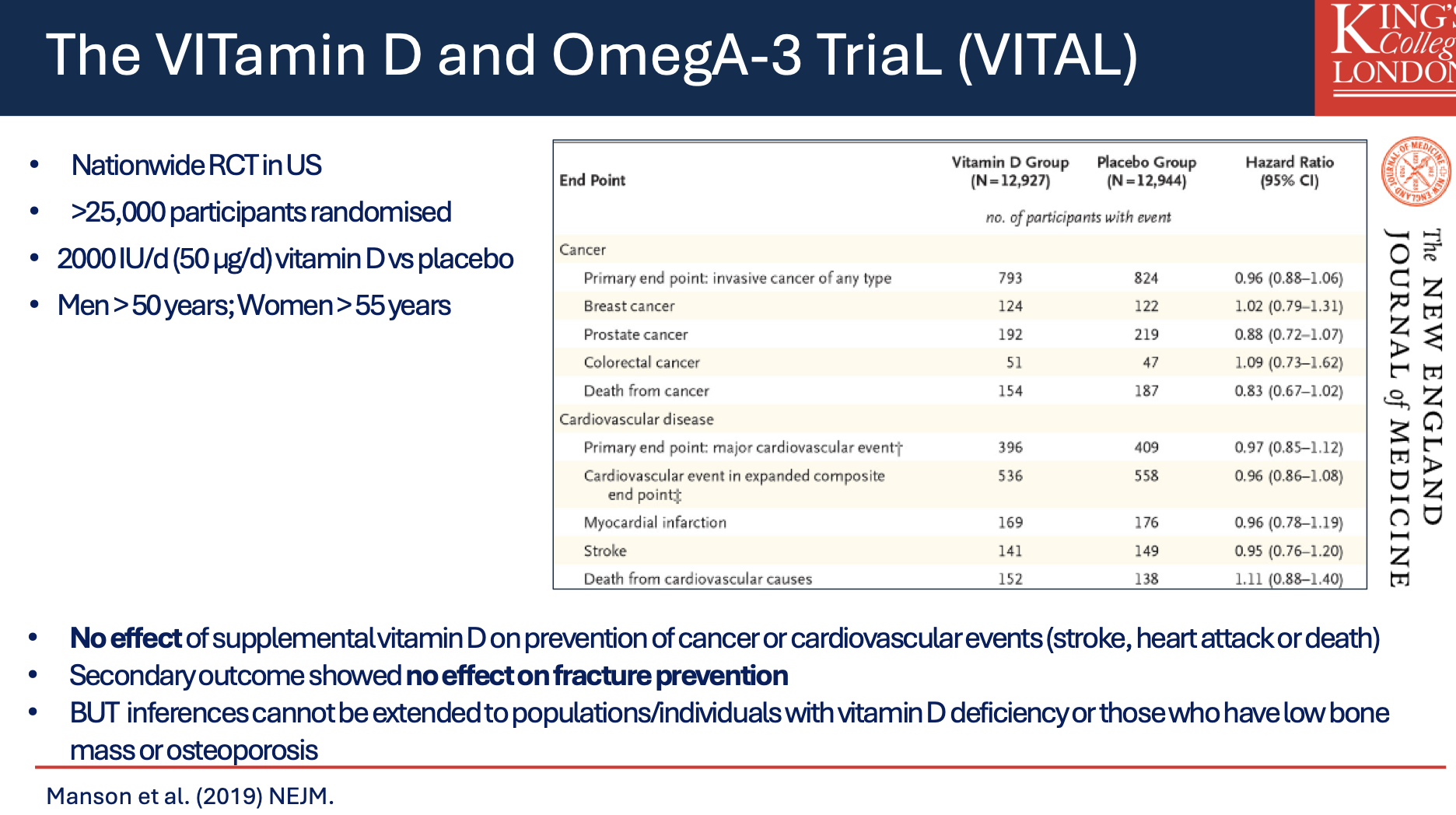
The VITamin D and OmegA-3 TriaL (VITAL)
A nationwide RCT conducted in the US involved >25,000 participants randomized to receive 2000 IU/d (50 µg/d) of vitamin D vs placebo.
Main findings indicated no effect on the prevention of cancer or cardiovascular events, with secondary outcomes showing no effect on fracture prevention.
Vitamin D and Immune Function
Mechanism: Regulation by synthesis of 1,25(OH)2D by macrophages and dendritic cells.
Antimicrobial Activity: 1,25(OH)2D regulates expression of antimicrobial proteins, enhancing immune responses.
Suppresses inflammatory T-cells and production of proinflammatory cytokines (IL-6, TNFα, IFN-γ).
Hepcidin (antibacterial protein); facilitates iron exportation from cells
Vitamin D and COVID-19
Observational evidence suggests lower 25(OH)D levels correlate with greater severity of COVID-19 symptoms.
The cause-effect relationship is confounded by shared risk factors for both vitamin D deficiency and COVID-19 severity.
Recommendations from NICE, PHN, and SACN included provision of free vitamin D supplements to vulnerable populations.
Media Coverage and Public Response
During the COVID-19 pandemic, significant misinformation regarding vitamin D and its association with COVID-19 circulated on social media.
CORONAVIT Trial
3-arm open-label RCT in the UK (Dec 2020 - Jun 2021) enrolled 6200 adults.
Participants with 25(OH)D < 75 nmol were randomized to receive either 20 µg/d or 80 µg/d of supplemental vitamin D or no intervention.
Findings: Increased 25(OH)D concentrations were observed, but no significant effect on acute respiratory infections or COVID-19 infection related risks.
Summary
Vitamin D deficiency is a global issue
Dietary and/or supplemental vitamin D is needed to meet year-round vitamin D requirements at Northern latitude
• Most well established role for vitamin D is in maintenance and development of the skeleton
• Role of vitamin D for many non-skeletal health outcomes is debated due to inadequately designed trials
Related Lectures
Bone Minerals: 7MNT0004 (semester 1)
Nutrition and Bone Health: 7MNT0003 (semester 2)
Content is complementary; integrated study suggested instead of silos learning.
Formative quiz is available on KEATS for self-directed learning.
Key References
Scientific Advisory Committee on Nutrition. Vitamin D and Health, 2016. Available at: SACN Report.
Manson et al. (2020). Principal results of the VITamin D and OmegA-3 TriaL (VITAL) and updated meta-analyses of relevant vitamin D trials. J Steroid Biochem Mol Biol.
National Institute for Health and Care Excellence. COVID-19 rapid guideline: vitamin D (nice.org.uk).
Jolliffee et al. (2022). Effect of a test-and-treat approach to vitamin D supplementation on risk of all-cause acute respiratory tract infection and COVID-19: Phase 3 randomized controlled trial (CORONAVIT). BMJ.