Drugs and Addiction
Marijuana
The Controversy with Marijuana
People fall into particular groups of thought regarding cannabis:
People who advocate for its medical use
People who advocate for its recreational use
People who warn against its potential harm
Much is being said in the news lately about marijuana, also known as weed, pot, or cannabis. There are those who advocate its use for medical purposes, those that advocate its use for recreational purposes, and those that warn of the potential harm in using marijuana. In Canada, marijuana is legal, and its recreational use is legal in several U.S. states with more states contemplating legalizing it. The truth is we do not know as much about marijuana as we would like to. Research has been stymied by strict regulations in the U.S. and Canada — preventing researchers from finding out more about it. It appears that that is about to change, as federal U.S. officials are starting to relax those restrictive laws.
Marijuana Use
Can be smoked
Can be eaten
Derived from cannabis sativa plant
THC is the active ingredient
Marijuana is a drug that is most often smoked, but it can be mixed in foods and eaten, such as in “pot brownies.” It is derived from the dried leaves of the cannabis sativa plant. One active ingredient in marijuana is THC or tetrahydrocannabinol.
THC is a Cannabinoid
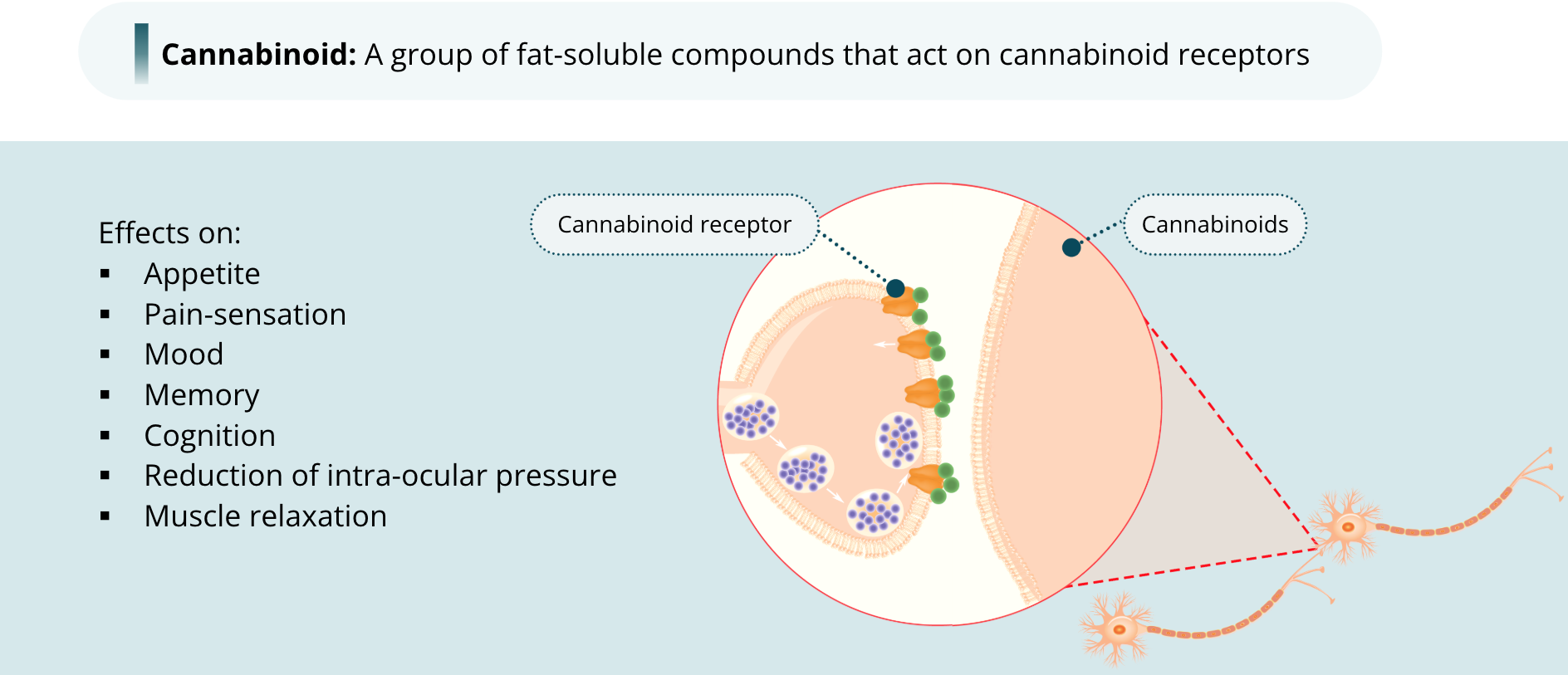
THC itself is a cannabinoid, a group of fat-soluble compounds that act on receptors called cannabinoid receptors. These receptors are located on the presynaptic terminals throughout the central nervous system, although they are also present in other tissues throughout the body. Because of their widespread distribution, it is unsurprising that THC has such a wide array of effects, including effects on appetite, pain-sensation, mood, memory, and cognition as well as reduction of intra-ocular pressure in the eye and muscle relaxation. We will come back to the effects in a moment. As most cannabinoid receptors in the brain are located on the presynaptic terminals, cannabinoids behave a little differently than the classical neurotransmitters. Endogenous cannabinoids in the brain act as retrograde messengers. That is, they are released by the postsynaptic neuron and bind to receptors on the presynaptic neuron. This is a sort of backwards signalling mechanism that regulates the release of neurotransmitters from the presynaptic neuron.
Marijuana is a Psychoactive Drug
Psychoactive drugs: Have many non-specific psychological effects
For Marijuana, this includes:
Euphoria
Enhancement of sensory perception
Relaxation
Stress reduction
Greater creativity
Marked distortions in the passage of time
Most people who use marijuana recreationally do so because of its psychoactive effects. Psychoactive drugs are those that have any non-specific psychological effects, from hallucinations, for example, to a calming effect. The psychoactive effects with marijuana use (in other words, the high) can include euphoria, enhancement of sensory perception (such as greater enjoyment of listening to music), relaxation, or stress reduction. Other reported effects are greater creativity or marked distortions in the passage of time. Of course, these psychoactive effects are very subjective and vary from person to person.
Marijuana is a Psychedelic Drug
Psychedelic drugs: cause perceptual distortions in the user
Because marijuana can produce distortions in sensory experiences, such as the passage of time or the appreciation of comedy, food, or music, it is considered a psychedelic drug. Psychedelic drugs are those that cause perceptual distortions in the user. Other commonly used psychedelic drugs include MDMA or Ecstasy, which is sometimes taken at all-night dance parties or raves, and LSD, which was more popular in the 1960s with the hippie movement than it is today.
Effects of Marijuana
Side Effects
Side effects: any effect that wasn’t the intended purpose of taking it
The most notable effects include:
Memory loss
Difficulty concentrating
Effects for people with less experience include:
Panic attacks
Paranoia
Physical short-term effects include:
Increased heart rate
Dry mouth
Red eyes
Marijuana also has side effects. A side effect of a drug is any effect that was not the intended purpose of taking it. Perhaps the most notable side effects with marijuana are memory loss and difficulty concentrating. In people with less experience with using the drug, it can produce panic attacks or paranoia. Some short-term physical side effects are increased heart rate, dry mouth, and the all-telling congestion of the conjunctival blood vessels — in other words, reddening of the eyes.
THC Actions in the Brain
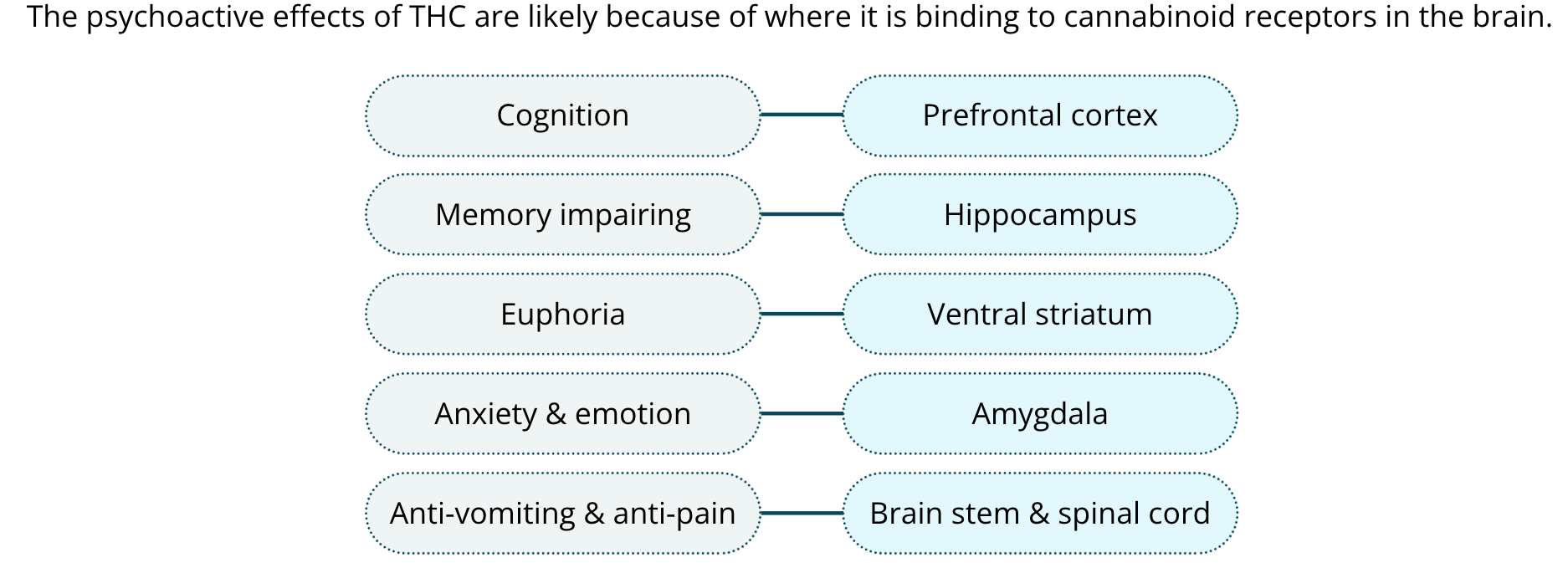
The psychoactive effects of THC are likely because of where it is binding to cannabinoid receptors in the brain. Its effects on cognition are likely due to it binding to receptors in the prefrontal cortex. Its memory impairing effects are thought to occur because of its actions in the hippocampus. The euphoric effects are likely due to it acting on receptors in the ventral striatum. The amygdala, as you know, is important for anxiety and emotion, so marijuana is likely having a calming effect by acting there. Its anti-vomiting and anti-pain effects are likely due to its actions in the brain stem and spinal cord. We still need more research to be sure.
Medicinal Effects
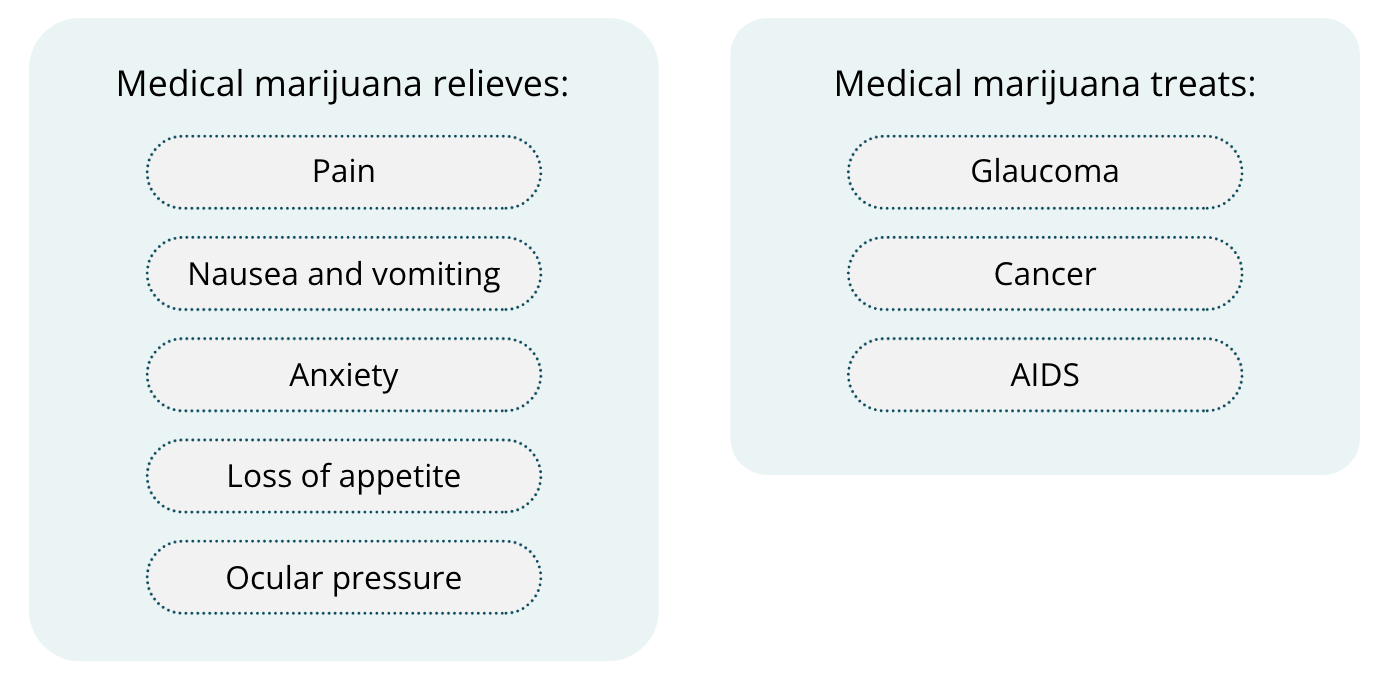
When used for medicinal purposes, medical marijuana is typically taken to relieve pain, nausea and vomiting, anxiety, and/or loss of appetite. Its ability to reduce ocular pressure makes it a good drug for treating glaucoma, a medical condition in which there is a buildup of pressure in the eye. It has also been shown to possibly have benefits in treating cancer or the side effects of cancer therapies, such as chemotherapy, which produces nausea and loss of appetite. THC can also be synthesized in the lab. Synthetic THC is sometimes prescribed to reduce vomiting and increase appetite in patients with AIDS.
Long-Term Use
Recent studies found a correlation between reduced hippocampus size and heavy marijuana use, however it is correlational data only
Correlational data: it is not known if marijuana use decreased the volume of the hippocampus or if people who have a smaller hippocampus are more likely to use marijuana
There have been only a handful of studies that examine the long-term consequences of regular marijuana use. Recent studies suggest that the effects may be greater than once thought. Heavy users have been shown to have abnormalities in their brains, such as reduced hippocampus size. It is important to point out that these data are correlational — meaning that we do not know if marijuana use decreased the volume of the hippocampus or if people who have a smaller hippocampus are more likely to use marijuana.
Research on Marijuana
The bottom line is, there really is not that much concrete research out there. There are parents who claim that marijuana reduces the number of seizures in their child; there are others who claim it helps with a wide variety of disorders. We will have to wait until more research is conducted. Considering that marijuana has been around for so long, you would think we would know more about it. But as I mentioned, government restrictions have prevented scientists from doing much study on it. With the legalization in many states, that is starting to change. With more data, we will eventually determine which medical conditions may benefit from it, and what, if any, negative long-term consequences of marijuana use are.
Cocaine
Coca-Cola and Cocaine
On a hot summer day, you may be like me and really enjoy drinking an icy-cold CocaCola. Sometimes, it feels like there must be something addictive in it. Well, there is not anymore, but that was not always the case.
Back in 1885, when the developers of the soft drink were thinking up a brand name, they decided on the name Coca-Cola, because of its two “medicinal” ingredients: an extract from coca leaves and kola nuts. Why is this historical ditty interesting? Cocaine is what is extracted from coca leaves, and, in the early years, Coca-Cola certainly contained it, although how much exactly was in there is hard to determine now. CocaCola became “cocaine free” in 1929. In the early 20th century, it was not uncommon for patent medicines to contain cocaine, and when Coca-Cola was developed, it was initially marketed as a medicine.
Cocaine is a Stimulant Drug
Cocaine has some of the following effects:
Produces euphoria
Decreases appetite
Increases alertness
Relieves fatigue
Stimulant drugs: Activate the central nervous system to produce arousal, increase alertness, and elevate mood
Cocaine produces euphoria, decreases appetite, increases alertness, and relieves fatigue. Because it increases mood and alertness, cocaine is considered a stimulant. Stimulant drugs activate the central nervous system to produce arousal, increase alertness, and elevate mood. Another stimulant drug is amphetamine, also known as speed, which acts in a similar way to cocaine. Cocaine was typically taken in its white powder form and snorted up the nose where it is absorbed into the bloodstream from the nasal passages. Another pure form of cocaine was developed, called free base, which, in solid form, can be smoked. Powdered cocaine can also be dissolved and injected. These forms of cocaine were historically expensive, and in the 1970s, cocaine was considered the fashionable drug for businesspeople and famous people in the movie and music industries. It was the rich man’s drug.
The Emergence of Crack Cocaine
Eventually, a cruder and less expensive way to process cocaine in its solid form emerged. This version is less pure, although the smoke from it contains pure cocaine, and because it was less expensive, crack cocaine became more widely accessible and affordable — it is also the most addictive form of cocaine. By the 1980s, crack cocaine use was reaching epidemic levels in impoverished neighbourhoods in the U.S. In a single decade, cocaine was no longer associated with being wealthy and successful; it was associated with poverty, crime, and death.
Effects of Cocaine
What Actions it has on the Brain
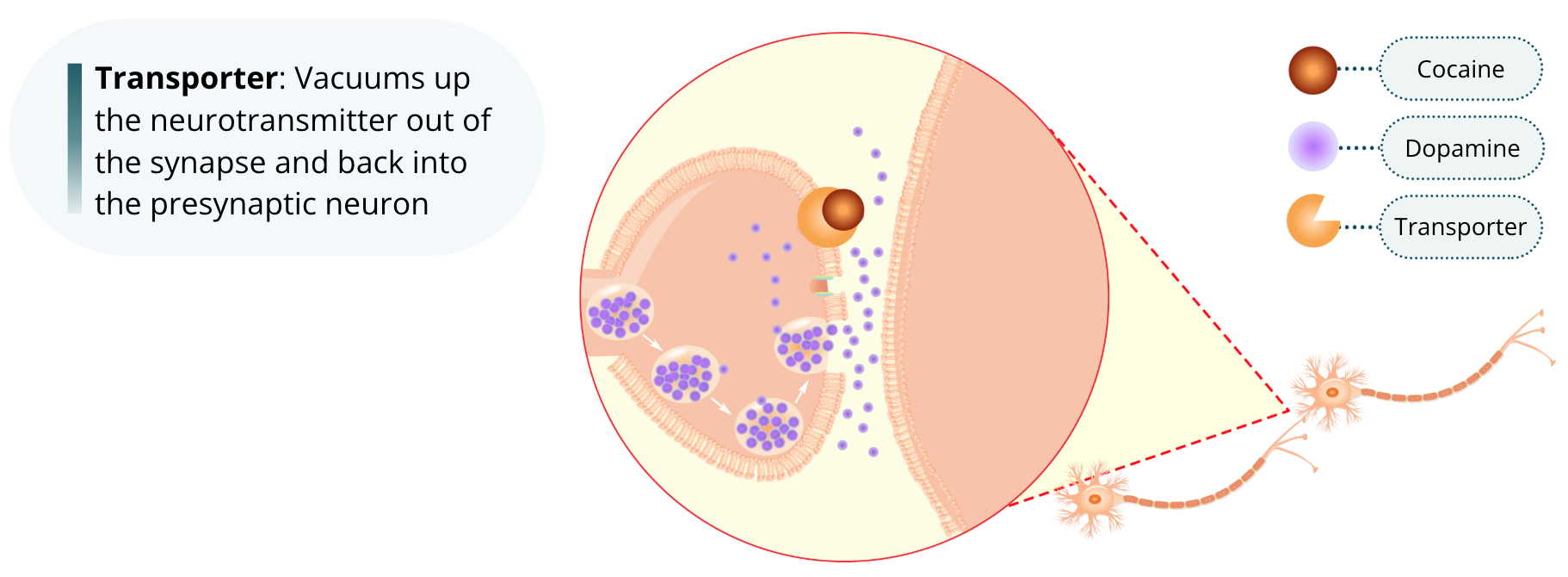
When a neurotransmitter is released into the synapse, it signals the next neuron by binding to the postsynaptic receptor and having an effect on that neuron. This signal can be terminated by removing the neurotransmitter from the synapse. For some neurons, this is achieved using transporters, which basically vacuum up the neurotransmitter out of the synaptic cleft and back into the presynaptic neuron. Cocaine acts by binding to the dopamine and serotonin transporters. By binding to them, it effectively blocks their function. In so doing, cocaine extends the life of these neurotransmitters within the synapse and thereby increases their transmission signal.
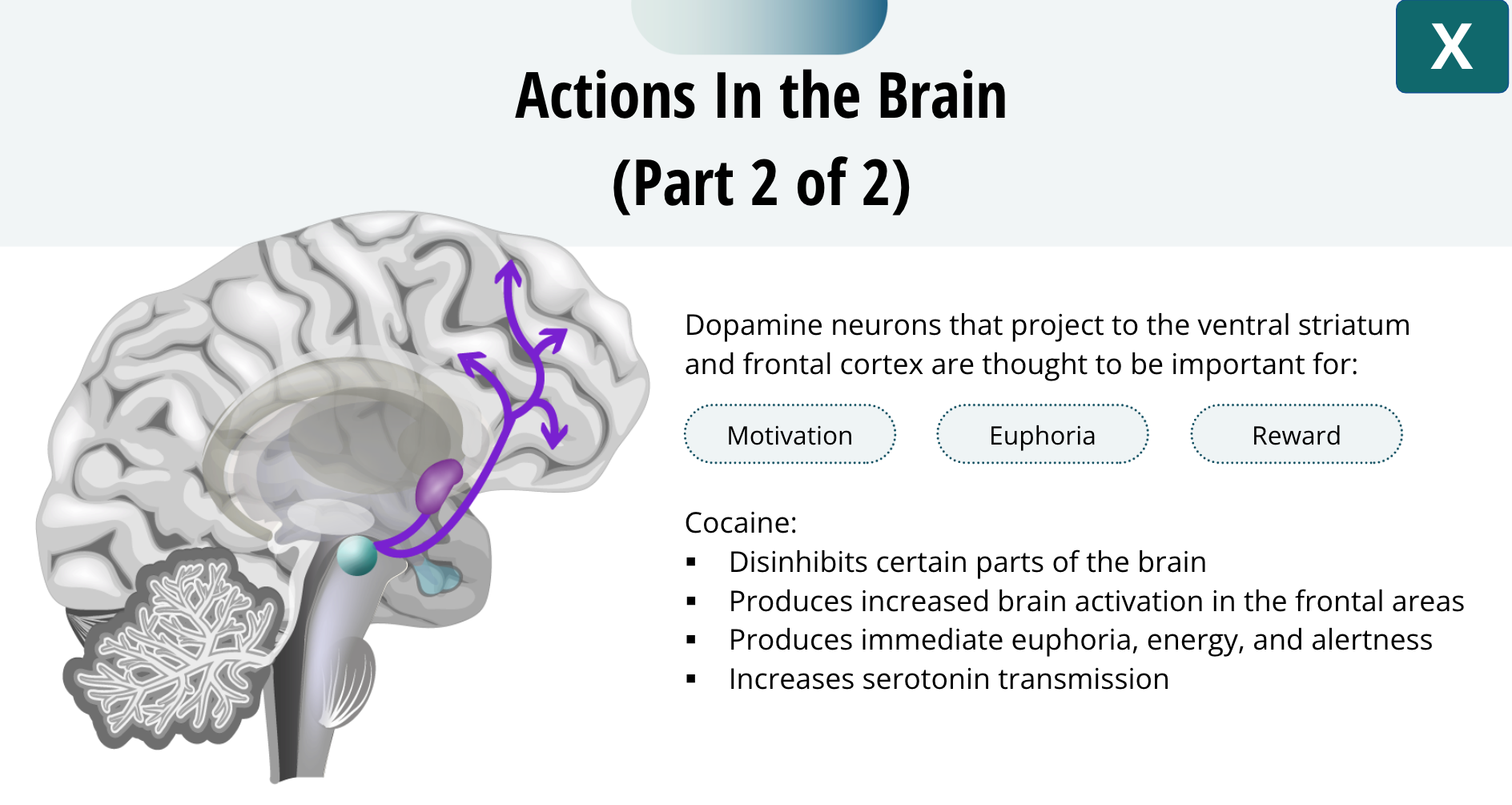
Dopamine neurons that project to the ventral striatum and frontal cortex are thought to be important for:
Feelings of euphoria
Motivation
Reward (although dopamine ≠ reward)
These dopamine neurons are certainly important for addiction, as we will learn. It is thought that cocaine’s euphoric effects come from dopamine’s ability to prevent the cortex from inhibiting other brain structures. Thus, cocaine disinhibits certain parts of the brain. All drugs that cause euphoria will produce increased brain activation in the frontal areas. Snorting or smoking cocaine will produce immediate euphoria, energy, and alertness, adding to its addictive properties. It is thought that the feelings of happiness and well-being, that also come from cocaine, come from it increasing serotonin transmission.
Side Effects
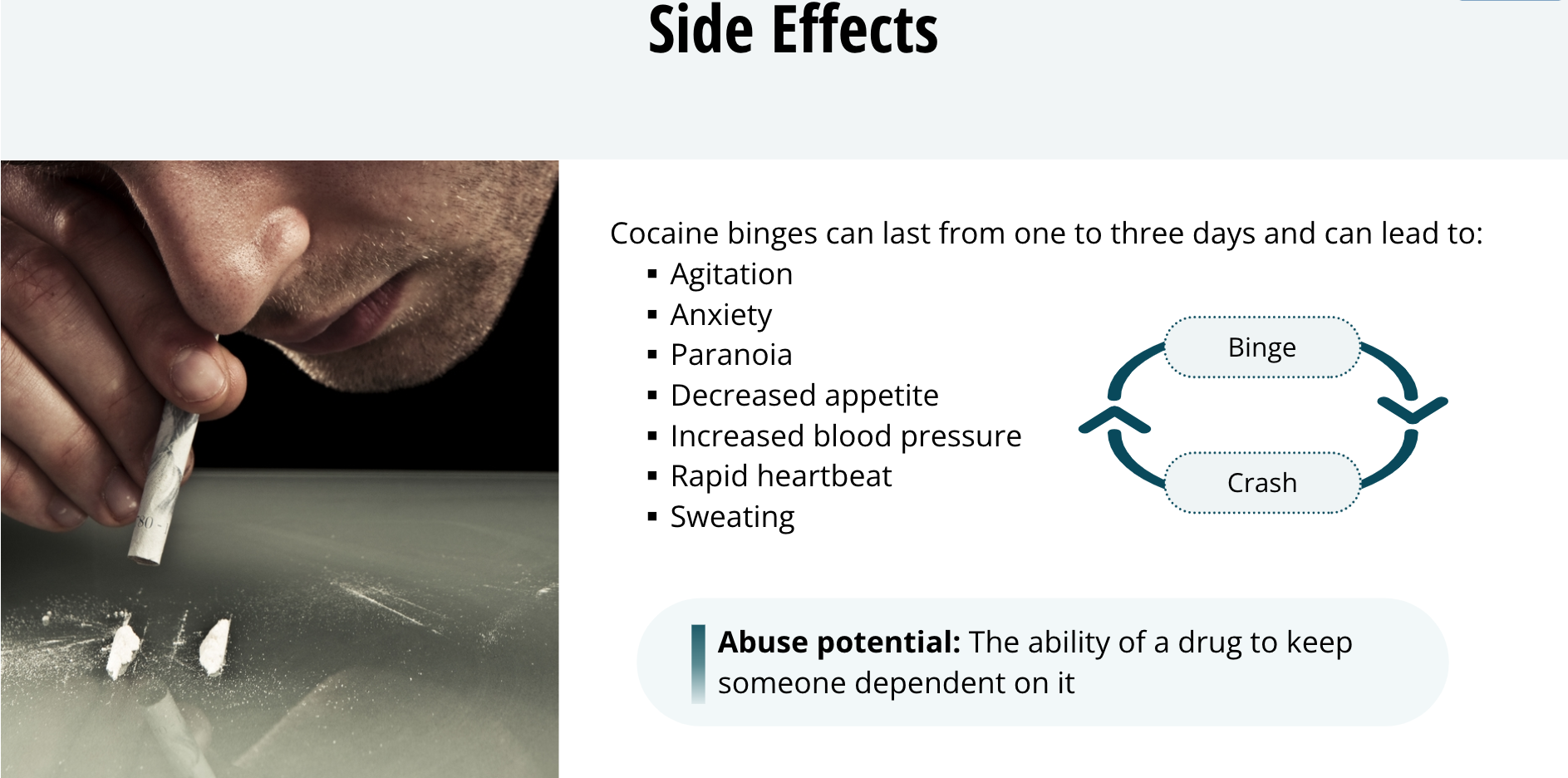
Cocaine is often taken repeatedly to extend the euphoric effects and ward off the withdrawal effects. This is called a cocaine binge. Cocaine binges can last from one to three days and can lead to agitation, anxiety, paranoia, and decreased appetite. Other side effects include increased blood pressure, rapid heartbeat, and sweating. After a cocaine binge, the user crashes, typically suffering from depression, anxiety, boredom, a lack of pleasure, and a craving for more cocaine. This cycle of the euphoric high followed by mild dysphoric withdrawal and a craving for more cocaine is thought to contribute to its high abuse potential. Abuse potential is the ability of a drug to keep someone dependent on it: basically, how addictive it is.
Long-Term Use
Impairments in:
Memory
Executive functions
Impulse control and decision-making
Associated with:
Reduced activity in prefrontal cortex
Reduced grey matter in:
Prefrontal area
Temporal lobe
Long-term cocaine users have impairments in memory and executive functions, including impulse-control and decision-making. These impairments are associated with reduced activity in the prefrontal cortex and reduced gray matter in the prefrontal and temporal lobe areas.
Alcohol
Alcohol Comes from Fermentation
In the fall, in Canada, you might sometimes see birds flying into buildings, or not quite getting that landing right. People who study birds suggest that a number of them are intoxicated from eating berries. Alcohol forms in berries as they ferment after the first frost, and birds that feed on winter berries can get tipsy. Alcohol, or specifically ethanol, is probably the oldest abused drug. Primitive societies probably discovered its effects upon eating fermented fruits or grains. During the fermentation process, yeasts convert the sugars in plants into energy, and ethanol is a byproduct. Thus, Mother Nature gives us alcohol naturally.
Alcohol
Well known effects include:
Evokes euphoria, reduction of anxiety, relaxation
Side effects include:
Motor incoordination
Poor judgement
Cognitive impairments
In lower doses:
Acts as a stimulant
Is a social lubricant
In higher doses:
Has a sedative effect
Induces relaxation, sleep and/or unconsciousness
Alcohol acts on many different brain regions to evoke euphoria, reduction of anxiety, and relaxation. Some of its side effects include motor incoordination, poor judgment, and cognitive impairments. Most people who drink alcohol value it as a social lubricant taking the edge off in social situations, like meeting people at a party or at a bar. At lower doses, it acts as a stimulant, increasing social interactions. As the amount of alcohol consumed increases, an opposite sedative effect occurs in which its effects go from being relaxing to inducing sleep or unconsciousness.
Alcohol is a Depressant Drug
Depressant drugs: reduces activity in the central nervous system
Includes sedatives (drugs that induce calm or sleep)
Barbituates
Includes anxiolytics (drugs that reduce anxiety)
Benzodiazepines (like valium)
Because of its sedative qualities, alcohol is considered to be a depressant drug. Depressants are drugs that reduce activity in the central nervous system which may lead to a calming effect, a reduction in anxiety, or even induce sleep. Some other examples of depressants are sedatives (meaning inducing calm or sleep), such as barbiturates and a class of anxiolytic drugs (meaning anxiety reducing) called benzodiazepines. An example of a benzodiazepine is Valium.
Effects of Alcohol
Alcohol Actions in the Brain
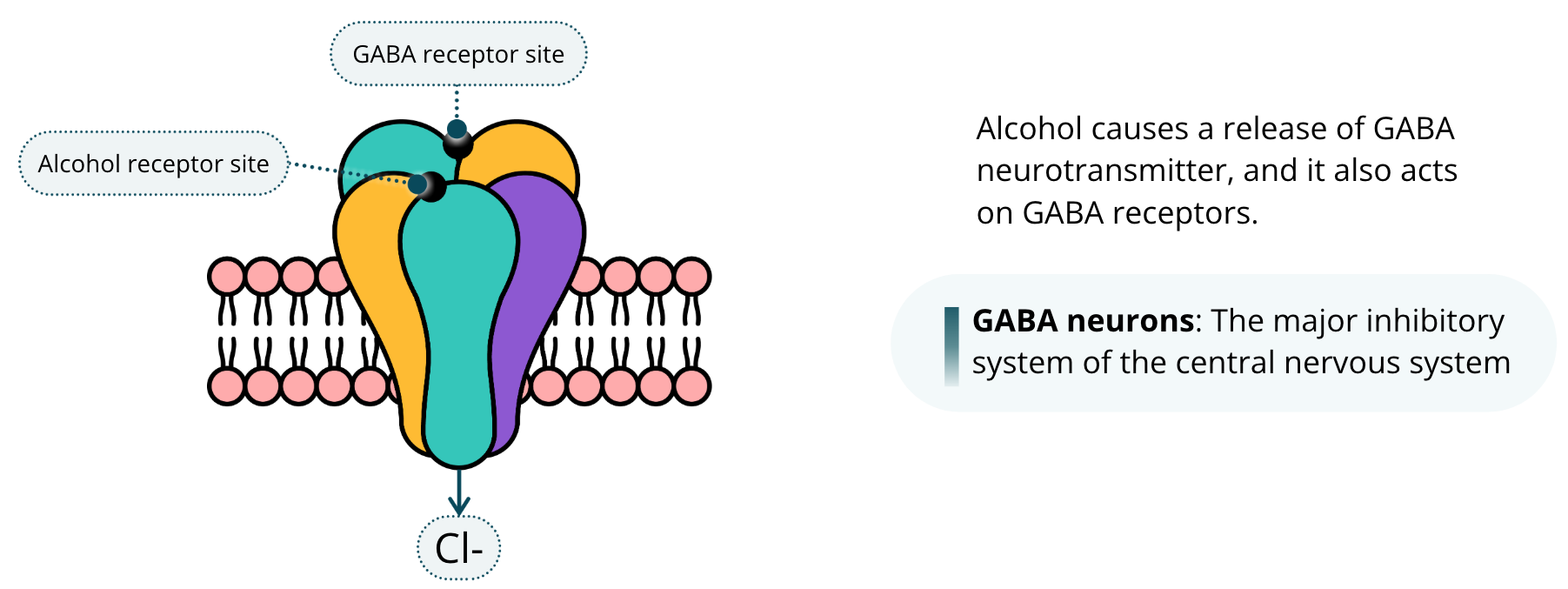
The effects of alcohol on the brain are very complex, and we have not gotten that one fully figured out yet despite decades of research. What we do know is that alcohol causes a release of GABA neurotransmitter, and it also acts on GABA receptors. Given that alcohol is a depressant, this should not come as a surprise because, as you now know, GABA neurons are the major inhibitory system of the central nervous system.
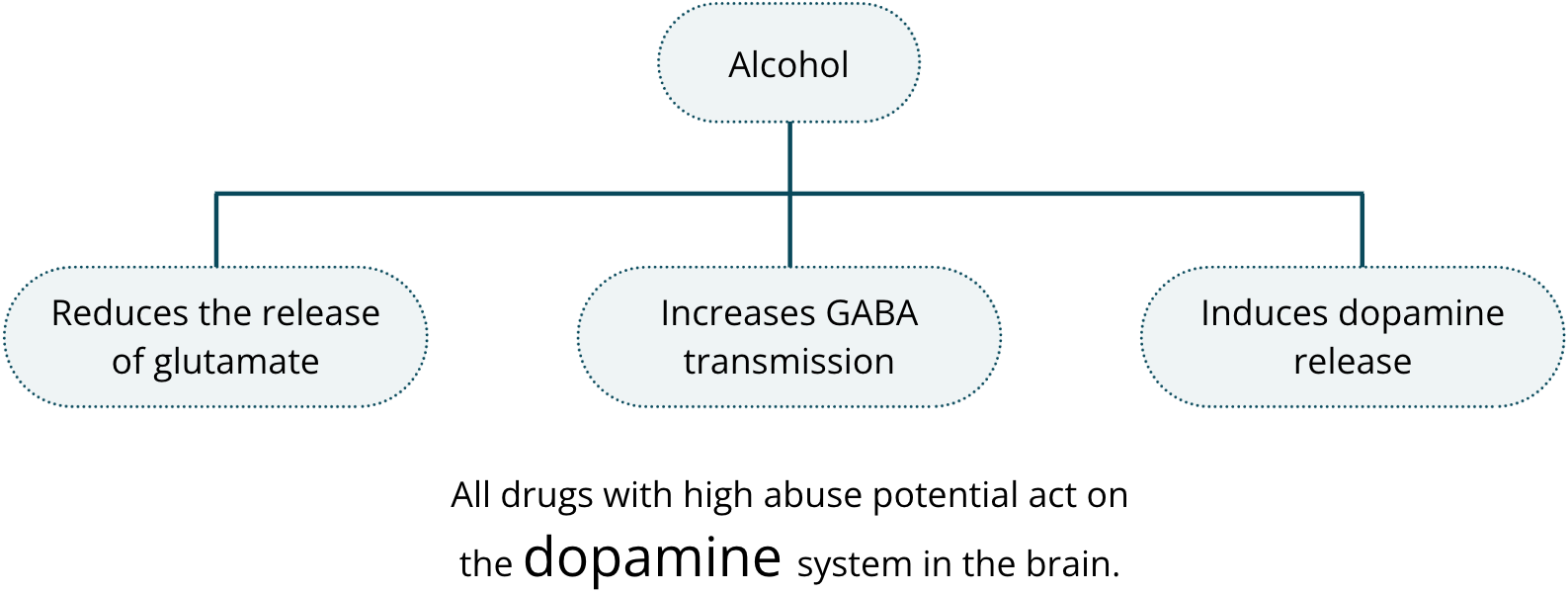
Alcohol also reduces the release of glutamate, which is the major excitatory neurotransmitter in the brain. It is thought that alcohol produces its sedative and anxiolytic effects as well as inhibiting motor skills by both reducing glutamate transmission while simultaneously increasing GABA transmission. Alcohol is thought to produce its euphoric affects by also acting on certain pathways in the brain to ultimately induce dopamine release. As you are probably beginning to figure out by now, all drugs with high abuse potential act on the dopamine system in the brain.
Side Effects
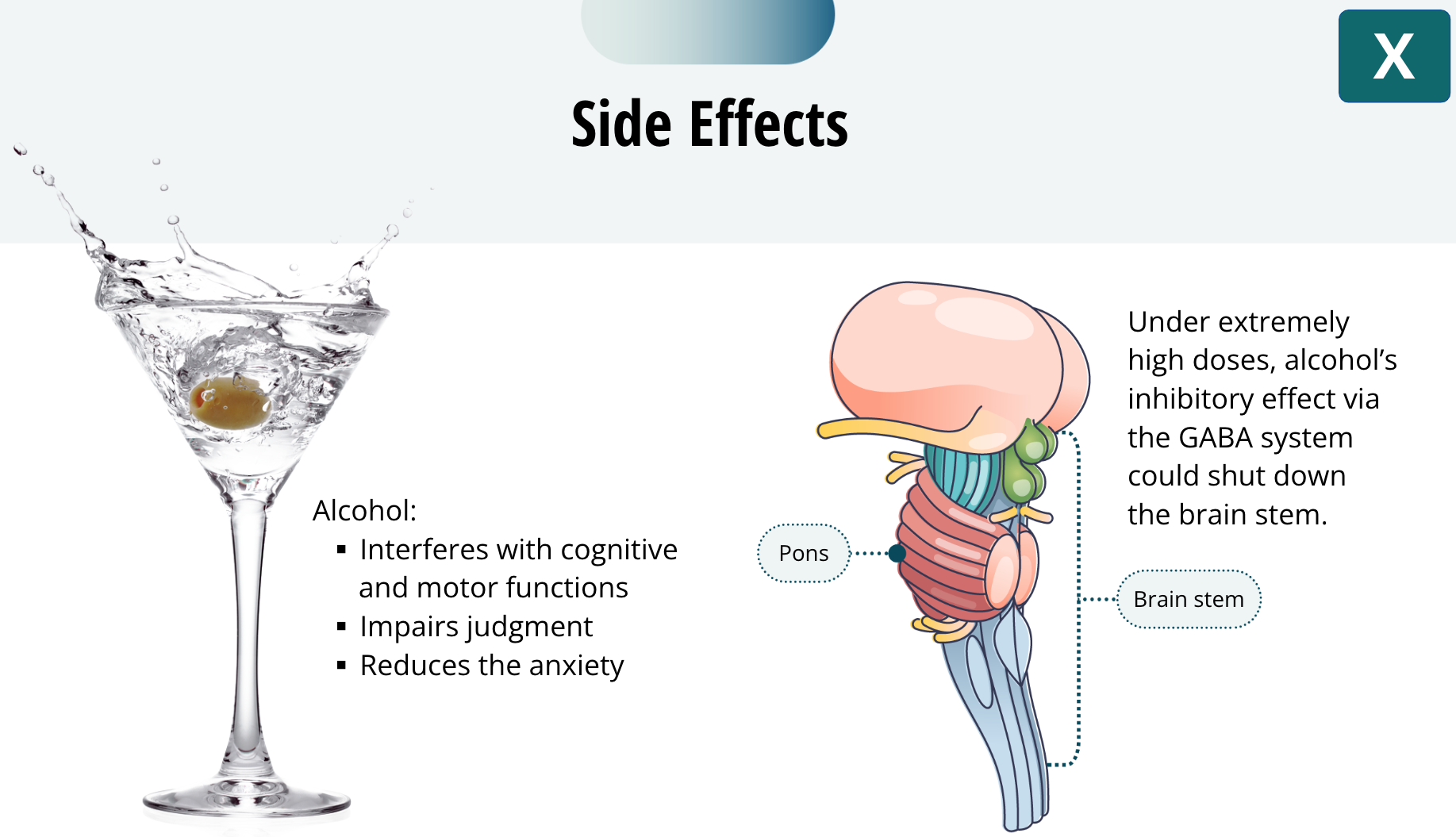
As mentioned, alcohol has side effects including interference with cognitive and motor functions as well as impairing judgment. This explains why alcohol is involved with a third of all traffic fatalities and over a third of all violent crimes. In addition to impairing judgment, alcohol also reduces the anxiety that would normally cause people to avoid aggression or aggressive situations. In other words, intoxicated people can become aggressive in ways that gets them in trouble, whereas sober people would avoid such situations. Under extremely high doses, alcohol’s inhibitory effect via the GABA system could shut down the brain stem. As you have learned, the brain stem contains the pons, which contains the reticular formation, which is vital for sleep and arousal. Shutting down this part of the brain, which could happen when consuming too much alcohol, would result in coma or even death. I am talking about very high doses here, not simply a few beers.
Long-Term Use
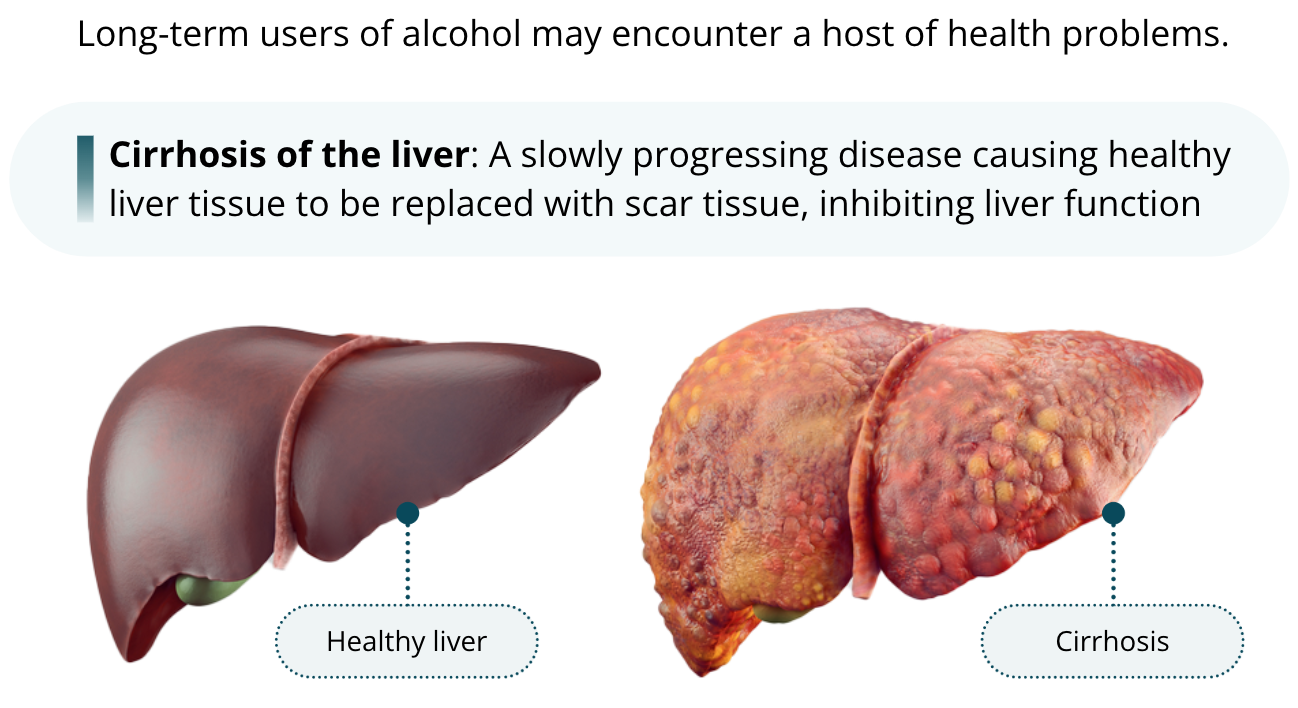
Long-term users of alcohol may encounter a host of health problems. One common side effect of chronic alcoholism is a condition called cirrhosis of the liver. This slowly progressing disease causes healthy liver tissue to be replaced with scar tissue, inhibiting liver function. In extreme cases, this disease can be fatal.
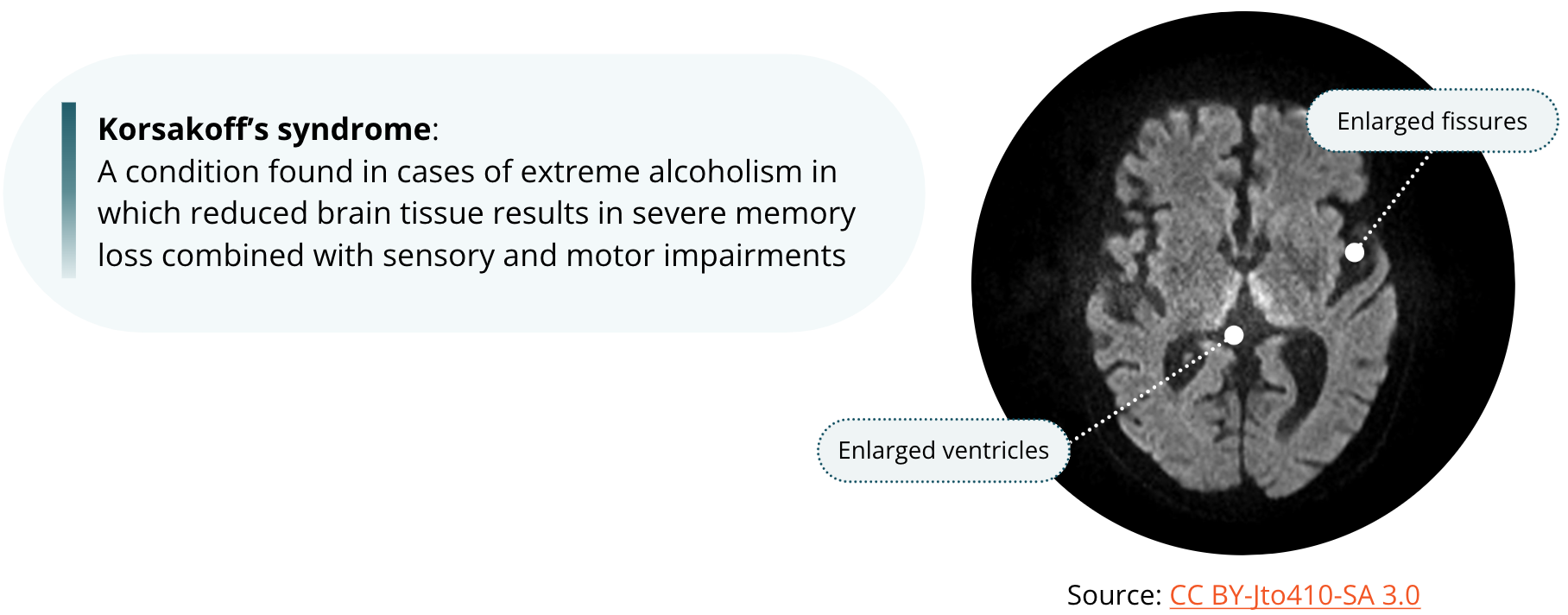
Chronic alcoholism can lead to a type of brain damage called Korsakoff’s syndrome. This is a condition found in cases of extreme alcoholism in which reduced brain tissue, results in severe memory loss combined with sensory and motor impairments. It was originally thought that alcohol directly causes such brain damage. Now it is believed that the condition arises from the malnutrition and vitamin deficiency that sometimes can accompany severe alcoholism.
Alcohol Withdrawal
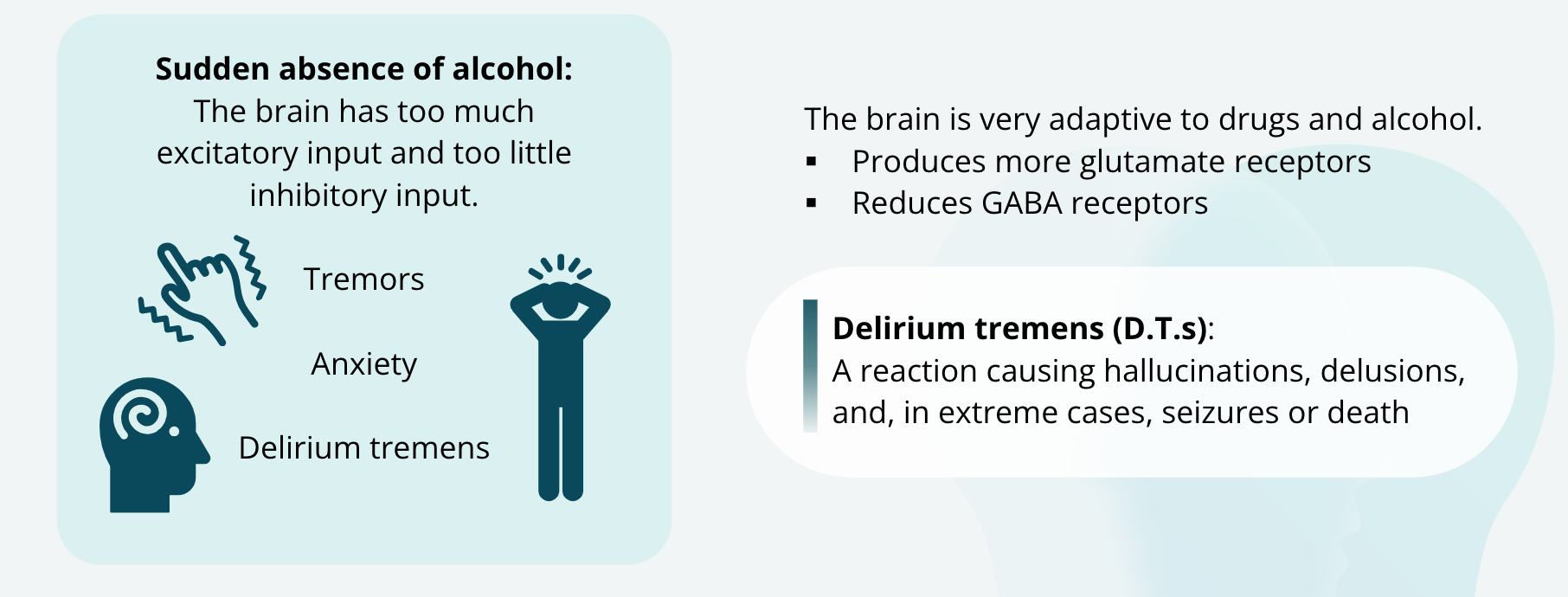
The brain is very adaptive to whatever we throw its way, including drugs and alcohol. In severe alcoholism, the glutamate and GABA receptors adapt, such that, given the inhibition of glutamate release with repeated alcohol, the brain produces more glutamate receptors to compensate. Likewise, given the excess of GABA release in the presence of alcohol, the brain reduces GABA receptors. Because of these adaptations, it can be very dangerous for chronic alcoholics to abruptly stop drinking. In the sudden absence of alcohol, the brain now has too much excitatory input and too little inhibitory input. Alcohol withdrawal can lead to tremors, anxiety, and a more serious reaction called delirium tremens, also called the D.T.s. The D.T.s consist of hallucinations, delusions, and, in extreme cases, seizures or death. For this reason, severe alcoholics must first enter a medically supervised detox program prior to beginning rehab therapy.
Summary
So, the next time you see birds in the trees in the fall trying to fatten up for the long flight south for the winter, just remember you do not have to feel too sorry for them, or maybe you should feel more sorry for them, for they are probably drunk.
Addiction
Drug Addiction is More Complicated than Pleasure and Withdrawal
Theory 1: using a drug is pleasurable
Reports that the drug doesn’t produce pleasure, but users still addicted
Theory 2: using a drug avoids the effects of withdrawal
Doesn’t explain what led to addiction in the first place
Doesn’t explain relapse following the end of withdrawal symptoms
The addictiveness of a drug isn’t related to its withdrawal symptoms
Drug addiction is more complicated than most people think. It was believed that addiction occurred simply because using a drug is pleasurable. However, many addicts report that they do not even enjoy the drug anymore, yet they still feel helpless to stop. Another theory was that people continue to abuse drugs because they wish to avoid the effects of drug withdrawal. This idea has several flaws. For one, it does not explain how people came to be addicted in the first place. And secondly, it does not explain why people who have quit using a drug for a long time — years even — will relapse long after the withdrawal symptoms have gone away. Moreover, the addictiveness of a drug is not related to its withdrawal symptoms. While both the pleasure derived from using a drug and the withdrawal experienced with its cessation probably both contribute to continued use, drug addiction is likely more complicated than just these two factors.
Treatment of Drug Addiction
Understanding addiction in the brain has been the focus of much research funding, and therefore, there are many researchers looking into it. We now understand quite a bit more about addiction and the brain, although we are not even close to a cure per se. In fact, Alcoholics Anonymous (or AA) and its related organizations, such as Narcotics Anonymous, are very effective at helping addicts to stop using, and they do not use modern science to help people out. That does not mean that we should stop trying to understand the brain and behaviour of addiction; it simply means we have not found a cure yet through science.
The Dopamine Hypothesis
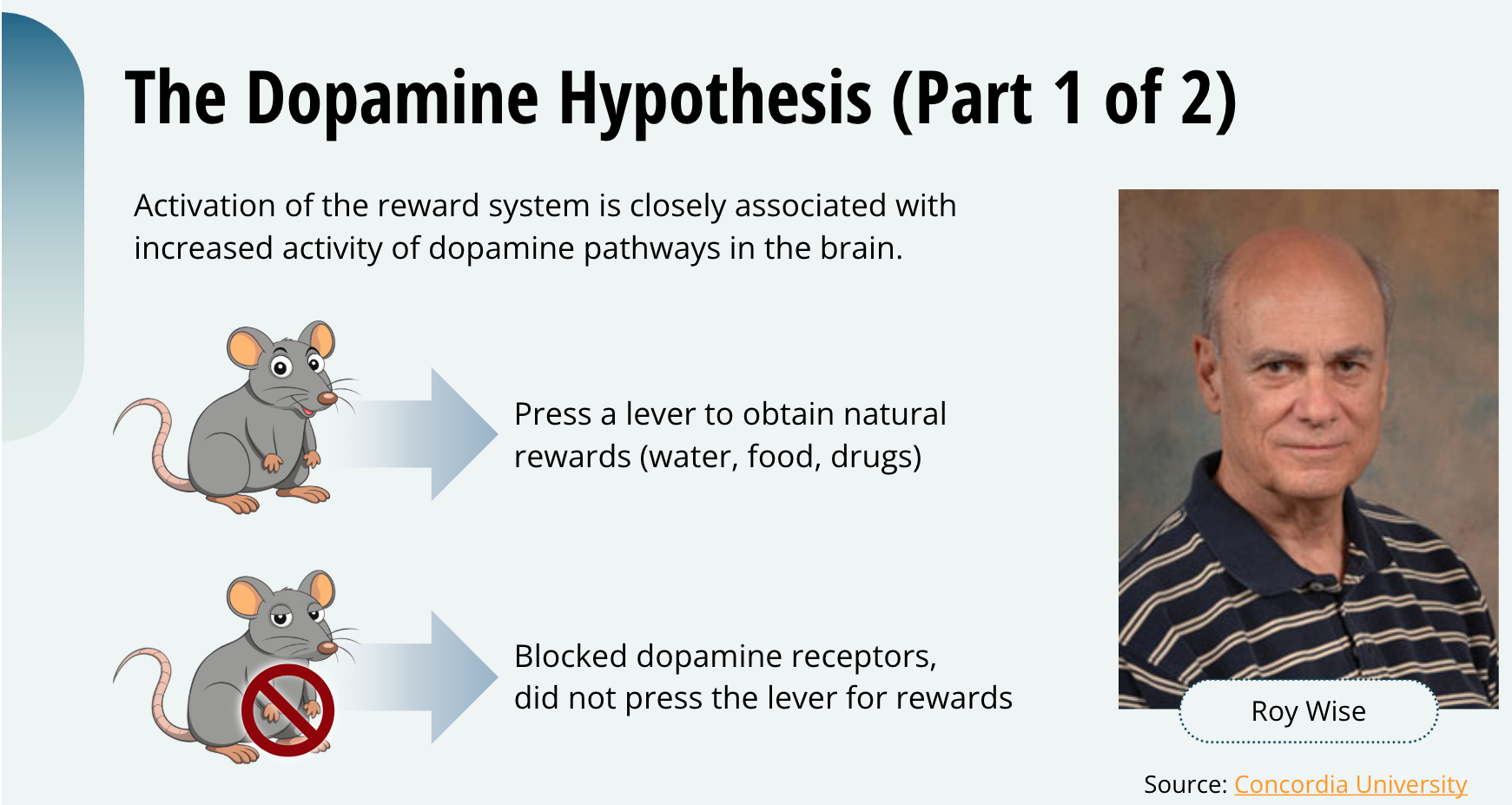
Early research by Roy Wise here in Montreal (in fact, here at Concordia University) led to the dopamine hypothesis of reward. Wise suggested that activation of the reward system is closely associated with increased activity of dopamine pathways in the brain. Wise and his colleagues showed that rats will press a lever to obtain natural rewards, such as water for thirsty rats and food for hungry ones, as well as for drugs with high abuse potential. However, when he gave the rats drugs that blocked dopamine receptors, they no longer pressed the lever for the reward.
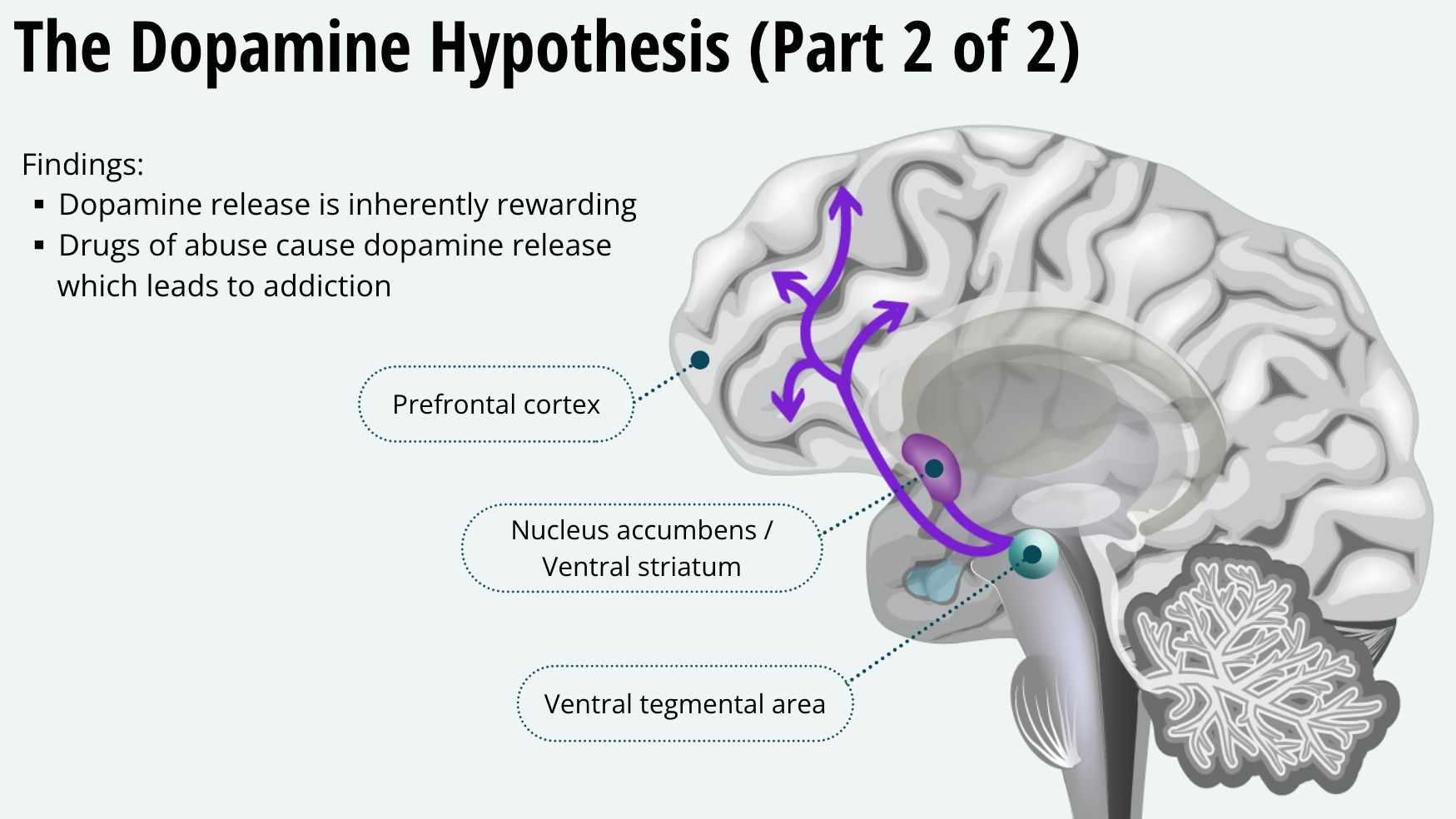
Specifically, Wise, and others since, showed that the mesocorticolimbic dopamine pathway in the brain is important for addiction. This system is comprised of dopamine neurons whose cell bodies are located in the ventral tegmental area, and whose axon terminals project to the ventral striatum and prefrontal cortex. Another name for the ventral striatum is the nucleus accumbens, which is what it is labelled in this figure. Remember this, the ventral striatum and the nucleus accumbens are the same brain area — they just have two different names. Rats will press a lever to receive drugs within these brain areas, and when pressing a lever to get a general reward, dopamine is released in the ventral striatum. These data lead Wise to suggest that dopamine release is inherently rewarding, and the fact that drugs of abuse cause dopamine release leads to addiction.
Dopamine is not the Whole Story
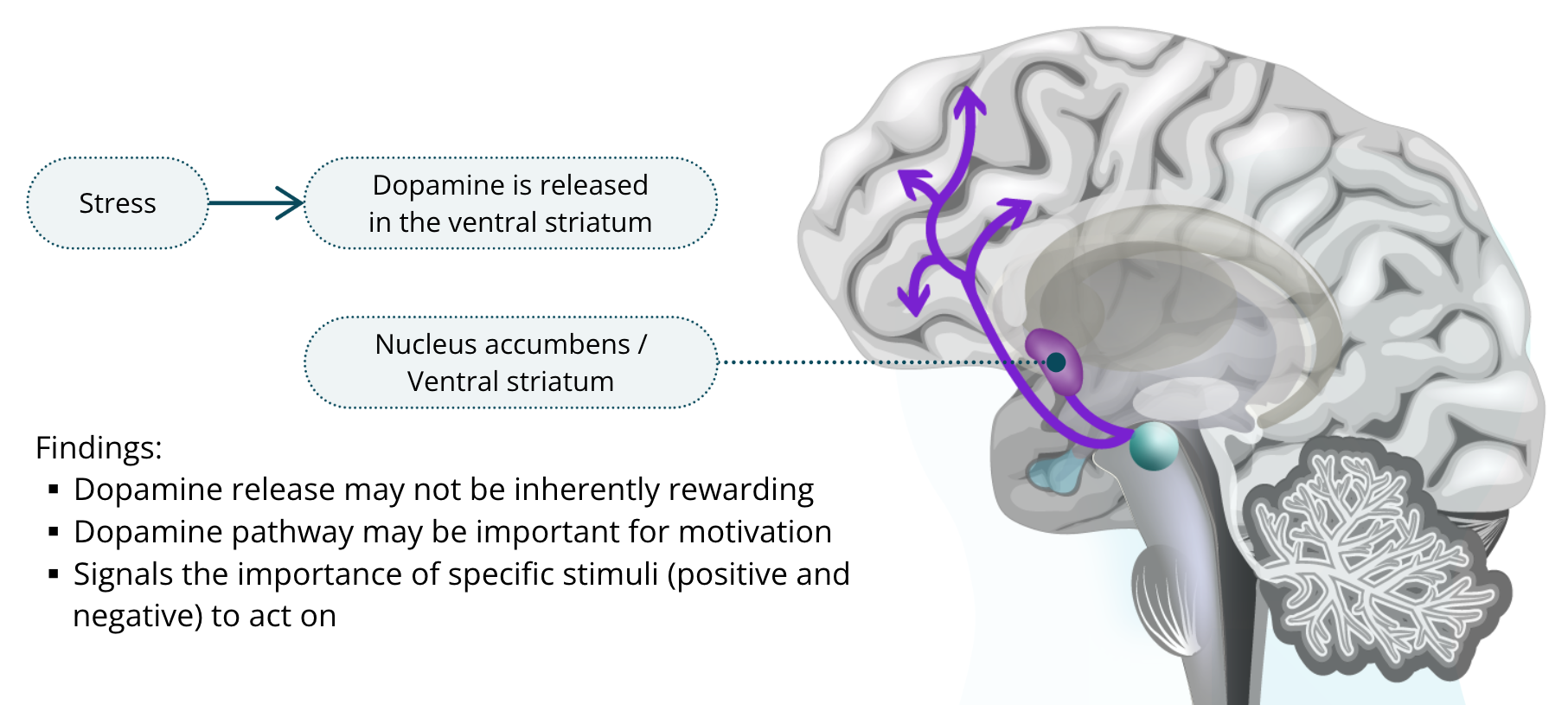
Not everyone agrees or thinks that addiction is that simple. For example, if you stress a rat, like presenting it with the odour of one of its predators, such as the smell of cat urine, dopamine is also released in the ventral striatum. This shows that dopamine release may not be inherently rewarding. It has been suggested that this dopamine pathway may be important for motivation. That is, it signals the importance of specific stimuli we encounter and need to act on, both those that are rewarding and those that are aversive.
Stages of Addiction
Early Stage of Addiction
Mesocorticolimbic dopamine is very important for early drug taking
Nearly all drugs of abuse can an ↑ in dopamine in the ventral striatum
Regardless of whether or not mesocorticolimbic dopamine represents reward in the brain, we do know that it is very important for early drug taking. Almost all drugs of abuse cause an increase in dopamine release in the ventral striatum. It has also been shown that among volunteers who took drugs in a brain scanner, those who reported the most intense highs also had the most dopamine in the ventral striatum.
Late Stage of Addiction
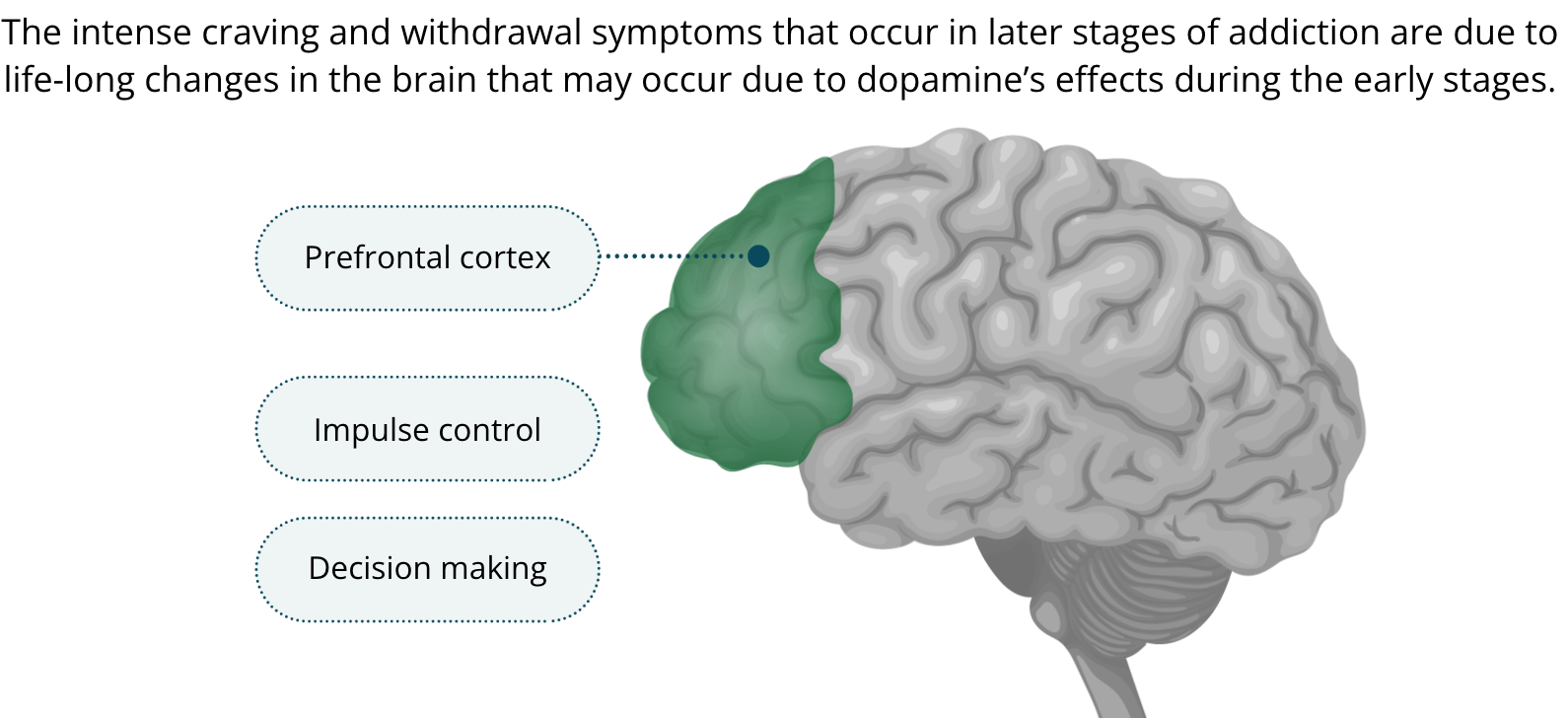
It is now thought that the intense craving and withdrawal symptoms that occur in later stages of addiction are due to life-long changes in the brain that may occur due to dopamine’s effects during the early stages. It is also thought that changes in the prefrontal cortex may be involved in addiction. As you have learned, the prefrontal cortex is important for impulse control and decision making. It has been theorized that disrupted prefrontal functioning could account for the addict’s impaired judgment and decision making. Moreover, it could account for the addict’s loss of control over his or her behaviour, even when wanting to abstain from taking drugs.
Going From Controlled Drug Use to Compulsive Addiction
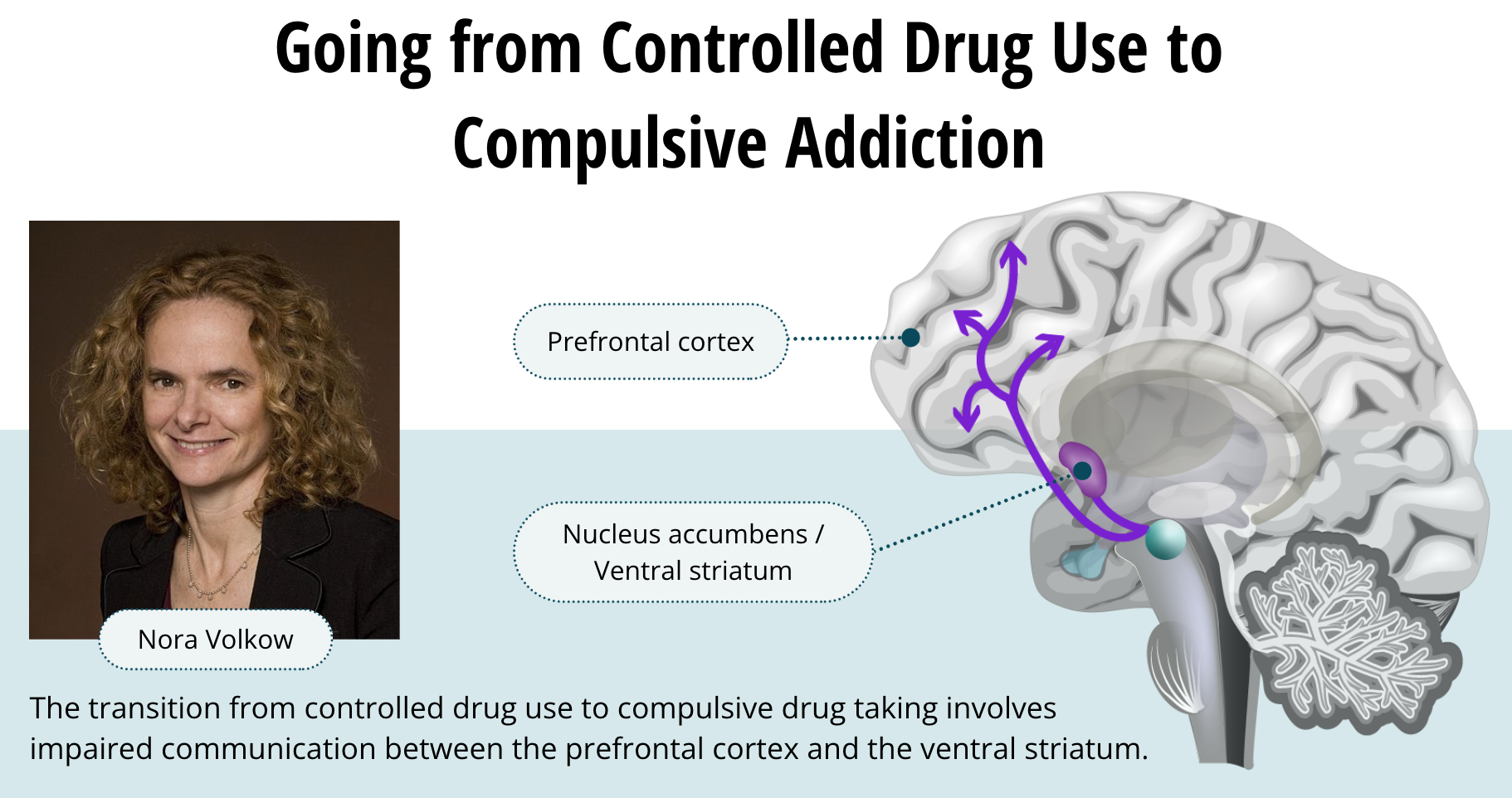
Nora Volkow, who is the director of the National Institute on Drug Abuse in the U.S., and a scientist conducting much of this research, suggests that the transition from controlled drug use to compulsive drug taking involves impaired communication between the prefrontal cortex and the ventral striatum. According to this idea, a person returns to drug taking when stress or another trigger increases dopamine in the prefrontal cortex and glutamate in the ventral striatum. Increased dopamine in the prefrontal cortex produces a compulsive focus on drugs while increased excitability in the ventral striatum from glutamate increases the motivation to seek out the drug. This idea seems to best fit the available data, but we have more research to do before we fully understand the complexities of addiction.