general anesthetics
Local anesthetics acts locally to block nerve conduction (lignocaine) while general anesthetics act in the brain to cause loss of consciousness. Both are used for operations and experimentally. There are two major types of general anesthetics: inhalation through gases and IV infusion
Anesthesia causes three main neuro physical changes:
unconsciousness
loss of response to painful stimuli (analgesia)
loss of reflexes
The first anesthetic was ether which was used in 1846 followed by nitric oxide which was discovered as a general anesthetic in 1844. Before this, alcohol was used to induce anesthesia but you needed to drink a lot and it did not come around very quickly. In some cases, opium was also used as an analgesic
General anesthetics have a wide variety of chemical structures meaning that there is no strict structure activity relationship: 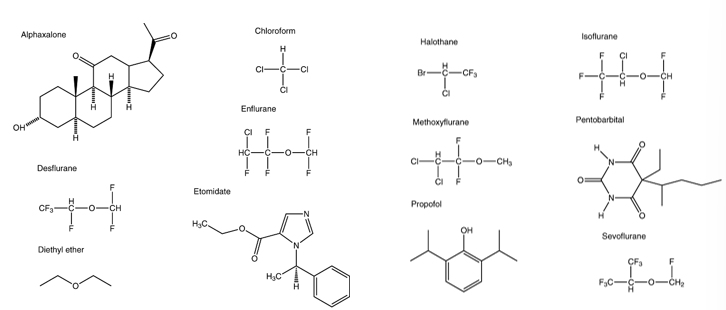
stages of anesthesia
stage 1
still awake but drowsy
distorted perception
at the end of the stage, analgesia is acquired
this is useful for obstetrics which uses gas and air.
breathing is normal and there is no significant respiratory depression
stage 2
loss of consciousness
inhibition depressed before motor centres - exaggerated reflexes such as vomiting
stimulation of CNS which leads to uncontrolled movements and vocalisations
loss of temperature control - flushing of skin
irregular breathing and cardiac dysrhythmia
This stage is dangerous so you need to move through it as quick as possible
stage 3
This is surgical anesthesia and is the stage used in operating theatres
regular breathing
cough and vomit reflex depressed
pupils initially constrict but as you get deeper into the stage, the pupils dilate
large skeletal muscle relax
drop in blood pressure
corneal reflex disappears
stage 4
as you get deeper into further stages of anaesthesia, breathing becomes shallow and there are falls in blood pressure with a feeble pulse and pupils dilate more
In stage 4, there is no ventilations due to depression of the medulla oblongata and other and associated respiratory centres.
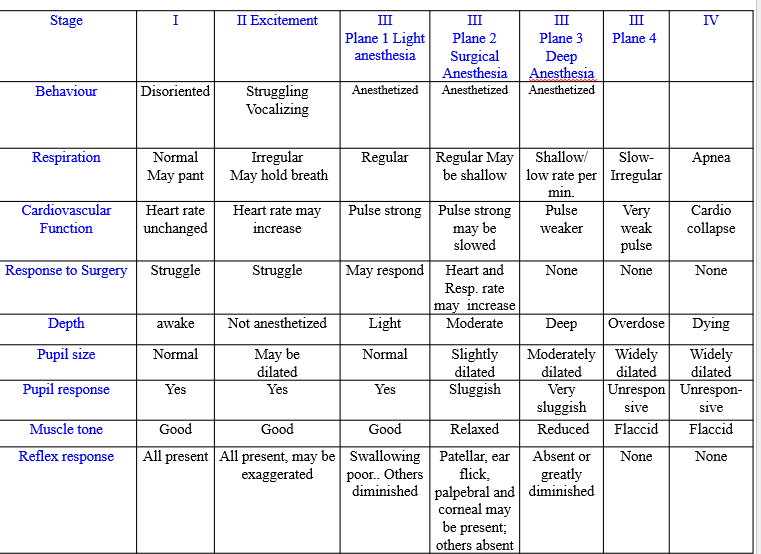
the stages of anesthesia are difficult to measure and most of the signs of Guedel’s classification depend on muscular movements including respiratory muscles but this means that paralysed patients clinical signs are not detectable. As well as this, the use of multiple agents obscure signs. The stages of anaesthesia measured in this way are often thought of as obsolete
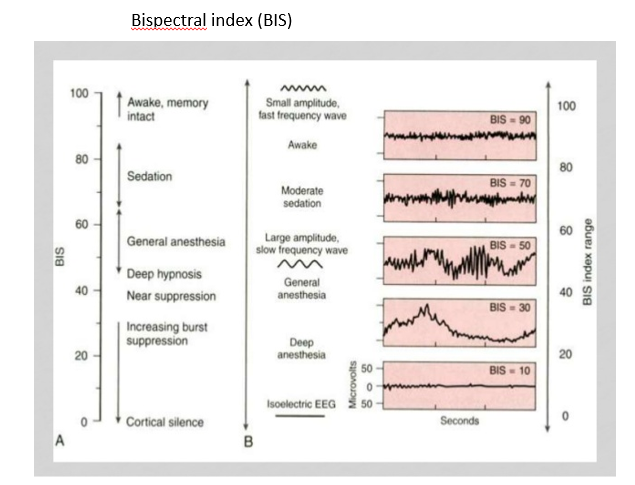
As anaesthesia deepens, the amplitude of high frequency components of EEG falls with an increase at the lower frequencies. This could potentially mean that the EEG can be used to monitor the depth of anaesthesia however:
these changes are agent dependent
various pathophysiological events also effect the EEG such as hypotension or hypoxia
Patient state index is one EEG method of assessing hypnosis and was developed by comparing large numbers of EEGs during induction, maintenance and emergence.
Cerebral function monitor is where the signal is filtered, semi logarithmically compressed and rectified. It represents the overall electrocortical background activity of the brain
Bispectral index is statistically based and an empirically derived complex parameter.
General anesthetic mechanisms of action
there are three major theories:
lipid theory
protein theory
combination of both - lipid/protein interface
lipid theory
The lipid theory states that general anesthetics dissolve in membranes which leads to:
changes in bilayer thickness
changes in order parameters
changes in curvature elasticity
these effects may then effect the proteins present in the membrane. There are three pieces of evidence to support this:
Meyer-Overton Correlation
The Meyer-Overton correlation states that the potency of an anesthetic is proportional to its solubility in lipids.
Evidence: This relationship was first observed by Meyer and Overton independently in the early 20th century. They found that the more lipid-soluble a compound is, the lower the concentration needed to achieve anesthesia. This implies that anesthetics exert their effects by interacting with the lipid components of cell membranes.
Example: Anesthetics like diethyl ether, chloroform, and halothane show a strong correlation between their lipid solubility and their anesthetic potency.
2. Critical Volume Hypothesis
The critical volume hypothesis extends the Meyer-Overton rule, proposing that anesthetics cause anesthesia by expanding the lipid bilayer to a critical volume, thereby disrupting membrane function.
Evidence: Studies have shown that anesthetics can cause a measurable increase in the volume of lipid bilayers. This expansion is thought to interfere with the function of membrane proteins, particularly ion channels, which are crucial for nerve transmission.
Example: Experiments using model lipid bilayers and biological membranes have demonstrated that anesthetic molecules can insert into the lipid bilayer, causing it to expand and alter its physical properties.
3. Pressure Reversal of Anesthesia
High pressure can reverse the effects of anesthesia, suggesting that the action of anesthetics involves changes in membrane structure or function that can be counteracted by pressure.
Evidence: Research has shown that applying high hydrostatic pressure can reverse the effects of various anesthetics. This supports the idea that anesthetics work by causing physical changes in the lipid bilayer, as increased pressure can counteract the volume expansion caused by anesthetics.
Example: In animal studies, high pressure has been used to reverse the anesthesia induced by agents such as nitrous oxide and halothane, further supporting the role of lipid interactions in anesthetic mechanisms.
as well as this, the fact that there is no defined chemical structure also supports the lipid theory
problems with the lipid theory include:
new compounds do not fit the meyer-overton correlation
an increase in carbon length leads to the cut off effect where there is a loss in analgesia
small increases in temperature produce similar changes in membrane density and fluidity but do not produce anesthesia
the protein theory
this states that general anesthetics bind to specific membrane proteins with 3 major proteins implicated:
GABAa receptor (inhibitory)
2 pore K+ channels (control resting potential)
NMDA receptor (excitatory)
evidence for this is the fact that mutations in channels in animal models either reduce or increase anaesthetic potency.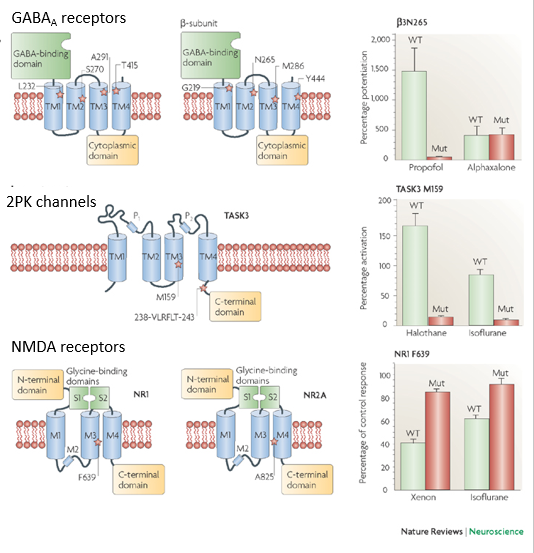
the criteria for identifying relevant anesthetic protein targets is as follows:
reversibly alters target function at clinically relevant concentrations
protein target expressed in appropriate anatomical location in brain or spinal cord
stereo selective effects in vivo parallel actions on the target in vitro
target exhibits appropriate selectivity and insensitivity to model and non anaesthetic compounds.
an ideal anesthetic should have rapid action and recovery with minimal irritant properties. There should also be no risk of explosion and is should be analgesic and a muscle relaxant. No single anaesthetic as all properties so a combination of agents has to be used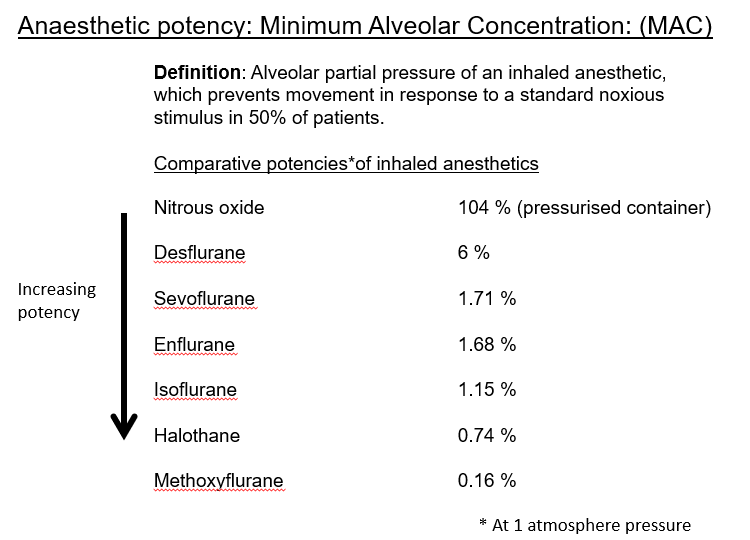
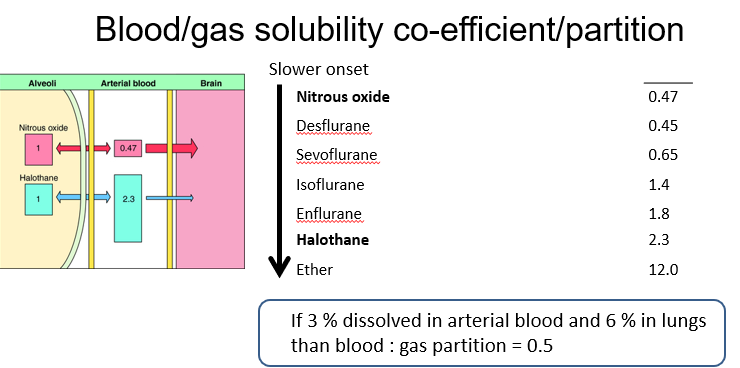
pharmacokinetics
blood acts as a reservoir for inhaled agents and the greater the solubility in blood, the more there is a reduction of rise of alveolar partial pressure. This reduces the rate of brain partial pressure which leads to the slower rate of the onset of anaesthesia.
an increase in cardiac output delays induction and a decrease in cardiac output can lead to an overdose of anesthetics. In lean tissues such as the brain, there is fast perfusion and a small partition coefficient and rapid equilibrium. This means that the onset of analgesia is faster In fat, there is slow perfusion and a large partition coefficient and a slow equilibrium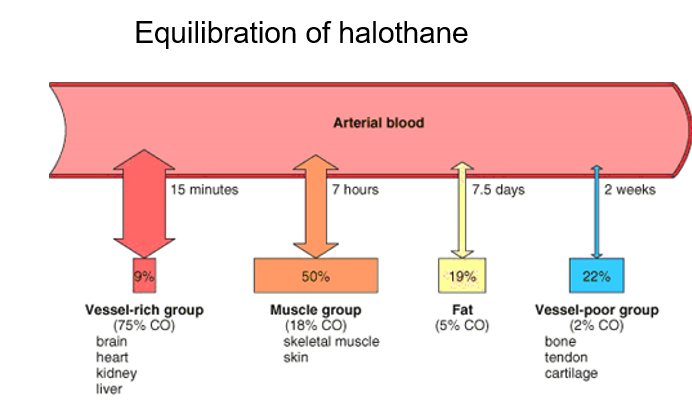
from the pharmacokinetics of induction and recovery, you can see that the anesthetics with the fastest induction such as N2O has the fastest recovery but ether has a slow induction and a slow recovery.
recovery from anaesthesia
Rate of reduction of alveolar partial pressure determines the rate of recovery from the anaesthetic. elimination of inhaled anaesthetics is mainly done by ventilation through the lungs. Factors decreasing the length of recovery include:
reduction of the inspired concentration
high alveolar ventilation
low blood gas solubility
short duration of anesthesia (little anaesthetic dissolved in low perfusion tissue)
anesthetic examples
Inhalation anesthetics are most commonly used as halothane, isoflurane, sevoflurane and desflurane. They are all volatile liquids that produce fast loss of consciousness, smooth induction and recovery although induction with IV agents is preferred. These anesthetics produce dose dependent lowering of the mean arterial pressure by their combined action on myocardial function and on peripheral vascular resistance. They also depress respiration leading to the increase in arterial carbon dioxide level and impairment of oxygen exchange. The metabolic rate of the brain is decreased by inhalation anaesthetics even though they increase cerebral blood flow. There is also relaxation of skeletal muscles which occurs by central action.