Restoration of Dental Implants
Priority groups for implants
1. Patients with congenital, inherited conditions that have led to missing teeth, tooth loss or malformed teeth
2. Patient with traumatic events leading to tooth loss
3. Patients with surgical interventions resulting in tooth and tissue loss, e.g. head and neck cancer
4. Patients with congenital or acquired conditions with extra-oral defects, e.g. eyes or ears
5. Patients who are edentulous in either one or both jaws who repeated conventional denture treatment have been unsuccessful
6. Patients with severe oral mucosal disorders and those with severe xerostomia where conventional prosthetic treatment is not possible
7. Patients who do not have suitable existing teeth that can be used for anchorage to facilitate orthodontic treatment
Implant Treatment
Planning phase → Surgery (period of osteointegration healing - 4-6 months in maxilla and 3-6 months in mandible) → Restoration → Maintenance
Implant Planning
Prosthetically driven implant treatment
First plan final tooth positioning
Use as a guide for 3D positioning of the implant fixture
Diagnostic wax-up can then be used as:
Radiographic stent – to indicate tooth positioning
Surgical stent – to guide implant placement
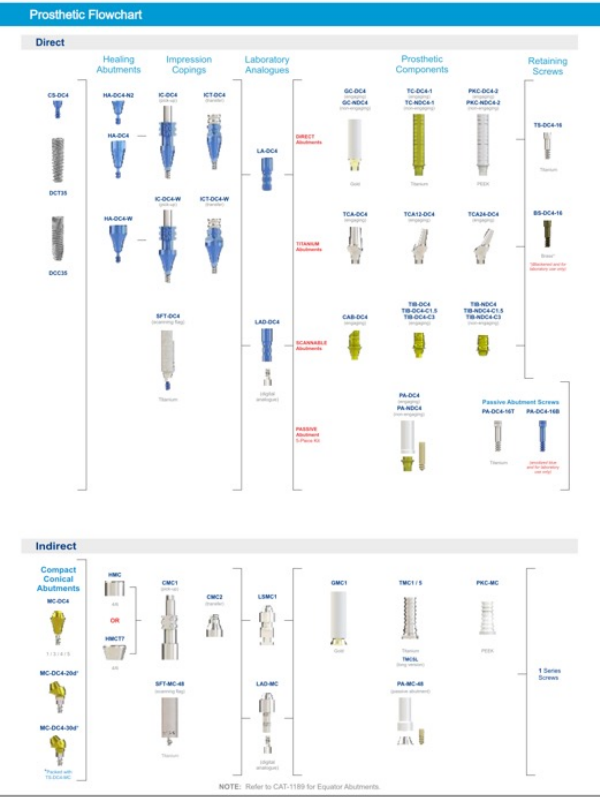
Terminology
Implant fixture
Healing abutment
Abutment
Healing cap
Crown
Bridge
Bar
Insert
Locator
Clix
Housing
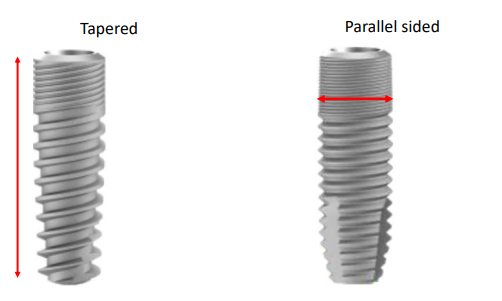
Implant fixture - goes into the bone
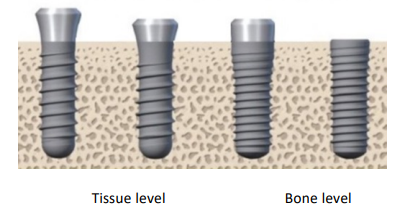
The benefit of tissue-level fixtures is that they are far away from the bone for bacteria colonising which can then lead to bone loss.
The challenge of the tissue-level implant is that it is harder to place surgically.
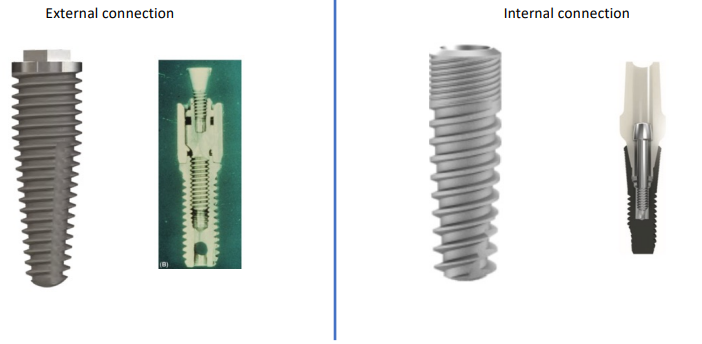
Implant fixture – prosthetic connection
Treatment strategies
• Single tooth replacement - crown
• Multiple tooth replacement – bridge
• Full arch replacement
• Fixed
• Removable
Principles of all implant restorations
• Good aesthetics
• Well retained
• Functional
• Cleansable
• Retrievable
Single tooth replacement
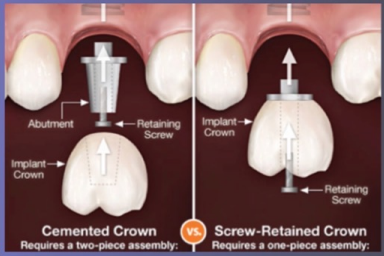
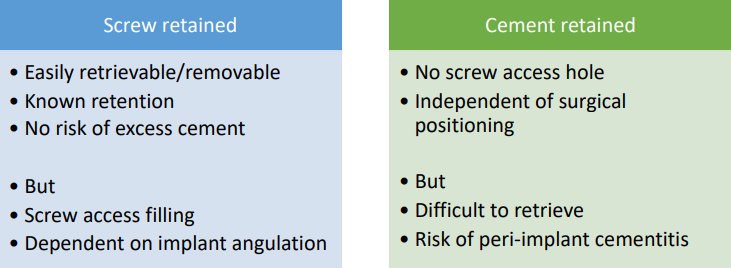
Design features:
Screw retained: one piece
Cover screw retained hole with composite after placing for aesthetics
Cement retained: two pieces
Clinical stages – single crown
Planning → Surgical phase → Healing for osseointegration
→ Primary impressions (using a special tray) → Open tray implant, pick up secondary impression → Fit

Multiple tooth replacement - bridge

Clinical stages - bridge
Planning → Surgical phase → Healing for osseointegration
→ Primary impressions, open tray implant pick up secondary impression → Verification jig, jaw reg → Try in → Fit
Full arch implant restorations
Full arch – treatment planning decisions
1) Does the patient require lip support?
2) How much prosthetic space is available?
Full arch - Fixed
- Gums included or not, materials (metal ceramic, acrylic, etc), etc
- More prosthetic space then go for acrylic!
• Benefits
• Not removable!!
• Improve quality of life
• Improved chewing ability vs removable
• Lower long-term maintenance
• Decision making:
• Material choice – acrylic vs MCC/Zirconia
Full arch - Removable
• Benefits
• Improved quality of life vs C/C
• Easy to clean
• Good aesthetics
• Decision making:
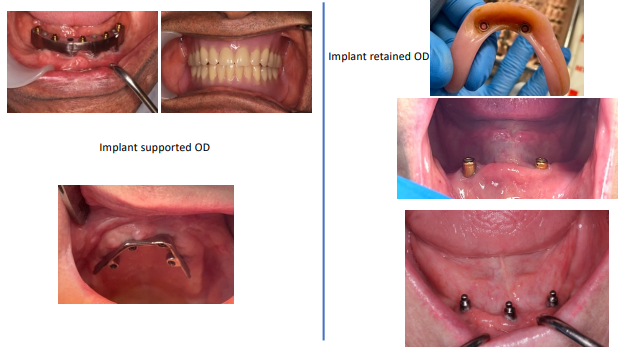
• Implant-supported OD - prevents it from sinking into the soft tissues
• Implant-retained OD - the nylon insert will wear over time
Implant-supported vs Implant-retained
Space requirements - Removable
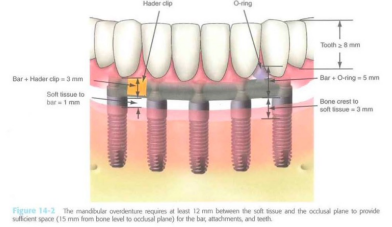
Full arch - Removable
Goodacre
Most common problems – loss of retention, need for relining, wear of attachment, fracture of prosthesis
• Red inserts have most retention
• White inserts have the least retention
Summary
• Restoration of implants can be challenging
• Requires good working knowledge of the implant system used
• Removable full arch may be required due to significant loss of soft tissue but comes with increasing maintenance due to loss of retention
• ALL implant restorations require some maintenance, and ultimately replacement – everything fails!!