purinergic signalling
There are two types of purine based signalling molecules:
nucleotide (contain phosphate group(s) eg ATP
nucleoside (don’t have phosphate group(s)
A huge amount of ATP is produced everyday however it is not the only cellular energy source and is also a neurotransmitter
Purine production, release, metabolism and receptors
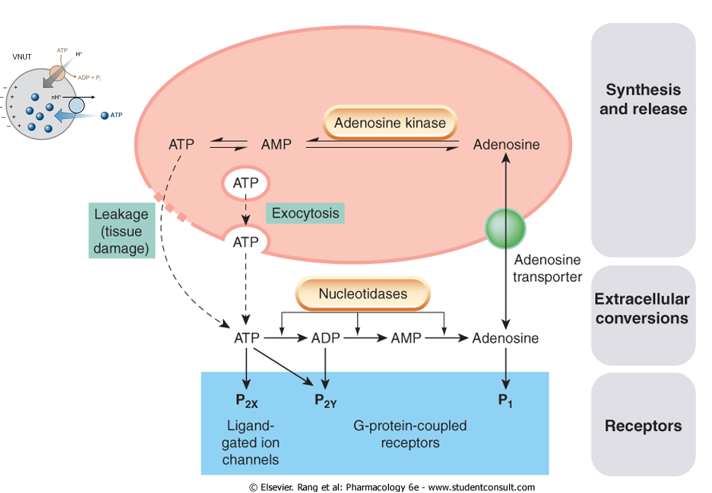
ATP is produced through the regular synthesis
For packaging however, the transporter is Vnut which accumulates ATP into vesicles by the same mechanisms
It is then released by exocytosis often As a co transporter as well as on its own. This happens when there is tissue damage so ATP is leaked into the extracellular space due to high concentrations in the cytosol
Once ATP has been released, they activate P2X receptors which are ligand gated ion channels. P2Y receptors can also be activated and these are G protein coupled.
In the extracellular space, ATP is metabolised by nucleotidases which limit signalling by ATP but gives rise to other molecules (eg ADP, AMP and adenosine). ADP can act as an antagonist to P2Y receptors. Adenosine activates P1 receptors
adenosine is removed by adenosine transporter which is known as an equilibrium transporter as it operates on concentration gradients ( high concentrations of adenosine outside means it will go down the gradient into the Cell). This gradient is maintained by adenosine kinase
Purine receptors are known as P2X receptors of which there are 7 subtypes. They are activated by ATP and are ionotropic - directly open when bound to the right substance. They are trimeric rather than tetrameric like glutante or pentameric like nicotinic receptors however still has a TM2 domain which forms the central facing helix. Structurally, they have a dolphin topology and have alternative ion access - through rather than just the entire channel above through gaps just above the membrane rather than going through the entire pore - like a colander receptor except it is its entrance and not the exit.
Another purine receptor are the P2Y receptors where 1,12 and 13 are activated by ADP, 2 and 11 by ATP and 4,6 and 14 are activated by other pyrimidines. UTP and UDP-glucose can activate hen as well. These receptors are G protein coupled and are important for platelet aggregation. Where antagonists stope aggregation, it can be used as treatment for strokes, emboli and heart attacks.
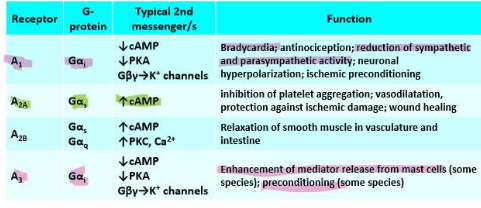
P0 receptor are activated by adenine and are also G protein coupled. P1 receptors such as 1, 2A, 2B and 3 are activated by adenosine and are also G protein coupled
They are very widely spread so targeting is an issue since it is so widespread in the body - a drug that activates or inactivates one could do the same for others leading to side effects.
Evidence for ATP being a transmitter
Early work showed that stimulation of nerves promote the release of ATP. Other studies done on guinea pig vas deferens show that the excitatory action potential decreases with increasing concentrations of a,b,methylene-ATP which is a compound that desensitises P2X receptors. This suggests that the action potentials are mediated through the activation of these receptors. The spontaneous release of ATP containing vesicles was also stopped.
Where the control showed regular EJP or excitatory junction potential for guinea pig vas deferens but there in the presence of a-b methylene ATP, there was little to no signal depending on the stimulation. This means that a,b-methylene ATP desensitises P2X receptors that suggests that the action potential are mediated by P2X activation. In addition, the spontaneous release of ATP from vesicles stopped
Due to the conversion of ATP to adenosine, a feedback loop can be created as adenosine will switch off the release at a synapse and this allows finer control of neurotransMitter release
Other studies have shown that stimulation of these purinergic nerves will lead to inhibition of activity.
ATP can also mediate inhibition and prevent contraction of smooth muscle. ATP was shown to affect synaptic transmission as well - Where transmission wasn’t blocked with substances such as hexamethonium. Transmission was affected/inhibited with drugs pertaining to ATP such as suramin and alpha beta-methylene-ATP, Therefore these are being mediated by P2X/ATP
P2X
These receptors are involved in pain pathways where ATP is a primary signal for pain - P1 can also be a main signaller in this pathway.
P2X antagonists produce analgesia:
P2X3R
involved in chronic coughing where irritation of the airways or damage causes the signal
Antagonist to P2X3 causes a decrease in coughing
Gefapixant - approved medication
P2X7
Involved in pain and cell death signals
Only activated by very high ATP concentration so is only activated when there is serious damage to cells or tissues
Can lead to excessive efflux of Na/Ca which can act as a signal for apoptosis
antagonists can be used to treat Crohn’s disease:
For Crohn's disease, where there was less abdominal pain and general improvement
The Receptor does NOT DESENSITISE - it cannot be switched off even with excessive stimulation
P1 or adenosine receptors
Adenosine, when injected, causes a drop in BP and HR and is a regulatory metabolite with a protective function to restore heart rhythm during supraventricular tachycardia. It also results in the dilation of blood vessels to increase energy access
In epilepsy and other seizure disorders, adenosine levels are elevated after seizure activity to suppress further activity. In an experiment, high levels of adenosine were administered to replicate a seizure and it was found that ATP was converted to adenosine which then suppressed the seizure.
Using an antagonist meant that there were spontaneous seizures and there was a lack of hyperpolarization when needed so cells and tissue were more sensitive to stimulation - more seizures.
adenosine kinase regulates the amount of adenosine present in the extracellular space. When this doesn’t function, there is depression of synaptic transmission due to A1 stimulatory - inhibitory so leads to less. In severe epilepsy there is high proliferation of astrocytes. Astrocytes contain adenosine kinase so high numbers of astrocytes means that this is in high concentration which means that more adenosine flows into astrocytes due to the concentration gradient so less leave. This gives protection. This also leads to more sensitive tissue as there is a lower threshold for seizure initiation. ADK deficiency means reduced seizure activity due to the high amount of adenosine