Functional brain development and paediatric acquired brain injury
Functional MRI in the Developing Brain
Structural MRI shows what the brain looks like.
Functional MRI techniques show how the brain works and how different regions are connected. This is particularly important in children, where brain function is still developing and can reorganise after injury.
Functional imaging focuses on networks, not single brain areas.
Why Functional MRI Is Treated Differently from Structural MRI in Paediatrics
The short answer is:
Structural MRI tells you what developed.
Functional MRI tells you how the brain is using what developed.
In children, those two things often do not match.
Structural MRI: Development Follows Rules
Structural MRI works well in paediatrics because:
Brain development follows predictable biological sequences
Myelination, sulcation, and growth occur in an orderly way
Deviations from the normal pattern usually mean:
injury
malformation
genetic disorder
So when you look at structural MRI in a child, you are asking:
Did this part of the brain form normally for this age?
That’s why structural imaging is:
Pattern-based
Age-dependent
Good at timing injury
Functional MRI: Development Is Adaptive, Not Fixed
Functional MRI behaves very differently because brain function is not fixed early in life.
In children:
Functions are distributed
Networks are still forming
The brain can reassign tasks to different regions
So functional MRI is asking a different question:
How is this brain actually working right now?
That answer depends on:
age
experience
injury timing
plasticity
Two children with the same structural lesion may show completely different functional maps.
Why This Difference Is Bigger in Children Than Adults
Adult brains:
Have stable anatomy
Have stable functional localisation
Structure and function usually align
Paediatric brains:
Are still wiring themselves
Can move function across hemispheres
Can preserve function despite structural damage
So in children:
Structure ≠ function
Function may look “normal” even when structure is abnormal
Or function may be reorganised in unexpected places
Why Functional MRI Needs Different Interpretation Rules
Functional MRI in children:
Is less about localisation
More about network engagement
More variable
More context-dependent
You are not asking: “Where is language?”
You are asking: “How has language been organised in this child?”
That’s a fundamentally different mindset.
Key Imaging Techniques
Diffusion Tensor Imaging (DTI) and Tractography
DTI is a functional MRI technique that visualises white-matter pathways by measuring the direction of water diffusion along axons. Because water moves more easily along fibres than across them, major tracts can be reconstructed using tractography.
DTI allows us to study:
Brain connectivity
White-matter maturation
Disruption of pathways following injury
This is especially valuable in children, where damage may affect connections even when cortical anatomy appears relatively normal.
Important White-Matter Tracts
Language Pathways
The arcuate fasciculus connects frontal and temporal language regions. DTI can show whether this pathway is present, reduced, or disrupted. Abnormalities in this tract are associated with language impairment and developmental language disorders.
DTI helps explain why some children have language difficulties despite minimal visible cortical damage.
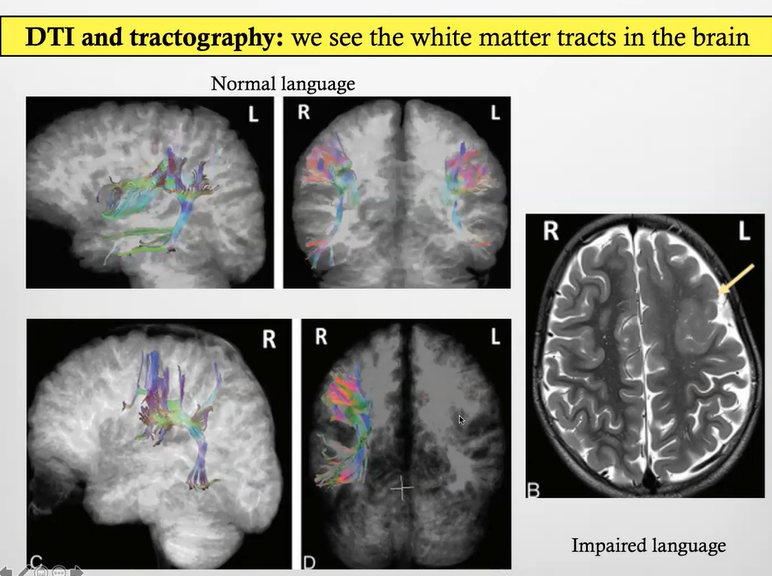
Patient 1 (Top Row): Normal Language
The top images show DTI tractography from a child with normal language development. The white-matter tracts are well formed and continuous, with a clear language pathway connecting frontal and temporal regions and normal hemispheric lateralisation. This indicates an intact language network with effective connectivity between cortical areas. Even without structural MRI, the tractography alone explains why language function is preserved.
Patient 2 (Bottom Row): Impaired Language
The bottom images show DTI tractography from a different child with language impairment. The language pathways are reduced, fragmented, and abnormally organised, with loss of continuity between key language regions. This disrupted connectivity indicates a network-level abnormality and already suggests a functional explanation for the language deficit.
DTI tractography only shows coloured fibre lines when water diffusion is directionally constrained along intact axons; if tract structure is damaged or disorganised, directional diffusion is lost and the tracts cannot be reconstructed. This is why, in the bottom image, no tract model is generated on the left side, the underlying white-matter pathway is too disrupted for the algorithm to identify a coherent direction of diffusion.
Structural MRI (Right): Same Patient as Bottom Row
The T2-weighted structural MRI on the right belongs to the same child shown in the bottom row. It demonstrates a large focal cortical dysplasia involving the language area. This malformation disrupted normal brain development and prevented the left arcuate fasciculus from developing properly. While structural MRI shows the location and extent of the cortical abnormality, it does not explain language outcome on its own. The DTI findings complete the picture by showing failure of normal language network formation due to impaired white-matter tract development.
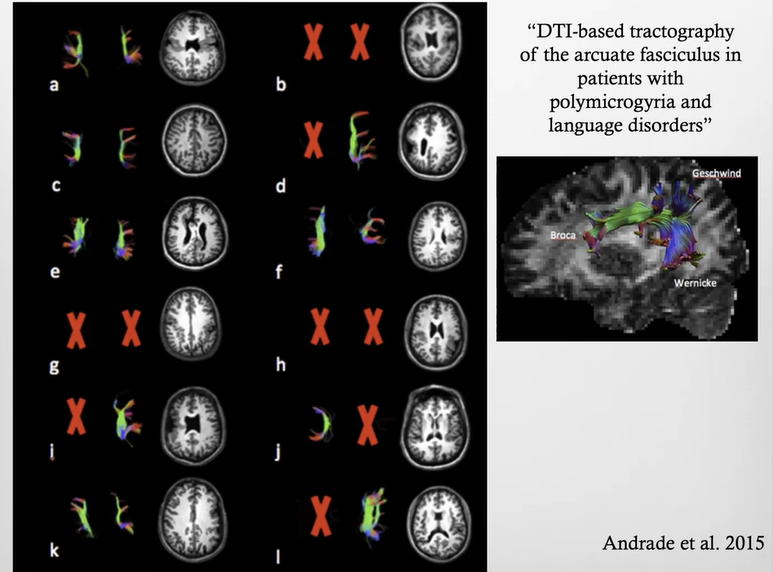
DTI Tractography of the Arcuate Fasciculus in Polymicrogyria
This figure comes from a study examining DTI-based tractography of the arcuate fasciculus in patients with polymicrogyria affecting language areas. Polymicrogyria is a malformation of cortical development characterised by abnormally thick, small, and irregular gyri, particularly affecting cortical organisation.
The purpose of the figure is to show how structural cortical malformations affect the development of language white-matter pathways.
What the Coloured Tracts Represent
The coloured fibre bundles represent DTI tractography reconstructions of the arcuate fasciculus, the major white-matter pathway connecting frontal (Broca) and temporal (Wernicke) language regions.
In healthy brains:
The arcuate fasciculus is continuous
It has a predictable shape and course
It supports normal language function
What the Red Crosses Mean (Key Point)
The red crosses indicate cases where the arcuate fasciculus could not be reconstructed using DTI.
This does not mean the software failed.
It means:
There was no coherent, directional water diffusion
The white-matter fibres were absent, severely disrupted, or never developed
The tract does not exist in a form that can be modelled
In some patients:
The arcuate fasciculus is completely absent
In others:It is present but markedly dysmorphic, reduced, or fragmented
Why This Happens in Polymicrogyria
In polymicrogyria:
The cortex is abnormally organised
Gyri are small and thick
Normal cortical layering is disrupted
Because white-matter tracts develop in coordination with cortex:
Abnormal cortex cannot support normal tract development
The arcuate fasciculus may fail to form or form abnormally
This is why, in several patients, no arcuate fasciculus is seen at all.
Clinical Meaning of the Figure
This figure demonstrates that:
Language impairment can reflect abnormal white-matter anatomy
Structural cortical malformations can prevent normal language network formation
DTI reveals network-level abnormalities invisible on standard MRI
The key lesson is:
Language problems in developmental disorders are often due to abnormal connectivity, not just abnormal cortex.
Motor Pathways
The corticospinal tract carries mo
tor signals from the cortex to the spinal cord. DTI demonstrates how this pathway develops over time and how it is affected in conditions such as cerebral palsy.
Reduced integrity of the corticospinal tract correlates with poorer motor outcome.
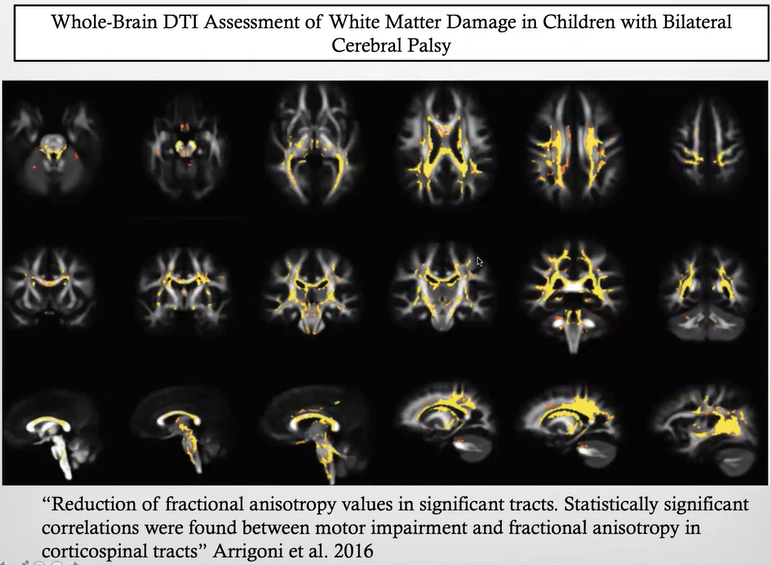
Whole-Brain DTI Assessment in Bilateral Cerebral Palsy
This figure shows a group-level DTI analysis comparing children with bilateral cerebral palsy to typically developing controls. Rather than displaying individual fibre tracts, it presents a statistical map of white-matter damage across the whole brain.
The technique uses diffusion tensor imaging (DTI), but instead of 3D tractography, it analyses diffusion properties voxel by voxel.
What the Yellow/White Areas Represent
The highlighted yellow/white regions indicate areas where fractional anisotropy (FA) is significantly reduced in children with cerebral palsy compared with controls.
Reduced FA means:
Loss of fibre organisation
Abnormal myelination
Disrupted axonal integrity
These areas therefore represent damaged or abnormally developed white matter.
How This Is Different from Tractography
This is not a 3D reconstruction of tracts.
Instead:
It is a map showing where white matter is abnormal across a population
It uses the same DTI sequence
But applies statistical comparisons between groups
So you are seeing patterns of vulnerability, not individual pathways.
What It Shows About Cerebral Palsy
The map demonstrates that in bilateral cerebral palsy:
White-matter damage is widespread
Multiple motor and associative pathways are affected
Damage is not limited to a single tract
Importantly, the study showed a significant correlation between motor impairment severity and reduced FA in the corticospinal tracts, linking structural connectivity directly to clinical function.
Why This Matters Clinically
This figure reinforces that cerebral palsy is:
A disorder of brain connectivity
Not just focal lesions or cortical damage
DTI provides objective evidence of:
Network-level injury
Structure–function relationships
Severity-related changes
Developmental Changes in White Matter
White-matter tracts mature gradually:
Organisation increases
Fibres become more coherent
Signal measures reflect increasing myelination
Early injury can alter this trajectory, leading to long-term functional consequences even if the initial lesion appears small.
DTI therefore provides a quantitative marker of brain development and injury
Functional MRI (fMRI): Measuring Brain Activity
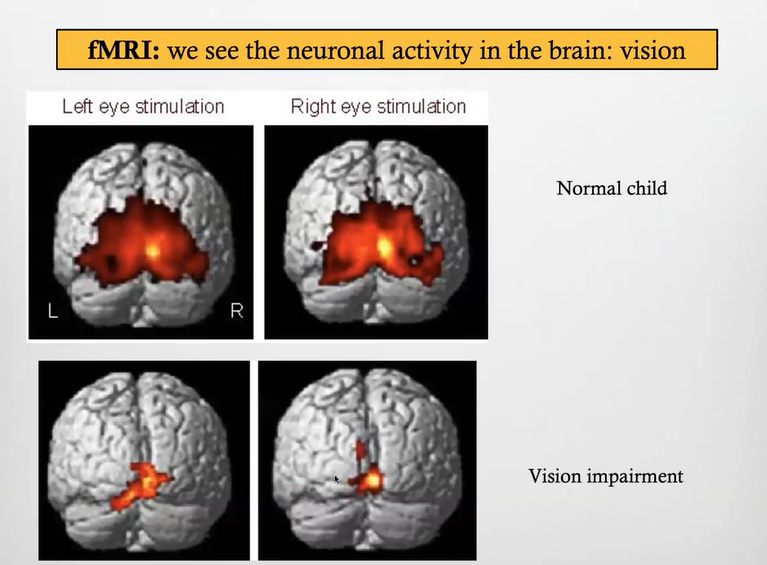
fMRI measures brain activity indirectly using the BOLD signal, which reflects changes in blood oxygenation linked to neuronal activation. Active brain regions consume more oxygen, leading to detectable signal changes.
A bright or coloured region on fMRI indicates an area where activity increased during a task compared with rest. It does not mean neurons are literally glowing or that a region is simply “on”; the signal always reflects a relative change over time. fMRI works by comparing rest and task states, so only regions that alter their blood oxygenation between these conditions appear activated. This is why fMRI highlights motor cortex during movement, language areas during speech tasks, and visual cortex during visual stimulation. In essence, fMRI images appear to “light up” because active brain regions receive extra oxygen-rich blood, producing a stronger magnetic signal shown as bright or coloured activation.
Task-Based fMRI
Motor fMRI
Motor tasks activate specific regions of the motor cortex. fMRI is useful for mapping motor organisation, particularly when anatomy is abnormal or displaced.
Language fMRI
Language tasks identify language networks and hemispheric dominance. This is especially helpful in children with epilepsy, developmental brain abnormalities, or early brain injury.
Altered or bilateral activation patterns reflect developmental reorganisation.
Visual fMRI
Visual stimulation activates the occipital cortex. Reduced or absent activation may be seen in visual impairment, demonstrating how sensory deficits affect cortical organisation.
Neuroplasticity and Functional Reorganisation
One of the key messages of functional MRI in children is neuroplasticity.
After early injury:
Function may shift to the opposite hemisphere
Nearby regions may take over lost functions
Networks reorganise rather than repair damaged tissue
Functional MRI provides direct evidence of this adaptive reorganisation.
Paretic - weakness or partial paralysis of muscles, meaning incomplete loss of movement
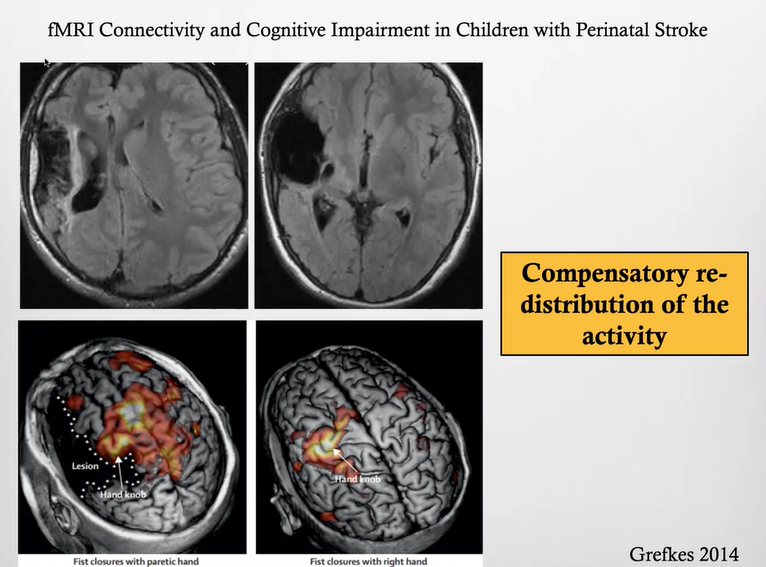
fMRI Connectivity and Plasticity After Perinatal Stroke
This figure shows a child with a perinatal middle cerebral artery (MCA) infarction, resulting in focal structural damage to the motor cortex. On structural MRI, the infarcted area is clearly visible and includes the region that would normally control hand movement.
Despite this early injury, fMRI during a motor task (fist closure) shows preserved motor function, but with activity occurring in atypical cortical locations. Instead of activating the usual hand area, motor activation is shifted to adjacent and more lateral regions of the cortex.
This pattern reflects neuronal plasticity in the developing brain. Because the injury occurred early, the brain was able to reorganise motor networks and redistribute function away from the damaged region.
Compensatory Redistribution of Activity (Key Concept)
The slide demonstrates compensatory redistribution of activity, meaning that:
The original motor area is damaged
Motor function is taken over by neighbouring or alternative cortical regions
Function is preserved, but the anatomical location of activation changes
This is not recovery of the damaged tissue, but reassignment of function within the network.
Clinical Significance
This example shows why functional MRI is essential in paediatric brain injury:
Structural MRI alone would predict severe motor deficit
fMRI reveals preserved function through reorganisation
Outcome depends on timing of injury and plasticity, not lesion size alone
What the stroke did in this child
This child had a perinatal MCA stroke, which damaged:
The normal hand area in one hemisphere (the one that should control the affected hand)
So the usual control centre for that hand was destroyed early in life.
What the developing brain did instead
In this child, the normal hand area (the hand knob) in the damaged hemisphere was destroyed by the MCA infarct. Because the injury happened very early, the brain reorganised motor control by recruiting alternative motor regions.
1. Adjacent motor cortex in the injured hemisphere
2. Secondary motor areas (premotor cortex)
3. Contralateral (opposite hemisphere) motor regions
This does not mean a full swap of control, but rather:
Bilateral or contralateral assistance
Shared control across hemispheres
This is called compensatory redistribution of activity.
Clinical Implications
The use of DTI is significant in understanding language disorders, as shown in patients with conditions such as polymicrogyria, where structural abnormalities correlate with language impairments.
Evaluation of motor function can reveal neuroplasticity adaptations in response to ischemic events (e.g., middle cerebral artery infarction) illustrating shifts in functional activity localization within the brain.
Understanding that the child’s brain undergoes rapid development necessitates timely interventions and imaging to monitor these changes accurately.
Final Summary
Functional MRI complements structural MRI by revealing how the developing brain is organised into networks and how these networks adapt following injury. DTI demonstrates white-matter connectivity and maturation, while fMRI maps functional activation and reorganisation. Together, these techniques show that developmental outcome depends not only on structural damage, but on connectivity and neuroplasticity, making functional MRI essential for understanding cognition, language, and motor function in children.