dermatology and heptobilliary *
HSV 1 primary infection is known as Herpetic Gingivostomatitis.
Commonly, which age groups is this virus seen between
Ages 1 to 5

New cards
9
What is Herpetic Whitlow
Recurrent HSV 1 on the finger.
Caused by Treatment of Infected Patients with Poor Oral Hygiene and/or not wearing gloves.
New cards
11
What is Herpes Zoster
Shingles which develop in patients who have previously had Chickenpox due to the Varicella Zoster Virus.

New cards
14
Why may Zoster cause Mouth Blistering
If the Trigeminal Nerve is affected
New cards
15
Where are Common Sites for Herpes Zoster to occur
- Chest
- Neck
- Lumbar/Sacral Regions
New cards
17
What dose of Acyclovir is prescribed to treat Herpes Zoster
800mg 5 times Daily for 7 days.
New cards
18
What is Herpes Zoster Ophthalmicus
Shingles in the Ophthalmic Division of the Trigeminal Nerve.
Unilateral Distribution

New cards
20
What is Hutchinson's Sign
When a zoster infection has a trigeminal eruption including the tip of the nose indicating Nasociliary Nerve Involvement
New cards
22
What is Molluscum Contagiosum
Common Skin Infection caused by the Pox Virus
Causing a Reactionary Epithelial Hyperplasia

New cards
23
How is Molluscum Contagiosum transmitted
Direct Contact and Vectors for Transmission i.e. Towels, Flannels, Toys and Clothes
New cards
24
What is the Incubation Period for Molluscum Contagiosum
7 weeks from Initial Infection
New cards
26
Describe the Clinical Appearance of Molluscum Contagiosum
Flesh Coloured to Pink, umbilicated and pearly surface
Approximately 1 to 5 mm in diameter
May become itchy or sore and often occurs in clusters
New cards
29
What are the common organisms that cause Cellulitis (2)
1) Streptococcus Pyogenes
2) Staphylococcus Aureus
New cards
31
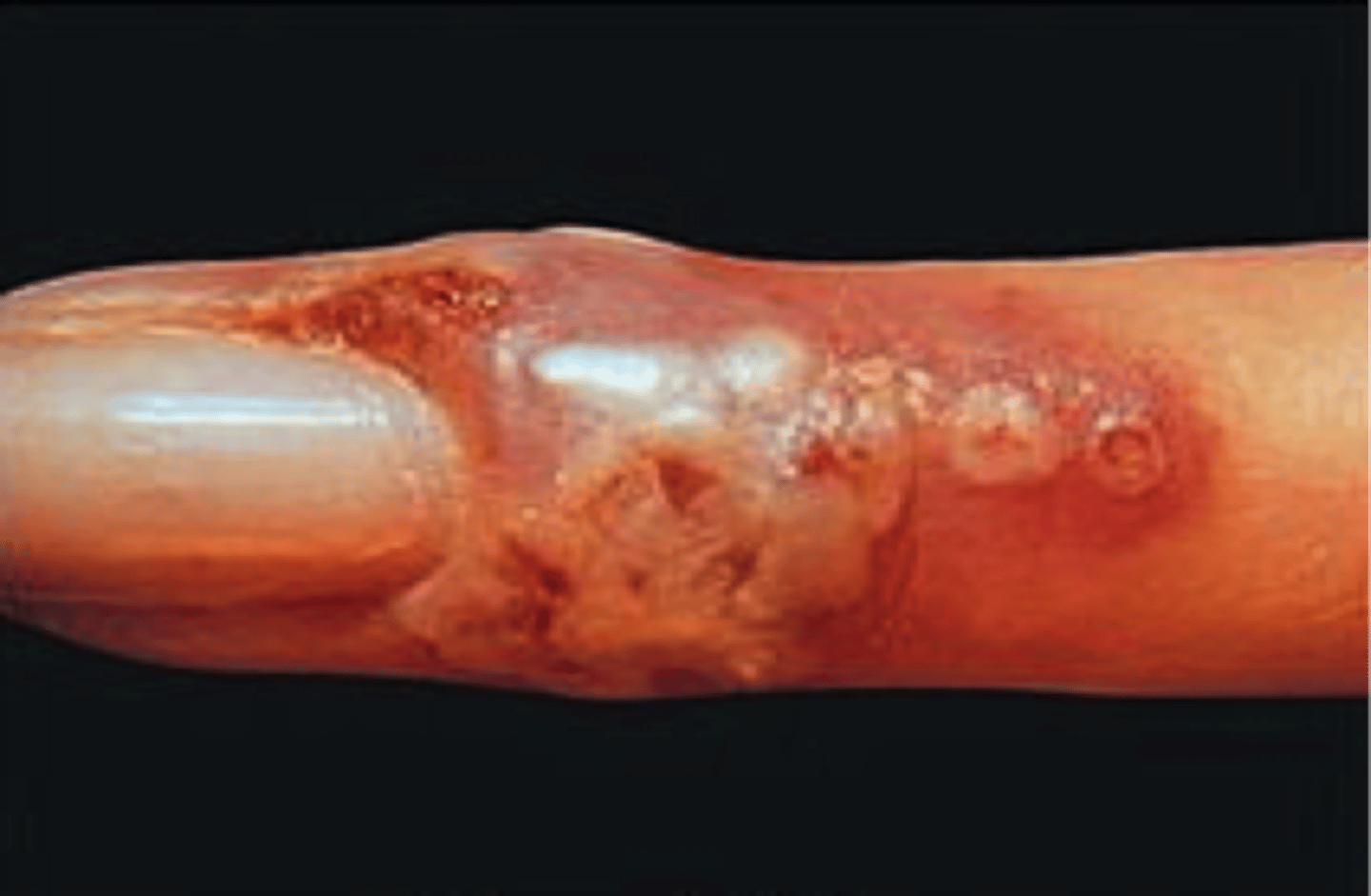
What is the Clinical Presentation of Cellulitis
1) Unilateral
2) Skin becomes Red and Inflamed, Warm to Touch and Painful upon Palpation
3) Erosions, Abscesses and Ulceration may form on the skin
4) Patients may become systemically unwell i.e. high fever and lymphadenopathy
New cards
34
What is Erysipelas
Superficial type of cellulitis caused by Bacterial Infection involving lymphatics.
Margin of lesion is raised and sharpley demarcated

New cards
35
What organisms cause Erysipelas
Almost all cases are caused by Group A Beta-Haemolytic Streptococci (S.Pyogenes)
New cards
36
What is the clinical presentation of Erysipelas
Skin Appears Dimpled Like an Orange Skin
Characteristic butterfly distribution of the cheeks and bridge of the nose
New cards
39
What is Acne Vulgaris
An inflammatory disease of pilosebaceous follicle

New cards
40
Acne Vulgaris results in Blockages in Skin Hair Follicles due to...(4)
- Increased Sebum Production
- Keratin Plugging
- Colonisation by C.Acnes Bacteria
- Local Inflammation
New cards
42
What is the clinical presentation of Acne Vulgaris
Non Inflammatory Lesions (mild acne) presents with open and closed comedones (blackheads and whiteheads)
Inflammatory Lesions (moderate and severe acne) presents with papules, pustules, nodules and cysts
Common Sites affected are the face, neck, chest and back
New cards
43
What is the management of Mild Acne (3)
1) Topical Antimicrobial Agents i.e. Benzoyl Peroxide and Topical Antibiotics
2) Low Dose Combined Oral Contraceptives for Women
3) Topical Retinoid Agents
New cards
47
What is Atopic Dermatitis (Eczema)
Chronic, Itchy skin condition that is very common in children but may occur at any age
Associated with Atopic Tendency (Atopic Dermatitis, Asthma and Hayfever)
Atropy is characterised by an overactive immune response to environmental factors
New cards
48
What is the aetiology of Atopic Dermatitis (Eczema)
(6)
1) Inherited Abnormalities in the Skin Barrier i.e. Filaggrin Expression
2) Immune Factors (abnormal balances in T Cell production)
3) Imbalances in the Microbial Microflora of the skin
4) External Factors that make the skin dry causing loss of barrier function
5) Skin Irritants and Harsh Clothing
6) Stress
New cards
49
What is Filaggrin
Filaggrin are filament associated proteins which bind to keratin fibres in epidermal cells. Abnormal filaggrin is associated with early onset, severe and persistent atopic dermatitis.
New cards
50
What are the signs and symptoms of Atopic Dermatitis (3)
1) Itchy, Erythematous and Dry Scaly Patches
2) Acute Lesions become Erythematous, Vesicular and Weepy
3) Chronic Lesions become Excoriated and Lichenified
New cards
53
What is Psoriasis
Chronic Inflammatory Skin Condition characterised by clearly defined, red and scaly plaques.
Plaques are caused by hyper-proliferation of keratinocytes and secondary inflammatory cell infiltration

New cards
55
What are the causes of Psoriasis (3)
1) Genetics (HLA Subtype)
2) Immunological Factors
3) Environmental Factors i.e. Trauma, Stress, Hot Weather, Alcohol, Smoking, Obesity, Drugs
New cards
57
How is Psoriasis managed?
Psoriasis Area and Severity index (PASI) score used in assessment
1) Avoid Precipitating factors (alcohol consumption)
2) Emollients to soften scale
3) Topical Agents i.e. Vitamin D Analogues, Topical Steroid Creams, Coal Tar, Dithranol, Salicylic Acid, Topic Retinoids
4) Phototherapy (UVB or psoralen combined with UVA)
5) Systemic (Methotrexate, Retinoids, Cyclosporin, Mycophenolate Mofetil, Biological Agents)
New cards
60
What are the 4 Subtypes of Melanotic Naevi
1) Junctional Naevus
2) Dermal Naevus
3) Compound Naevus
4) Combined Naevus
New cards
67
What is Seborrhoeic Keratosis
a benign overgrowth of the basal cell layer of the epidermis. Exact cause is unknown.

New cards
68
What are the aetiological associations of Seborrhoeic Keratosis
1) Skin Friction
2) Genetic Factors
3) Sun exposure
4) Possible Local Inflammatory Response to Malassezia Fungi Species.
New cards
71
What is Spider Telangiectasia
A Benign Skin Condition also known as Spider Naevus or Spider Angioma.
Appears as a Central Red Papule (Spider Body) from which fine red lines extend radially.

New cards
76
What is Pyogenic Granuloma
A very common benign lesion, although exact cause is unknown is it strongly associated with hormonal influences and often indicated by trauma to the skin.

New cards
78
What is the term named if Pyogenic Granuloma occurs on the Gingiva
Epulus

New cards
79
What are the signs and symptoms of Pyogenic Granuloma
- Rapidly Growing
- Red, Browning Blue-Black exophytic growth on the skin. If left untreated they often reach 1-2cm in size
- Usually solitary lesions
- Typically bleed easily and have an ulcerated surface
New cards
81
What is Chondrodermatitis Nodularis Helicis
Benign Inflammatory condition affecting the skin and cartilage of the ear.
Related to repeated pressure and compromised blood supply to the ear.
Contributing Factors include:
- Sleeping predominantly on one side
- Exposure to cold and sun
- Trauma from headphones, mobile devices or hearing aids.
New cards
82
What is the Clinical presentation of Chondrodermatitis Nodularis Helicis (CNH)
- Appears on the Helix or Antihelix of the Ear
- Solitary, Firm, Oval Shaped Nodules around 4-6mm
- May have central crusting and surrounding erythema
- Located on Sleeping Side
- Painful and may prevent sleeping

New cards
87
What are the signs and symptoms of Epidermoid Cysts
Normal or Slightly Pink overlying skin colour, fixed to the skin surface but mobile over deeper layer
Has a central punctum
Bad Smelling Cheesy Debris can be expressed from the central punctum.

New cards
89
What is Solar Lentigo
Liver Spots
Caused by UV light exposure over a prolonged time and Sun Damage to Skin

New cards
91
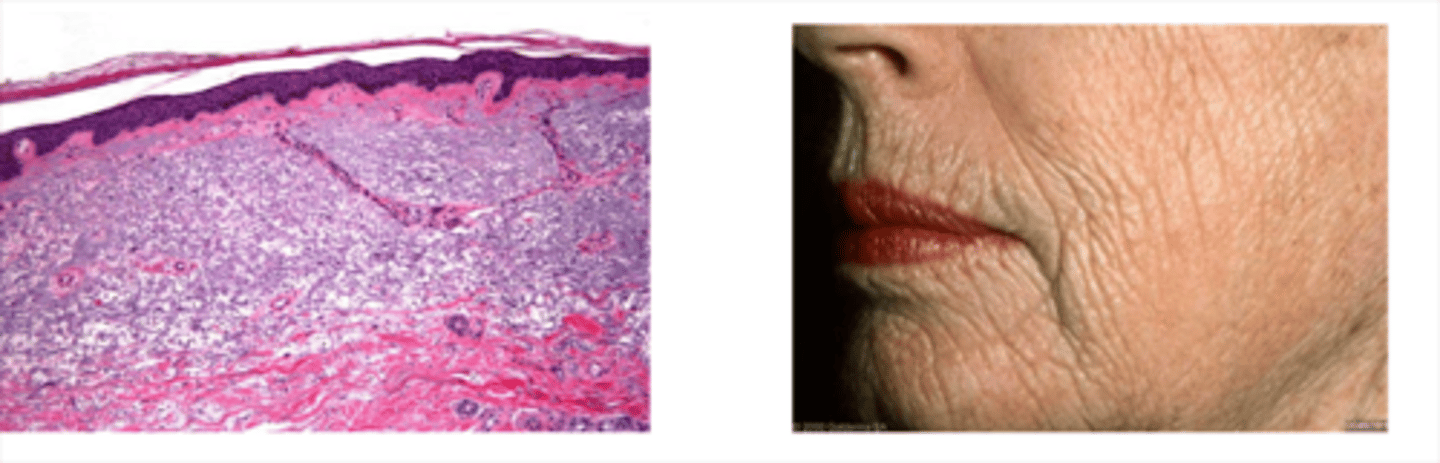
What is Actinic Elastosis
Accumulation of Abnormal Elastin in the Dermis of the Skin caused by Prolonged Sun Exposure.
UV stimulates the fibroblasts to produce excess collagen and elastin
New cards
92
What are the signs and symptoms of Actinic Elastosis
Skin Appears Thickened, Dry, Wrinkled and Furrowed.
New cards
94
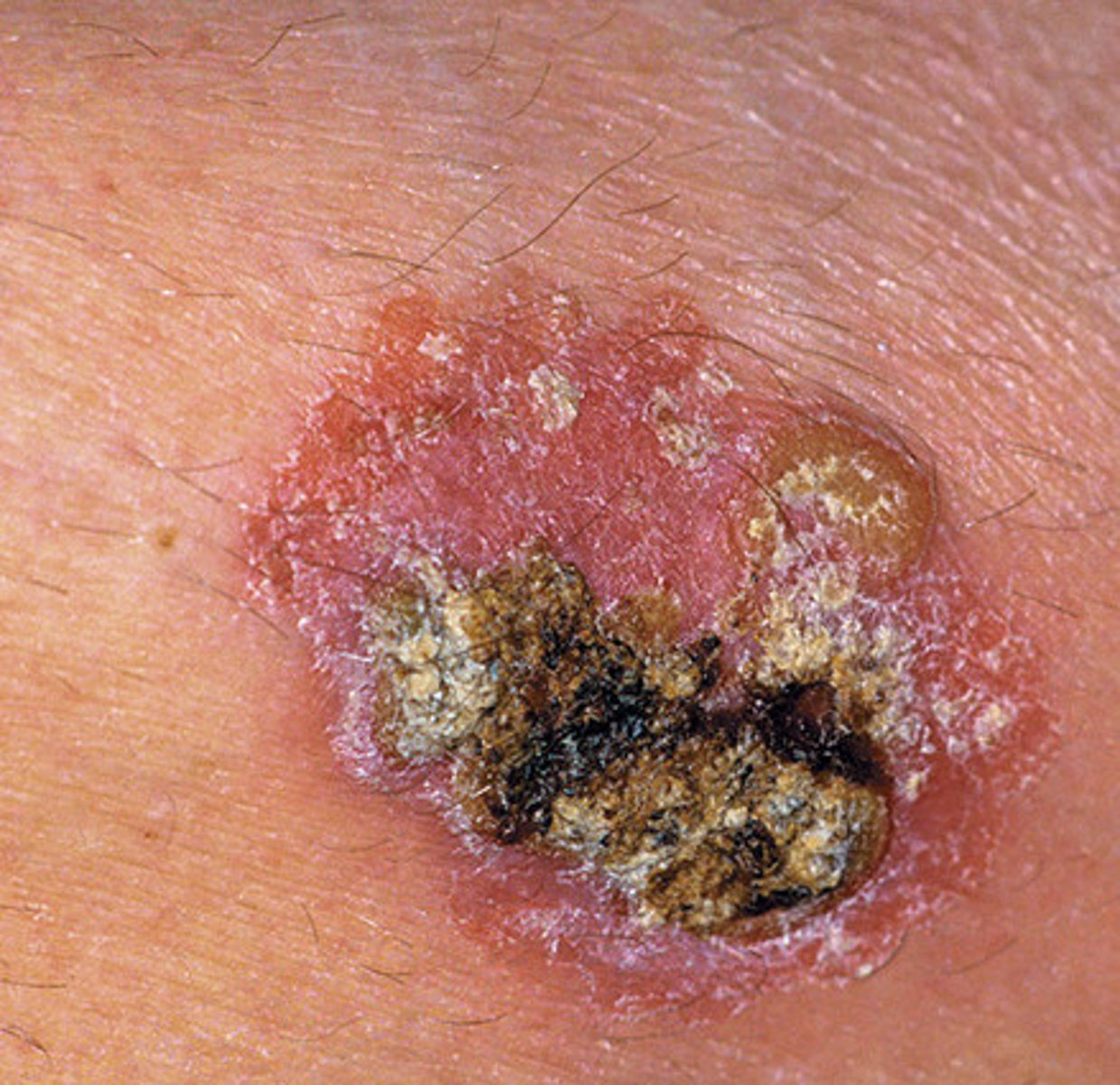
What is Actinic Keratosis
a pre-malignant lesion
flat, scaly area with red edges
20% transform in Squamous Cell Carcinomas
caused by Abnormal Keratinocyte development due to DNA damage by short wavelength of UVB

New cards
95
What are the risk factors of Actinic Keratosis (4)
1) Cumulative UV Exposure
2) Fitzpatrick Skin Types I and II
3) History of Long Hours spent outdoors for work or recreation or use of tanning beds
4) Immunosuppression
New cards
98
What is Basal Cell Carcinoma
Most common form of skin cancer.
Locally invasive malignant tumours that tend to be slow growing.
New cards
100
What are the risk factors for Basal Cell Carcinoma (7)
1) Cumulative UV exposure
2) Previous Skin Cancers
3) Pre existing Actinic Keratosis or Actinic Elastosis
4) Repeated Episodes of Sun Burn
5) Fitzpatrick Skin Types I and II
6) inherited Syndromes
7) Exposure to Ionising Radiation
New cards
101
What are the three clinical subtypes of Basal Cell Carcinomas
1) Nodular
- Most Common
2) Superificial
3) Morphoeic
New cards
102
What is a Nodular Basal Cell Carcinoma
Most Common
Shiny Skin Coloured nodule with smooth surface
Blood Vessels cross its surface
Pearly Rolled Edges
Ulcerated or Necrotic Centre if large

New cards
103
What is a Superficial Basal Cell Carcinoma
Most Common in Younger Adults
Predilection for Upper Trunk and Shoulders
Slightly Scaly and Irregular Plaque
Thin Translucent Rolled Border
Multiple Micro-erosions

New cards
104
What is a Morphoeic Basal Cell Carcinoma
Found Mid-Facial Sites i.e. Cheeks
Waxy scar-like plaque with indistinct borders
Wide and Deep Subclinical extension
May infiltrate cutaneous nerves

New cards
105
What is the Management for Superficial Basal Cell Carcinomas (3)
1) Cryotherapy
2) Curettage
3) Topical Chemotherapy creams (5-Flurouracil cream)
New cards
106
What is the Management for High Risk Basal Cell Carcinomas
1) Mohs micrographic surgery may be performed
2) Lesioned Tissue Excision
3) Radiotherapy if surgery is not suitable
New cards
107
What is a Squamous Cell Carcinoma
Local invasive, malignant tumour of the epithelial keratinocytes
caused by UV radiation causing mutations in p53 tumour suppressor gene
New cards
108
Signs and Symptoms of Squamous Cell Carcinomas
- Ill defined nodules
- Lesions continue to grow in size if left untreated
- May have an ulcerated or necrotic centre
- Surface Crust
- Predilection for Sun exposed sites
New cards
110
What is a Malignant Melanoma
Invasive Malignant Tumour of the Epidermal Melanocytes
New cards
111
What are the risk factors for Malignant Melanomas (4)
1) UV Exposure
2) Fitzpatrick Skin Types I and II
3) Multiple Moles or atypical moles
4) Previous History or Family History of Melanomas
New cards
112
What is Lichen Planus
Autoimmune driven, inflammatory mucocutaneous condition of unknown aetiology.
There is oral mucosal involvement in 30-70% of Lichen Planus Cases
New cards
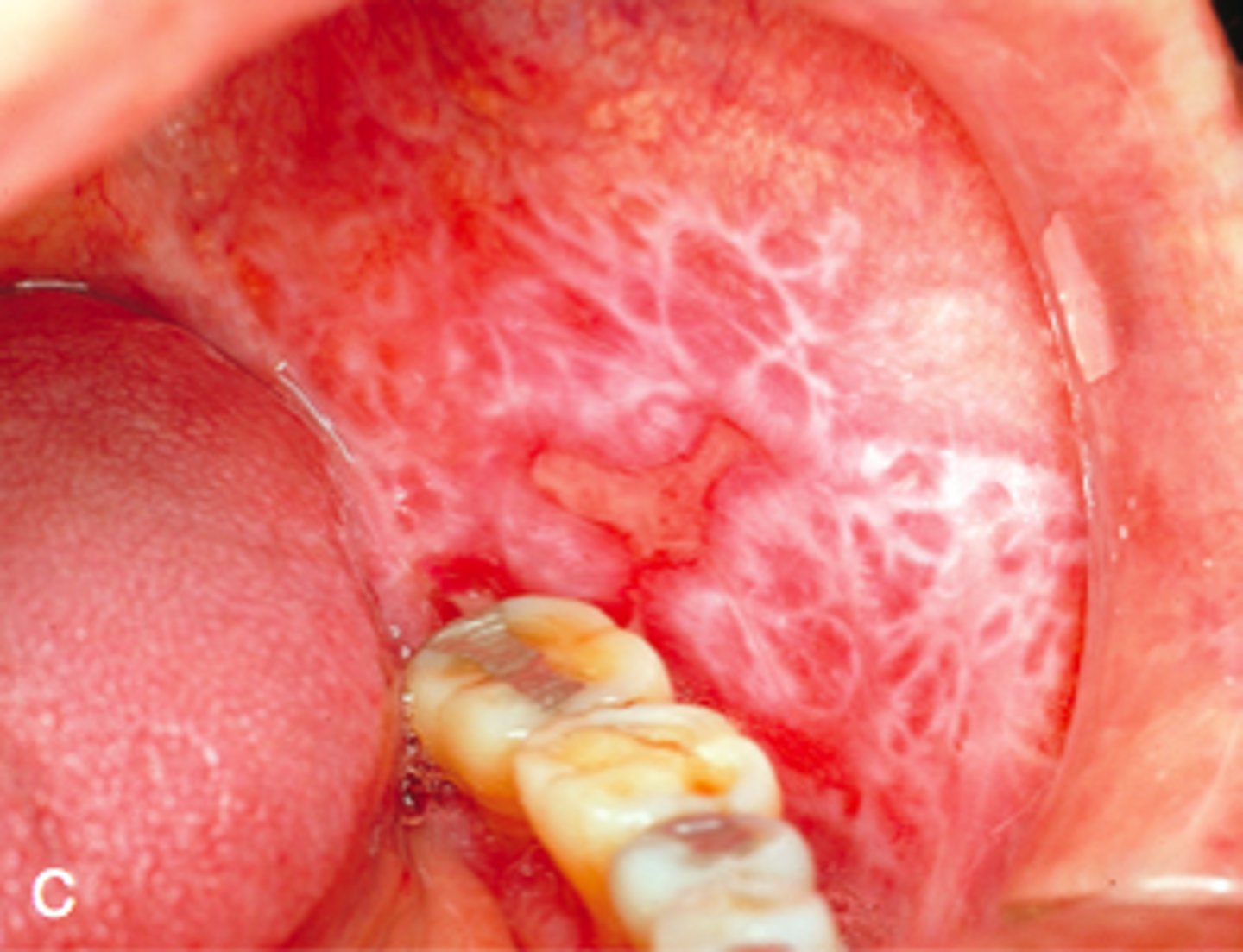
113
Which sites are more commonly affected by Oral Lichen Planus
Buccal Mucosa and the Tongue
Lesions tend to be Bilateral.
New cards
114
What are the 6 clinical subtypes of Lichen Planus
1) Reticular
2) Plaque Like
3) Atrophic
4) Erosive
5) Papular
6) Bullous
New cards
115
How does Lichen Planus present
violaceous, flat-topped, polyclonal papules. May have Wickham's striae (white stripes) on mucous membranes. Associated with Koebner's phenomenon

New cards
117
What is Pemphigus
an autoimmune disease in which antibodies are produced against Desmosomes in skin, leading to extensive blistering and intradermal separation

New cards
118
Which antigens does Auto-Antibodies in Pemphigus target
Desmoglein I and III
New cards
120
Describe the intraoral presentation of Pemphigus
Intraoral manifestation is often the first presentation of Pemphigus
Lesions are very fragile and breakdown rapidly
Formation of Irregular Ulcers with ragged Edges
New cards
121
In Oral Pemphigus, the Nikolsky Sign may be positive.
What is the Nikolsky Sign
The sign is demonstrated when lateral pressure is applied on the border of an intact blister, which results in the dislodgment of the normal epidermis and extension of the blister.
Where minor trauma can cause separation of mucosal layers.
New cards
123
What is Pemphigoid
Autoimmune Blistering Disease where autoantibodies attack proteins at the basement membrane causing separation of the dermis and epidermis.

New cards
126
What are 3 types of Pemphigoid
1) Bullous Pemphigoid
2) Mucous Membrane Pemphigoid
3) Gestational Pemphigoid
New cards
127
What is the Oral Presentation of Pemphigoid
Affects mainly the elderly > 60 years of age
Bullae formed are more resilient and present intact
Bullae rupture to cause ragged erosions

New cards
128
What is the Skin Presentation of Pemphigoid
Often starts with a itchy urticarial rash on trunk and limbs which progress to form Bullae after a few days.
Initially which is filled with straw coloured fluid and then bullae may later get filled with blood.
Bullae may coalesce before bursting and when ruptured they form extensive areas of painful ulcerated crusted skin.
New cards
129
What is Dermatitis Herpetiformis
Cutaneous Manifestation of Coeliac Disease characterised by a deposition of IgA within the connective tissue papillae.
New cards
130
What is the Oral presentation of Dermatitis Herpetiformis
Fragile Vesicles affecting palatal mucosa
Keratotic patches that resemble mild lichen planus
Frequent oral ulcerations
New cards
131
What is the Skin presentation of Dermatitis Herpetiformis
Symmetrical Distribution commonly appearing on Scalp, Shoulders, Buttocks, Elbows and Knees
Very itchy papules and vesicles on normal skin.
Lesions often occur in clusters or snake like patterns
Blisters often burst and become crusted due to immediate scratching

New cards
132
What is Epidermolysis Bullosa
Chronic, non-inflammatory skin disease
Rare but serious groups of blistering disorders. Inherited.
Four Major Subtypes distinguished
New cards
133
What is the Oral Presentation of Epidermolysis Bullosa
Predominantly in the Junctional and Dystrophic subtypes of Epidermolysis Bullosa
Extremely fragile Oral Mucosa
Bullae breakdown to form painful erosions
Can cause Trismus and Dental Anomalies including Hypoplastic Tooth Formation

New cards
134
What is the Skin Presentation of Epidermolysis Bullosa Simplex (2)
1) Bullae Commonly on Hands, Feet and Extremities
2) Thickened plaques develop on palms and soles. Limit finger function and interfere with joint movement
New cards
135
What is the Skin presentation of Junctional Epidermolysis Bullosa
Bullae Appear over the body, widespread soon after birth. Death occurs in early infancy due to sepsis
New cards
136
What is the skin presentation of Dystrophic Epidermolysis Bullosa
Blistering involving large areas of the skin, scarring and deformity to fingers and toes.
Fingers may fuse to form mitten hands.
Survivors at risk of developing Squamous Cell Carcinoma within chronic wounds.
New cards
137
What is Systemic Sclerosis
Autoimmune disorder characterized by chronic inflammation, destruction of small vessels and progressive tissue fibrosis.
Progressively Tightening and Hardening of Skin

New cards
138
What are the three subtypes of Systemic Sclerosis (3)
A) Limited Cutaneous Systemic Sclerosis (Face and Distal Limb)
B) Diffuse Cutaneous Systemic Sclerosis (Trunk with Internal Organ involvement)
C) Scleroderma (internal organs)
New cards
139
What is Systemic Lupus Erythematous
Autoimmune Chronic Inflammatory Disease affecting skin and internal organs
New cards
140
What is the Oral presentation of Systemic Lupus Erythematous
Erythematous Patches and Oral Ulceration

New cards
141
What is the Skin Presentation of Systemic Lupus Erythematous
Malar or Butterfly Rash sparing Nasolabial Folds
Generalised Rash triggered by Sun Exposure

New cards
142
What is Discoid Lupus Erythematous
Autoimmune Driver Chronic Inflammatory Condition unlike Systemic Lupus Erythematous, this has not Systemic Effects.
New cards
143
What is the Oral Presentation of Discoid Lupus Erythematous
White Papules with Central Erythema
Oral Lesions are rare without Skin Signs
New cards
144
What is the Skin Presentation of Discoid Lupus Erythematous
Well Demarcated Scaly Erythematous Papules, most commonly affecting the face and scalp.
Lesions become either hypopigmented or hyperpigmented before finally scarring.
New cards
153
What is the Oral Presentation of Palmoplantar Keratoderma
High Arched Palate, Lingual Ridging and Fissuring, Hyperkeratotic Mucosal Plaques.

New cards
155
What is Darier's Disease
A congenital autosomal dominant skin disorder due to genetic mutations, disruption of calcium movement within the cells leading to fragility in the adhesion of kertainocytes
New cards
156
What is the oral presentation of Darier's Disease
Asymptomatic confluent white patches affecting the palate and buccal mucosa
New cards
159
What is Type I Hypersensitivity reactions mediated by
IgE
New cards
160
What are Type IV mediated Hypersensitivity Reactions mediated by
T Lymphocytes
New cards
163
What are the Severe Symptoms of Type I Hypersensitivity (5)
1) Increased Vascular Permeability (Swelling)
2) Airway Constriction
3) Angioedema
4) Cardiovascular Collapse
5) Anaphylactic Shock (Very Severe end of Spectrum)
New cards
167
What are the oral manifestations of Erythema Multiforme
Widespread painful blistering and erosions to the mucosa
Characteristic haemorrhagic crusting to lips
New cards
171
Which Viruses can cause Liver Disease
Hepatitis B
Hepatitis C
New cards
173
Describe the Role of the Liver
Liver Produces Bile which is excreted into the Bile Duct, Stored in the Gall Bladder and Excreted in the Duodenum.
New cards
175
Patients with Liver Disease may also have Haemolytic Anaemia.
Why?
Red Blood Cells are not sturdy as healthy Red Blood Cells so they get broken down in the spleen so there is a higher turnover of Red Blood Cells.
New cards
177
Splenomegaly may occur in Patients with Haemolytic Anaemia. Explain Why.
The Spleen is grossly enlarged in patients with Haemolytic Anaemia.
New cards
178
Why may Removal of the Spleen be disadvantageous
Weakens the Immune System
New cards
179
Describe what happens to the size of the Liver in Liver Disease
The Liver can reduce in size. Therefore there is Less Tissue so it cannot process as much.
New cards
180
What is the main cause of too little Liver
Cirrhosis
New cards
181
What is Cirrhosis
scarring of the liver
New cards
182
Describe the differences between a Cirrhotic Liver and Healthy Liver
In Health, the Liver should be smooth. A Cirrhotic Liver has lots of little nodules and rough appearance
New cards
184
How does Cirrhosis occur?
Damage to Liver Cells causes Inflammation. Liver Cells can regenerate. However if continuous long term damage to liver cells occurs you get Healing by Fibrosis leading to Cirrhosis.
New cards
188
What is Hep A
Hep A causes an Acute Infection of the Liver. If a patient recovers from a Hep A infection, their immune system will clear the virus.
However with Chronic Hepatitis Infections, the body does not clear the virus and instead produces an inflammatory response to it.
New cards
189
What is the effect of Alcohol on the Liver
Alcohol Damages the Liver. However if short periods of Alcohol are consumed then the Liver may be able to Regenerate.
Long Term Alcohol Consumption in High Amounts will cause Cirrhosis
New cards
192
What are the Consequences of Cirrhosis (4)
1) Liver Failure
2) Portal Hypertension
3) Ascites
4) Hepatocellular Cancer
New cards
195
What are the Effects of Portal Hypertension
1. esophageal varices → hematemesis + melena
2. peptic ulcer → melena
3. splenomegaly
4. caput medusae, ascites
5. portal hypertensive gastropathy
6. hemorrhoids
New cards
196
Portal Hypertension leads to the formation of Varices.
Where do the Varices commonly form
Stomach and Rectum
Stomach Varices can bleed and people with Cirrhosis come into Casuality vomiting blood.
New cards
197
How does Cirrhosis cause Portal Hypertension
Abnormal structure of liver, impedes blood flow.
The nodules of regenerative cells are aligned in groups and not along the capillaries
Some blood vessels may end in blind endings and as a result it is difficult to push blood through the liver raising the blood pressure in the portal venous system.
New cards
199
Cirrhosis can cause a Low Albumin Production which leads to Ascites.
Explain How.
Liver produces Albumin which is a common Plasma Protein in Blood. Albumin plays a role in absorbing Water back into the Blood at the Venous End of the Capillaries.
If there is Low Albumin, then less Water will be absorbed back into the blood. This leads to Fluid in the Peritoneal Cavity commonly known as Ascites.
New cards
204
What can block the flow of Bile from the Bile Duct into the Duodenum (2)
1) Gall Stones
2) Tumour at the Bottom of the Bile Duct.
New cards
205
How can you differentiate between Pancreatic Carcinomas and Gall Stones.
Patients with Pancreatic Carcinoma produce Painless Progressive Jaundice. If the Patient turns Yellow without any pain it is most likely a Tumour at the Bottom of the Bile Duct or Head of the Pancreas.
Gall Stones are Painful
New cards
206
What is Pre-Hepatic Jaundice
Too Much Work For the Liver to Do
New cards
207
What is Hepatic Jaundice
Due to liver disease (cirrhosis, cancer, hepatitis, etc.)
Too Little Liver tissue to do the Work
New cards
208
What is Post Hepatic Jaundice
Obstructive Blockage in the Bile Duct.
New cards
209
What are the 3 routes of Flow in and out of the Liver
1) Arterial & Venous Blood Flow. (Hepatic Artery & Hepatic Vein)
2) Portal Circulation (From Gut to the Liver, Blood here is poor in Oxygen but has lots of nutrients)
3) Bile Flow (From Liver to Gut to help Digestion)
New cards
211
What are the 4 main vessels in the Liver
1) Hepatic Artery
2) Hepatic Vein
3) Hepatic Portal Vein
4) Bile Duct
New cards
212
Describe the Microanatomy of the Liver
The Liver is Organised into Hexagonal Lobules with a central Hepatic Vein.
The Hepatic Portal Vein, Hepatic Artery and Bile Duct form the Portal Triad.
The Flow of Bile is opposite to that of Blood Flow.
New cards
213
What are the Functions of the Liver (7)
1) Detoxification - Filters and Cleans Blood
2) Immune Function
3) Synthesis of Clotting Factors, Proteins, Enzymes, Glycogen etc.
4) Production of Bile and Breakdown of Billirubin
5) Energy Storage (Glycogen & Fats)
6) Regulation of Fat Metabolism
7) Ability to Regenerate.
New cards
216
How can Liver Injuries be Categorised (5)
Liver Injuries can be categorised based on their
i) Timeline (Acute or Chronic)
ii) Pattern (Hepatic, Cholestatic or Mixed)
iii) Presentation (Asymptomatic vs Symptomatic)
iv) Severity (Cirrhotic or Non-Cirrhotic)
v) Cause
New cards
217
What are the different Types of Acute Liver Injuries
1) Viral Causes (A, B & E, EBV)
2) Acute Liver Failure
Acute Liver Injuries can lead to recovery. Acute Liver Failure requires Emergency Treatment
New cards
218
What are the different types of Chronic Liver Injuries
1) Cirrhosis
2) Viral Causes (B & C)
3) Alcohol Induced
4) Autoimmune
These can lead to Chronic Liver Failure which can cause Decompensated Cirrhosis leading to Varices and Hepatoma.
New cards
219
How does an Acute Liver Injury Present (6)
1) Asymptomatic
2) Abnormal Liver Function Tests (LFTs) and Coagulopathy
3) Malaise, Nausea and Anorexia
4) Jaundice
5) Bleeding & Liver Pain
6) Confusion
New cards
220
How does a Chronic Liver Injury Present (9)
1) Loss of Appetite, Shortness of Breath, Nausea
2) Abnormal Liver Function Tests (LFTs)
3) Hepatomegaly
4) Malaise & Abdominal Discomfort
5) Itching, Wasting and Anorexia
6) Ascites and Oedema in Legs
7) Confusion
8) Jaundice
9) Easy Bruising and Haematemesis due to Varices
New cards
222
What is LFTs composed of (7)
Several Different Tests Looking for
1) Decreased Albumin
2) Increased Alkaline Phosphatase (ALP)
3) Increased Gamma GT (GGT)
4) Increased Alanine Aminotransferase (ALT)
5) Increased Asparate Aminotransferase (AST)
6) Increased Bilirubin
7) Globulin
New cards
223
To diagnose a Liver Injury, Platelet Count and INR/Prothrombin Time are measured.
Explain Why
Liver is the site of synthesis of fibrinogen and factors II, V, VII, IX, X, XI, and XII
If the Prothrombin Time is increased, there is a increased risk of Bleeding.
New cards
224
What is the cause of Jaundice
high levels of bilirubin in the blood
New cards
226
What is Billirubin
Breakdown Product of Haemoglobin
It is metabolised in the Liver and Excreted via the Intestine.
New cards
227
What is the effect of Bilirubin on Faeces
If Bilirubin rises and is not excreted, the faeces turn pale.
New cards
228
What are the 3 Causes of Jaundice
1) Pre-Hepatic
2) Hepatic
3) Post-Hepatic
New cards
229
What is the Pre-Hepatic Cause of Jaundice
Haemolysis caused by a increase in substrate i.e. breakdown of haemoglobin.
New cards
230
What are the Hepatic Causes of Jaundice
Intrinsic Liver Disease
- Cirrhosis
- Infiltration of the Liver by Tumours
- Acute Hepatitis (Viral Alcoholic, Autoimmune, Drug Induced)
New cards
231
What are the acute causes of Hepatitis (4)
1) Viral
2) Alcohol
3) Autoimmune
4) Drug-Induced
New cards
232
What are the Post-Hepatic Causes of Jaundice
1) Gallstones
2) External Compression i.e. Pancreatitis, Lymphadenopathy, Pancreatic Tumour, Ampullary Tumour.
New cards
234
Which Drugs can induce Chronic Liver Disease (3)
1) Amiodarone
2) Chemotherapy
3) Antibiotics
New cards
237
How is Alcoholic Liver Disease diagnosed
Reduced Levels of Vitamin D, Platelets and Folic Acid.
New cards
239
How is Viral Hepatitis Diagnosed
diagnosis of viral hepatitis can only be made by testing patients' serum for the presence of specific viral antigens and/or anti-viral antibodies for the various hepatitis viruses
New cards
240
How is Genetic Liver Disease diagnosed
Haemochromatosis Genotyping.
New cards
247
What is the difference between Compensated and Decompensated Cirrhosis
Compensated is asymptomatic
Decompensated is Symptomatic.
New cards
249
How is the Severity of Cirrhosis assessed
CPS (Child Pugh Score) ad MELD Tests
New cards
250
What factors determine the Prognosis of Cirrhosis (5)
1) Bilirubin
2) Albumin
3) Presence of Ascites
4) INR
5) Presence of Encephalopathy
New cards
255
What are the causes of Non-Cirrhotic Portal Hypertension (NCPH)
Due to Vascular Problems in the Liver. Can be caused by Previous Chemotherapy.
Patients with NCPH tolerate bleeding well and clotting is generally intact.
New cards
257
How can a Compensated Cirrhotic Liver be Diagnosed
1) Asymptomatic
2) Blood can be Normal
3) The Risk to Dental Work is Low
Compensated Liver Disease are difficult to spot. Patients do not look or feel ill.
New cards
259
Why is it important for effective Long Term Management of Cirrhosis
Staging and Assessing rate of Cirrhosis change accurately is the key to long term management.
New cards
260
What 4 Factors worsen the Prognosis of Cirrhosis
1) Malnutrition
2) Variceal Bleeding
3) Infection
4) Renal Failure
New cards
263
What is NAFLD
Non-alcoholic fatty liver disease
New cards
265
What are the Signs and Symptoms of Chronic Liver Disease (7)
1) Palmer Erythema (Reddening of the Palms)
2) Spider Naevi (Red Spots)
3) Gynaecomastia (Swelling or Enlargement of Male Breasts) - Can be due to Reduced Testosterone or Drug Related i.e. Spironolactone.
4) Leuconychia - White Nails due to Low Albumin
5) Fingernail Clubbing (Also present in Lung and CVD)
6) Jaundice
7) Ascites (Sign of Decompensated Cirrhosis)
New cards
266
What is Hepatic Encephalopathy
a decline in brain function that occurs as a result of severe liver disease. In this condition, your liver can't adequately remove toxins from your blood. This causes a build up of toxins in your bloodstream, which can lead to brain damage.
New cards
267
What is Hepatic Encephalopathy a feature of
Decompensation
Indicates underlying problem i.e. Bleed, Infection Constipation or Worsening Chronic Disease.
New cards
270
What is the Symptomatic Treatment of Liver Disease
1) Diuretics
2) Nutrition Support
3) Supplements
4) Propranolol
New cards
272
What is the Specific Treatment for Liver Disease
1) Antivirals
2) Immunosuppression
3) Relieving Obstruction
4) Venesection
New cards
274
Which Drugs should caution be used when prescribing Medications that are metabolised in the Liver
1) Anaesthetics
2) Antiplatelets (Stop Aspirin 7 days before)
3) Increased Drug Induced Liver Injury with Flucloxacillin and Co-Amoxyclav
4) Sedatives (Long Acting Benzodiazepines and Barbiturates)
New cards
275
Which Drugs Increase the Toxicity in Patients with Advanced Liver Disease
Avoid NSAIDs,
Paracetamol is Safest Painkiller in Liver Disease.