nha pharmacy technician notes
Module One – Early History of Pharmacy
Ancient China
Shennong (also called Emperor Shen Nong) tested the medicinal value of hundreds of herbs.
He wrote the Pen Ts’ao, which recorded 365 medications.
Ancient Chinese pharmacy practices date back to around 2900 BC.
Ancient Egypt
The Ebers Papyrus contained about 800 prescriptions and mentioned over 700 medications.
Ancient India
The Charaka Samhita was written around 1000 BC by multiple authors and became a foundational medical text in Ayurveda.
Ancient Greece
Terra Sigillata (“sealed earth”) was one of the first therapeutic agents to carry a trademark-like seal.
Ancient Rome
Mithridates VI, King of Pontus, studied poisons and developed antidotes.
Pedanius Dioscorides wrote De Materia Medica, a major reference on medicinal substances.
Galen of Pergamon taught pharmacy and medicine in Rome and influenced medical practice for centuries.
Module One subone – TIMELINE
Middle Ages and the Islamic Golden Age
Middle Ages (Europe): 6th–16th century
Islamic Golden Age (Middle East): 8th–14th century
Major Developments in Pharmacy
Monastic Medicine in Europe
Monks worked with herbs and preserved medical knowledge.
Role Separation in the Middle East
Clear roles developed between:
Physician (diagnosed illness)
Apothecary (prepared and dispe
nsed medicines)
Separation of Pharmacy & Medicine in Europe
In 13th-century Sicily, pharmacy and physician responsibilities were officially separated.
Development of the Pharmacy Workplace
The first drug shops appeared in Baghdad in the 8th century.
Similar apothecary shops spread across Europe in the 12th–15th centuries.
These shops compounded and distributed chemical preparations.
A time of renewed interest in art, culture, and science.
Scientific thinking and professional organization increased.
The Renaissance (16th century to 17th century) Organization of Pharmacists in England
In 1617, the first pharmacy organization was created in England:
Worshipful Society of Apothecaries
Official title: Master, Wardens and Society of the Art and Mystery of the Apothecaries of the City of London
This helped formalize and regulate the practice of pharmacy.
Pharmacy in the American Colonies
In 1640, John Winthrop, the first governor of the Massachusetts Bay Colony and founder of Boston:
Sold imported medications
Prepared medicines from plants found in New England
This marked one of the earliest organized pharmacy practices in the American colonies.
Colonial North America Pharmacy
Early Apothecaries
1729: Christopher Marshall opened an apothecary shop in Philadelphia.
His granddaughter became the first female pharmacist in America.
Hospitals and Prescriptions
1751: First hospital in Philadelphia established by Benjamin Franklin.
John Morgan:
First to support the use of written prescriptions in the colonies.
Pharmacy in the Military
Andrew Craigie:
First man to hold a commissioned pharmacy officer position in the US Army.
Later became the first Apothecary General.
Twenty-First Century Pharmacy
Evolving Roles
Pharmacist: Now authorized to immunize patients and provide direct patient care.
Pharmacy Technician: Assists pharmacists by obtaining detailed patient records, helping with immunizations, and performing other tasks depending on state laws and regulations.
Expanded Pharmacy Practices
Medication Therapy Management (MTM):
Works with care management plans for patients in chronic care programs.
Aims to achieve optimal therapeutic outcomes.
Medication Reconciliation:
Process of reviewing a patient’s medications alongside what they are already taking.
Helps prevent medication errors.
Recognition and Integration
Pharmacy technicians are increasingly recognized as important healthcare providers.
Technicians often interact with programs like Medicare and Medicaid to support patient care.
Summary – History of Pharmacy
Ancient Pharmacy
China (c. 2900 BC): Shennong tested herbs, wrote Pen Ts’ao documenting 365 medications.
Egypt: Ebers Papyrus recorded ~800 prescriptions and 700 medications.
India (c. 1000 BC): Charaka Samhita became a foundational Ayurvedic medical text.
Greece: Terra Sigillata (“sealed earth”) was an early trademarked therapeutic agent.
Rome: Mithridates VI studied poisons; Pedanius Dioscorides wrote De Materia Medica; Galen taught pharmacy and medicine.
Middle Ages & Islamic Golden Age (6th–16th / 8th–14th c.)
Europe: Monks preserved knowledge and worked with herbs.
Middle East: Roles of physician and apothecary were formalized.
Europe: 13th-century Sicily separated pharmacy and physician responsibilities.
Pharmacy Workplace: First drug shops appeared in Baghdad (8th c.), spreading to Europe (12th–15th c.).
The Renaissance (16th–17th c.)
Renewed interest in science and organization.
England (1617): Worshipful Society of Apothecaries formalized pharmacy practice.
American Colonies (1640): John Winthrop sold imported and locally prepared medicines.
Colonial North America
1729: Christopher Marshall opened Philadelphia apothecary; granddaughter became first female pharmacist.
1751: First hospital in Philadelphia established by Benjamin Franklin.
John Morgan: Promoted written prescriptions.
Andrew Craigie: First commissioned pharmacy officer in US Army; first Apothecary General.
Twenty-First Century Pharmacy
Pharmacist: Provides direct patient care, including immunizations.
Pharmacy Technician: Supports pharmacists with patient records, immunizations, and other tasks; roles vary by state.
Expanded Practices:
Medication Therapy Management (MTM): Optimizes therapy in chronic care.
Medication Reconciliation: Reviews all patient medications to prevent errors.
Recognition: Technicians increasingly seen as healthcare providers; interact with Medicare and Medicaid programs.
Module 9 - Managed Care Prescriptions
Third-Party Programs
Over 85% of prescriptions are paid in full or in part by third-party programs.
“Third party” refers to programs—both private and government-run—that pay for prescriptions on behalf of patients.
The term comes from the three parties involved:
The patient (PT) who receives the service
The provider who delivers the service (e.g., pharmacy)
The payer who pays for all or part of the service (insurance or government)
Payment Interactions
Payments among these three parties are interdependent.
The patient may pay a portion of the prescription cost, often called a copayment, and may also pay insurance premiums.
If insured through an employer:
The employer pays the majority of the insurance cost.
The employee pays the remaining portion of the premium (deducted from their paycheck as nontaxable income).
The insurance company (third party) pays the pharmacy directly on behalf of the patient.
Types of Insurance Plans
Indemnity Plans
Reimburse the insured individual for medical expenses incurred.
The patient often pays upfront and then is reimbursed.
Managed Care Plans
Pay the healthcare provider directly for services rendered.
Focus on cost control and coordinated care.
Sponsorship of Plans
Employer-Sponsored Plans
Available to eligible employees and their dependents.
Costs of premiums are shared between employer and employee.
Government-Sponsored Plans
Funded by state or federal programs, either fully or partially.
Private Plans
Chosen and paid for by the individual for themselves and eligible dependents.
PPI
Patient - Pharmacy - Insurance
Indemnity → Patient reimbursed
Managed care → Direct to provider
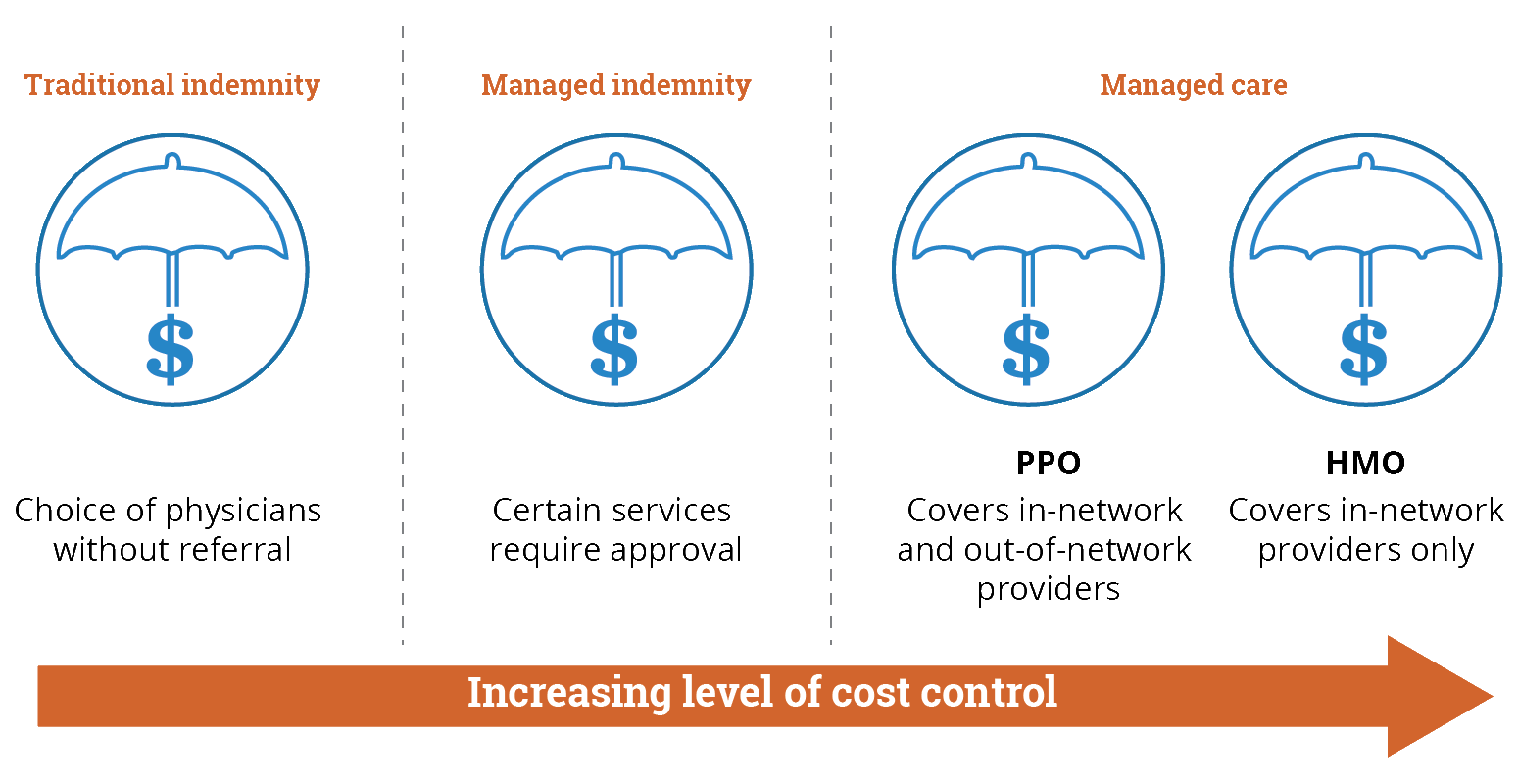
1. Traditional (Fee-for-Service / Indemnity) Plans
Also called indemnity plans.
Patients can choose any healthcare provider.
The insurance reimburses the patient for medical expenses after the service is received.
Usually involves higher out-of-pocket costs and less control over cost management.
Scenario: Jane goes to her local pharmacy to fill a prescription.
Process: She pays the full cost upfront ($100) and then submits a claim to her insurance company.
Outcome: Her insurance reimburses her $80, so her out-of-pocket cost is $20.
Key point: Jane can choose any pharmacy or doctor, but she handles the payment first.
2. Managed Indemnity Plans
A hybrid between traditional indemnity and managed care.
Patients still have flexibility in choosing providers, but there are some cost controls (like network discounts or pre-authorization requirements).
Designed to reduce costs while maintaining some freedom of choice.
Scenario: Mike visits a specialist for a chronic condition.
Process: He can choose any provider, but the insurance plan requires pre-authorization for certain tests. The specialist charges $200.
Outcome: Insurance reimburses $150 after approval, leaving Mike with $50 out-of-pocket.
Key point: Mike has flexibility, but the plan controls costs and requires some rules to reduce unnecessary expenses.
3. Managed Care Plans
Includes Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs), and Point of Service (POS) plans.
The insurance pays providers directly rather than reimbursing patients.
Focus on coordinated care, preventive services, and cost control.
Often requires patients to use in-network providers to get the full benefits.
Scenario: Sarah has an HMO plan and needs a flu shot.
Process: She goes to a clinic that is in-network. The clinic bills the insurance directly. Sarah only pays a $10 copay.
Outcome: No reimbursement process is needed; her out-of-pocket cost is minimal.
Key point: Managed care plans directly pay providers, focus on cost control, and require use of approved networks.
Pharmacy Benefit Managers (PBMs)
Also known as PBMs.
PBMs are intermediaries between pharmacies, insurers, and patients.
Their main roles include:
Contracting with pharmacies
Facilitating communication between pharmacies and insurers
Auditing pharmacy activities
Controlling and managing prescription benefits
Pharmacy Enrollment
PBMs enroll pharmacies through a participating pharmacy agreement.
This contract specifies:
Which pharmacy services will be provided
Reimbursement rates for those services
Non-Participating Pharmacies
If a pharmacy is not part of the patient’s PBM network:
The patient must pay cash upfront for prescriptions
The patient can then submit a claim form to the PBM or insurance for potential reimbursement
1. Government Programs
Includes programs such as:
Medicare
Medicaid
TRICARE (for military personnel and their families)
Workers’ Compensation
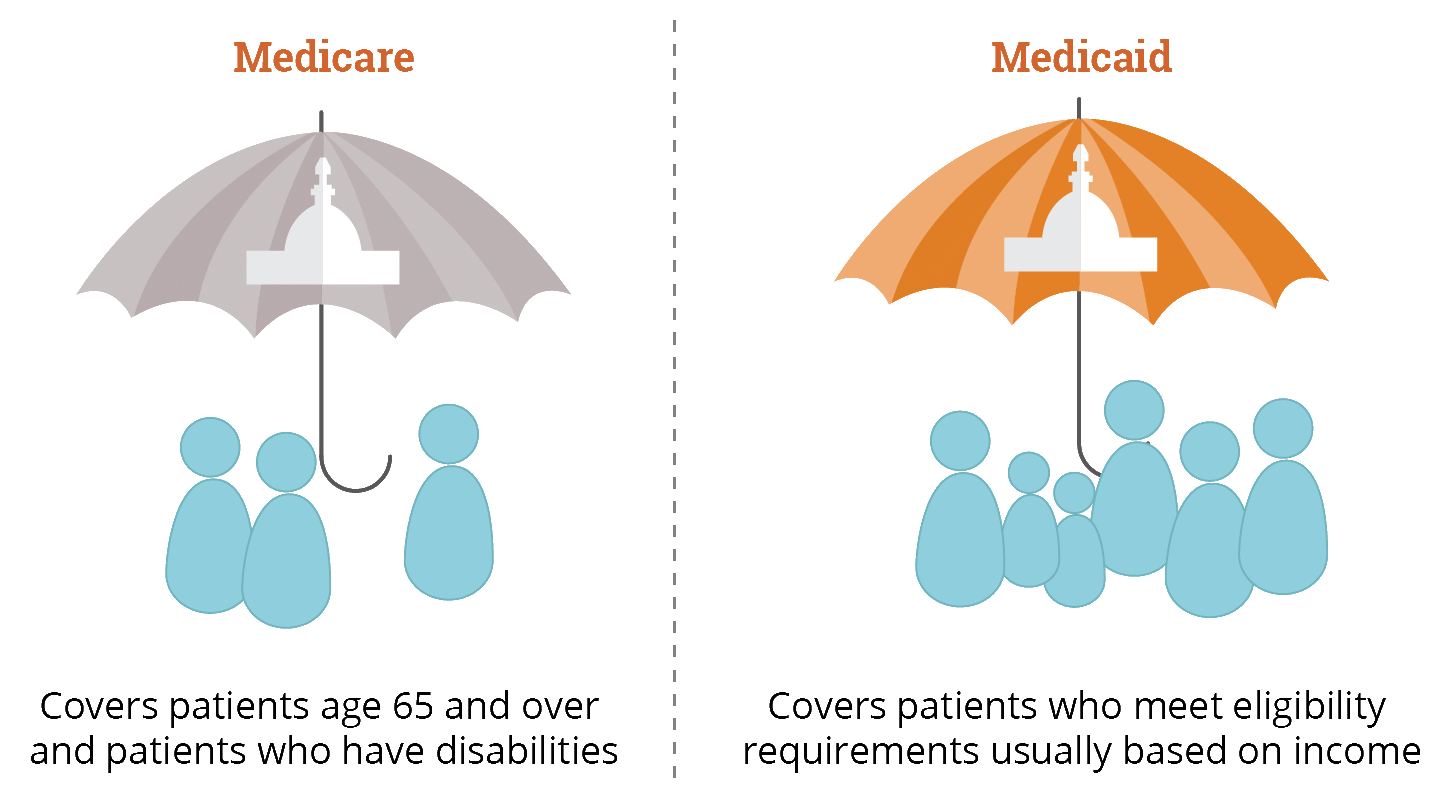
Medicaid
Prescription coverage is optional, and each state decides which medications to cover.
Accounts for more than 1 in 10 prescriptions in the U.S.
Patients who were previously eligible for both Medicaid and Medicare now often receive prescription coverage through Medicare Part D.
Medicare
Voluntary program primarily for individuals 65 and older or with certain disabilities.
Requires payment of premiums and sharing some costs (like copays or coinsurance). Low-income patients may have reduced costs.
Enrollment is required during specific enrollment periods; late enrollment can result in higher premiums.
Patients pay a monthly premium and meet a deductible before insurance coverage begins.
Coverage gap (“donut hole”): occurs when the patient must pay out-of-pocket for medications not covered by the plan until a certain threshold is reached.
This gap shrinks each year due to legislative changes.
2. Private Insurance
Often part of employer-sponsored health benefits.
Includes individual or family plans purchased privately.
Since the Affordable Care Act (ACA, 2010):
More people have access to health insurance
Health plans must cover essential health benefits, including prescription drugs
Plans cannot deny coverage for pre-existing conditions
Private insurance may include copays, deductibles, and coinsurance similar to government plans.
Many prescription errors are caused by incorrect data entry. Pharmacy technicians must carefully double-check all data entry points to ensure accuracy. Even small mistakes can lead to claim rejections or delays.
Some claim rejections may indicate that a prior authorization (PA) is required. When this happens, the prescription cannot be approved until additional steps are completed.
A prior authorization is a process required by insurance companies to review certain medications before they are covered. The Pharmacy Benefit Manager (PBM) evaluates the request and can either approve or deny the claim.
If a medication is not normally covered, the prescriber must provide additional documentation explaining the medical necessity of the drug. Based on this information, the PBM will determine whether to approve coverage. In some cases, the prescriber may choose to change the prescription to a medication that is covered by the patient’s insurance plan.
Potential Reasons for a PBM Prior Authorization Request
A prior authorization (PA) may be required by a Pharmacy Benefit Manager (PBM) for several reasons:
The medication is not on the third-party payer’s formulary.
A generic alternative is available, and the brand-name drug was prescribed.
The medication may be used for cosmetic purposes and not considered medically necessary.
The medication is treating a non–life-threatening condition when alternative treatments are available.
The prescribed dosage does not follow recommended dosing guidelines.
The cost of the medication exceeds the plan’s established maximum limit.
The prior authorization (PA) process can delay medication dispensing for several days while the Pharmacy Benefit Manager (PBM) reviews the request.
These delays may cause:
Patient anxiety
Confusion
Interruption in therapy
To help prevent delays, the pharmacy technician should:
Notify the prescriber promptly when a PA is required
Encourage early contact between the prescriber and the PBM
Document communication to ensure follow-up
Starting the process early can reduce wait time and improve patient satisfaction.
How the NDC Works
The NDC has 3 parts:
Labeler Code – Identifies the manufacturer or distributor
Product Code – Identifies the specific drug (strength, dosage form, formulation)
Package Code – Identifies package size and type
It usually appears in an 11-digit format for billing (5-4-2).
Example format:
Labeler – Product – Package
12345-6789-01