exam 1 study guide (Ch 42, Ch 1, Ch 13, Ch 38, Ch 5)
phases of nursing process
assessment
systematic, dynamic way to collect and analyze data about a client, the first step in delivering nursing care
includes not only physiologic data, but also psychological, sociocultural, spiritual, economic, and life-style factors
types of data
cue
piece or pieces of data that often indicate that an actual or potential problem has occurred or will occur
subjective
information that is provided by the patient
such as symptoms
objective
observable and measurable signs
such as signs
sources of data
primary source
from the patient
secondary source
include family members, significant others, medical records, diagnostic procedures, and previous nursing progress notes
methods of data collection
interview or nursing health history
Information about patient’s health history
biographic data
provide information about the facts or events in a person’s life
includes reason the patient is seeking health care, a history of the present illness, the health history, and the family history
environment
patient lives and works often plays a part in the patient’s health status
physical exams
guided by subjective data provided by the patient
diagnosis
identify the type and cause of a health condition
physician or other medically qualified health care provider
nursing can provide a medical diagnosis
LVN/LPN and RN observes and collects data
initial assessment completed and data requires analysis
RN responsible for analyzing and interpreting data to identifying data to identify health problems that the nurse treats and is the nursing diagnosis or patient problem statement
nursing diagnosis and patient problem statement is a type of health problem that can be identified by the nurse
nursing diagnosis provides basis for selection of nursing interventions to achieve outcomes for which the nurse has accountability
nursing diagnosis is a clinical judgment concerning a human response to health conditions and life processes, or a vulnerability for that response, by an individual, family, group or community
patient problem statement is used to guide the development of a nursing care plan
types includes actual or potential
Actual patient problem statement
Identifies health-related problems that exist and are discovered during the nursing assessment
Educational setting - 3 part statement
1 - the patient problem statement
2 - the contributing, etiologies, or related factor
3 - specific cues, signs, and symptoms from the patient’s assessment that support the patient problem statement
Potential patient problems statements
Health-related problems that the nurse deems as having a strong possibility of occurring
Nursing assessment indicates is factors that are present and known to contribute to the development of the problem
2 parts statement
1 - the patient problem statement with the adjective “potential” in front of it
2 - risk factors
Health promotion patient problem statement
Refers to the willingness of the patient, caregiver, or significant others to participate in activities that will aid in keeping the patient well
Statements are identified with the adjective “willingness”
If patient’s condition is expected to change, did phrase “potential for”
Adjectives add meaning to the patient problem statement by describing or modifying the statement
Chronic conditions
Things that are always present or consistently recur
Last 3 months or longer
Labeled as either chronic or prolonged
Acute problems
Typically rapid onset and are limited in the duration of time
Can become chronic if condition is not resolved
Labeled as acute or recent
Developments of a problem
Include contributing, etiologies, and related factors
These factors are written as “related to” in actual patient problem statement
Defining characteristics
Clinical cues, signs, and symptoms that furnish evidence that the problem exists
Cues, signs, and symptoms identified in patient’s assessment are written as “evidenced by” in patient problem statement
Types of health problems
Collaborative problems
Health-related problems that the nurse anticipates based on the condition or diagnosis of a patient
Both health care provider-prescribed and nursing-prescribed interventions are used
Medical diagnosis
Identification of a disease or condition with the evaluation of physical signs, symptoms, patient interviews, laboratory test, diagnostic procedures, review of medical records, and patient history
outcomes identification/ goal identification
Indicates the degree of wellness desired, expected, or possible for the patient to achieve and contains a patient goal statement
Patient goal statement provides a description of the specific, measurable behavior (outcome criteria) that the patient will be able to exhibit in a given time frame after the interventions
Desired patient goal statement has 2 functions
Guide the selection of nursing interventions
Nursing interventions are selected to promote the achievement of the desired outcme
Goal statement establishes the measuring standard that is used to evaluate the effectiveness of the nursing interventions
Well-written patient-centered goal statement
Uses the word patient or part of the patient as the subject of the statement
Uses a measurable verb
Is specific for the patient and the patient’s problem
Does not interfere with the medical plan of care
Is realistic for the patient and the patient’s problem
Includes a time frame for patient reevaluation
Because the subject of the patient goal statement is meant to be the patient or a part of the patient, the goal statement begins with “the patient will”
Measurable verbs indicate precise behavior that the nurse anticipates hearing or seeing
planning
Priorities of care are established and nursing interventions are chosen to best address the patient problem statement
Information typically communicated through the care plan so that all health care personnel directly involved in the care of the patient can follow the same plan, resulting in continuity of care
Priority setting
Priorities must be established to provide care for each patient
Once patient problem statements have been identified, the RN must prioritize the patient problem statements according to the patient’s current health status
Framework most often used to guide the prioritization is Maslow’s hierarchy of needs
Structure is based on the principle that lower-level needs must be met before higher-level needs can be satisfied
Physiologic needs are more vital than the safety and security needs, and the safety and security needs are more critical than the love and belongings needs
Actual problems often are ranked before potential problems, unless the potential problems, if they were to develop, are life threatening
Nurse can determine whether the actual or potential patient problem statements has the highest priority
Nurse also must take into consideration the patients thoughts and feelings regarding the prioritization of problems
Time factors and severity of illness are important considerations in determine which problems to initially address
Selecting nursing interventions
Nursing interventions
Those activities that promote the achievement of the desired patient goal
Interventions include that the nurse selects, in partnership with the patient, to resolve a patient problem, monitor for the development of a potential problem, or carry out physician orders
Nursing interventions are classified as physician prescribed or nurse prescribed
Physician prescribed
Actions ordered by a physician for a nurse or other health care professional to perform
Nurse prescribed
Any actions that a nurse is legally able to order or begin independently
Writing nursing interventions
Because nursing interventions offered in textbooks and care planning resources are often broad, general statements that indicate an activity to be performed, these nursing interventions must be converted to more specific instructional statements when writing a care plan for an actual patient
Communicating the nursing care plan
After completing the initial assessment, analyzing the data, writing the patient problem statement, selecting goals, and selecting appropriate nursing interventions
The nurse has the responsibility to communicate the detailed plan of care for the patient
Because the nursing staff constantly changes written guidelines are important for the continuity of patient care
Continuity increases patient trust in the nursing staff and promotes outcome achievement
Linear care plans vs concept maps
Linear care plan
Nursing faculty may require students to submit the care plan in a 4 column or 5 column format
Concept maps
Different shapes, and sometimes colors that are connected with lines when there is a relationship between 1 or more items
Beneficial for visual learners
implementation
Nurse and other members of the team put the established plan into action to goal achievement
Refers to actions that carry out the planned interventions established in the care plan
Evidence based interventions, the nurse should ensure that the plan is implemented in a timely and safe manner
Nurse process as a means of problem-solving is accelerated and nurse proceeds directly from assessment of the problem to intervention
Nursing interventions include nurse-prescribed and physician-prescribed activities
Evidence-based practice
A scholarly and systematic problem-solving paradigm that results in the delivery of high-quality health care
Gives meaning and provides rationale to nursing actions And provides accountability for the actions we as nurses implement on a daily basis
evaluation
Determination made about the extent to which the established goals have been achieved
Steps included
Review the patient-centered goals or desired patient outcomes that were established previously
These goal statements present standards and criteria that are observable and measurable
Reassess the patient to gather data that indicate the patient’s actual response to the nursing interventions
Compare the actual outcome with the desired outcome and make a critical judgment about whether the patient centered goal or desired patient outcome was achieved
experience does not matter for critical thinking but is not the sole reason
Signs and symptoms of inflammation and infection
Pyrexia
abnormal elevation of body temperature : fever
Infection
Caused by invasion of microorganisms that produce tissue damage
Examples - bacteria, viruses, fungi, or parasites
Inflammation
Protective response of body tissues to irritation, injury, or invasion by disease-producing organisms
Cardinal signs of infection and inflammation
Erythema (redness)
Edema (swelling)
Heat
Pain
Purulent drainage (pus)
Loss of function
Signs and symptoms of disease conditions
Ecchymosis
Discoloration of an area of the skin or mucous membrane caused by the extravasation of blood into the subcutaneous tissues as a result of trauma to the underlying blood vessels or by fragility of the vessel walls (also called a bruise).
Pruritus
A symptom of itching and an uncomfortable sensation that leads to an urge to scratch. Some causes are allergy, infection, jaundice, elevated serum urea, and skin irritation.
Purulent drainage (pus)
A creamy, viscous, pale yellow, or yellow-green fluid exudate that is the result of fluid remains of liquefied necrosis of tissues. Bacterial infection is the most common cause. The character of the pus, including its color, consistency, quantity, or odor, often has diagnostic significance.
Tachypnea (deals with pulse)
An abnormally rapid rate of breathing seen in many disease conditions.
bradycardia ( deals with respirations)
A circulatory condition in which the myocardium contracts steadily but at a rate of less than 60 contractions per minute.
Tachycardia ( deals with respirations)
An abnormal condition in which the heart contracts regularly but at a rate greater than 100 beats/min. The heart rate accelerates in response to fever, exercise, or nervous excitement.
Diseases caused by infections diseases
Types: acquired immunodeficiency syndrome (AIDS),tuberculosis (TB), measles, and pneumonia
Disease
a pathological condition of the body, is any disturbance of a structure or function of the body
Infectious disease
Result from the invasion of microorganisms into the body
objective data (select all apply question)
What is seen, hears, measures, and feels
Data includes laboratory findings and diagnostic imaging and other diagnostic studies
difference of subjective and objective data
Subjective
Symptoms - indications of illness that the patient perceives
Data includes what the patient tells the nurse about a symptom
Data collection from nurse encourages a full description by the patient of the onset, the course, and the character of the problem and any factors that aggravate or alleviate it
Descriptions of diseases
degenerative
Degeneration, often progressive, of some part of the body
Aging process may play a role
Example - osteoarthritis
metabolic
Caused by a dysfunction that results in a loss of metabolic control of homeostasis in the body
Dysfunction involves endocrine glands, which secrete hormones to regulate body processes
Example - diabetes mellitus
neoplastic
Abnormal growth of new tissues
New growth sometimes benign and sometimes malignant (cancerous)
Deficiency
Result from the lack of a specific nutrient
Nutrients are minerals, vitamins, proteins, fats, and carbohydrates
Example - iron deficiency anemia results from severe deficiency of iron
Risk factors for disease
Risk factor
Any situation, habit, environmental condition, genetic predisposition, physiologic condition, or other variable that increases the vulnerability of an individual or group to illness or accident
Major categories include
Genetic and physiologic
A family history of cancer increases the risk that an individual will have cancer develop (genetic).
Malnourishment predisposes an individual to illness (physiologic).
Age
Osteoporosis makes the older adult more prone to fractures, especially of the hip.
Thinning skin in older adults makes this group more susceptible to skin trauma.
Environment
Air, water, and noise pollution increase the risk of illness.
Asbestos in building structures increases the risk of cancer of the pleura (in lung).
Carbon monoxide (CO) with the burning of fossil fuels in generators, gas stoves, and heaters may lead to sudden illness and death.
Extremes of heat and cold have potential to damage or destroy body cells.
High crime rates and overcrowding also lead to stress, which makes individuals more susceptible to disease.
Within the family, conflicts or other problems have the potential to create stressors that put individual members or the family as a whole at increased risk of illness.
Lifestyle
Other habits that place a person at risk for illness include alcohol and substance abuse.
Overeating or poor nutrition, insufficient rest and sleep, and poor personal hygiene also add to increased risk for illness for the individual.
Prolonged emotional stress, especially with ineffective coping mechanisms, increases the risk of the development of illness and disease.
Smoking increases the risk of many diseases, including oral (mouth) cancer, pharyngeal cancer, laryngeal cancer, lung cancer, renal cancer, esophageal cancer, pancreatic cancer, bladder cancer, uterine and cervical cancer, cardiovascular disease, and osteoporosis. Smoking is the most preventable cause of death in our society.
Sunbathing increases the risk of skin cancer.
physical assessment techniques
Inspection
Visually inspect the patient’s body and observe moods, including all responses and nonverbal behaviors. This inspection, or purposeful observation, is the technique the nurse uses most frequently. It begins with the nurse’s first contact with the patient and continues throughout the gathering of the nursing history. Use inspection to collect data systematically about significant behaviors or physical features. It is important to be accurate and thorough using a systematic approach such as a head-to-toe assessment.
Palpation
With palpation, the nurse uses the hands and sense of touch to gather data. Hands are highly sensitive to texture, temperature, and moisture and thus help determine the quality of an area. Use palpation to detect tenderness, temperature, texture, vibration, pulsations, masses, and other changes in structural integrity. Palpate each body part, usually according to a systematic assessment pattern. Palpation rules out or confirms suspicions raised during interview and inspection. Because touching has the potential to elicit fear, embarrassment, pain, or other strong emotions, explain the nurse’s actions and the reasons for them. In addition, instruct the patient to let the nurse know whether palpation produces sensations of tenderness, pressure, or pain. The three palpation techniques are light, moderate, and deep.
When using palpation, be sure the fingernails are short, and warm the hands before touching the patient. Social conversation during palpation is appropriate at times to distract patients and help them relax. Use the pads of the fingers; place them flat against the patient’s skin with slight pressure and gentle rotation of the area under examination. The thumb and forefinger can be used to palpate muscle mass on arms and legs. Palpate pulses with the pads of the fingers. Someone who is not appropriately trained to perform palpation can cause internal injuries. During palpation, also observe the patient’s facial expressions; if you see a grimace indicating pain, for instance, ask the patient to describe it.
Auscultation
Auscultation is the process of listening to sounds produced by the body. Three systems produce sounds the nurse will auscultate: the cardiovascular system, the respiratory system, and the gastrointestinal system. For auscultation of these systems, the nurse uses a stethoscope, an instrument that amplifies sounds produced by internal organs. The nurse also uses the technique of auscultation to detect the fetal heart sound.
To master the auscultation technique and gain experience at interpreting the sounds the nurse hears, the nurse needs repeated practice on healthy and ill patients. Accurate assessment requires a quiet environment. Television, sounds from nasogastric suction, movement of bed linen, and conversation can interfere with accurate auscultation. Try closing the eyes while listening to reduce visual distractions. Never rush auscultation. Take time to assess each area properly.
Place the diaphragm of the stethoscope gently over the patient’s skin. If the area is hairy, dampening it sometimes decreases the sound of the hair rubbing against the diaphragm.
Percussion
Percussion is the use of the fingertips to tap the body’s surface to produce vibration and sound. The sounds indicate the density of the underlying tissue and thus help the nurse detect the location of body organs and structures. For example, percussion over a hollow organ such as the stomach produces a high-pitched, drumlike sound called tympany. Percussion over a dense organ such as the liver produces a low-pitched, thudlike sound called dullness. Percussion over a muscle produces a soft, high-pitched, flat sound called flatness. To perform percussion, place the palmar surface of one hand against the patient’s body while tapping with the fingers of the other hand. Tap each area two or three times. Properly performed, percussion is not painful for the patient, but if it does cause discomfort, discontinue it and document the results. This assessment technique is the one the nurse uses least frequently.
positions for examination (select all apply question)
Position: Sitting
Areas Assessed: Head and neck, back, posterior thorax and lungs, anterior thorax and lungs, breasts, axillae, heart, vital signs, and upper extremities
Rationale: Sitting upright provides full expansion of lungs and provides better visualization of symmetry of upper body parts.
Limitations: Some physically weakened patients are unable to sit. Use supine position with the head of the bed elevated instead.
Position: Supine (laying on back)
Areas Assessed: Head and neck, anterior thorax and lungs, breasts, axillae, heart, abdomen, extremities, pulses
Rationale: This is the most normally relaxed position. It provides easy access to pulse sites.
Limitations: If a patient becomes short of breath easily, consider raising the head of the bed.
Position: Dorsal recumbent (laying flat on back, knees flexed)(position for pericare)
Areas Assessed: Head and neck, anterior thorax and lungs, breasts, axillae, heart, abdomen
Rationale: Position is used for abdominal assessment because it promotes relaxation of abdominal muscles.
Limitations: Patients with painful disorders are more comfortable with knees flexed.
Position: Lithotomy (lying flat, legs in stirrups)(position for papsmear)
Areas Assessed: Female genitalia and genital tract
Rationale: This position provides maximal exposure of genitalia and facilitates insertion of vaginal speculum.
Limitations: Lithotomy position is embarrassing and uncomfortable, so minimize the time that a patient spends in it. Keep the patient well draped.
Position: Sims ( lying on side, one knee flexed up)
Areas Assessed: Rectum and vagina
Rationale: Flexion of hip and knee improves exposure of the rectal area.
Limitations: Joint deformities may hinder a patient’s ability to bend hip and knee.
Position: Prone (lying flat on stomach)
Areas Assessed: Musculoskeletal system
Rationale: This position is used only to assess extension of hip joint.
Limitations: Patients with respiratory difficulties tolerate this position poorly.
Position: Lateral recumbent (lying on either side, body straight)
Areas Assessed: Heart
Rationale: This position aids in detecting murmurs.
Limitations: Patients with respiratory difficulties tolerate this position poorly
Position: Knee-chest ( head down, butt up)(position with getting rid of gas)
Areas Assessed: Rectum
Rationale: This position provides maximum exposure of rectal area.
Limitations: This position is embarrassing and uncomfortable.
nonreactive pupils
Neurological assessment
Level of consciousness (matching question)
confusion
Inappropriate response to stimuli and decreased attention span and memory; inappropriate reactions to simple commands
lethargy (hypersomnia)
Drowsiness or increased sleep time; is able to be aroused; responds appropriately to; possibly falls asleep again immediately
stage 1 stupor
Arousable with vigorous repeated stimuli. See slowed verbal responses but deep tendon and superficial reflexes are intact
brain death
No responses noted, and reflexes are abnormal or absent
PERRLA
P - pupils
E - equal
R - round
R - reactive
L - light
A - accommodation
normal vital signs and the ranges
Temperature
98.6
Respirations
12 to 20
Blood pressure
120/80
Pulse
60 to 100
Pain
fifth sign
Use a pain rating scale to assess pain intensity systematically and manage pain. The most used numeric scale is 0–10. Ask the patient to rate pain from 0 (no pain) to 10 (worst pain). Ratings of 3–5 are considered mild pain, ratings of 5–7 are considered moderate pain, and ratings greater than 7 are considered severe pain. Some agencies use a scale of 0–5. For children, use happy and sad faces to rate the pain. For clinical assessment, any of these scales is adequate and appropriate. However, always use the same scale with the same patient.
abnormal respirations (select all apply question)
crackles
Produced by fluid in the bronchioles and the alveoli, are short, discrete, interrupted, crackling, or bubbling sounds that are usually heard during inspiration
wheezing
Sounds produced by the movement of air through narrowed passages in the tracheobronchial tree
stridor
High pitched, inspiratory, crowing sound, louder in the neck than over the chest wall
Originates in the larynx or the trachea and indicates upper airway obstruction from edematous, inflamed tissues or a foreign body
pleural friction rubs
Produced by inflammation often pleural sac
Hears a rubbing, grating, or squeaky sound upon auscultation
verbal and nonverbal messages
Verbal - by mouth
Nonverbal - gesturing
components of health history (select all apply question)
Health
Wellness
Illness
matching vital sign changes to causes
decreased blood pressure - dehydrated
increased pulse, temp, resp - infection
bruit
Abnormal “swishing” sounds heard over organs, glands, and arteries
abnormal assessment of spine (select apply apply question)
Lordosis
Swayback
Increased lumbar curvature
Kyphosis
Humpback
Exaggeration of the posterior curvature of the thoracic spine
Scoliosis
Lateral spinal curvature
demonstrate critical thinking in nursing
reasoning
Critical thinking
Cognitive process used for analysis of an issue or problem, is knowledge based, and not dependent on a particular situation
critical thinking relies on not only performing skills but also thinking about the reasoning of why to do it
strategies of critical thinking skills (select all apply question)
data clustering
obtain from the health history, physical examination, and related diagnostic procedures are analyzed in the development of a plan of care
Clustering of related data helps to identify patterns that assist with the identification of the patient problem statement
focus assessment
advisable when the patient is critically ill, disoriented or unable to respond
used to gather information about a specific health problem
performed continually throughout nurse-patient contact
nurse monitors intake and output , skin turgor, and oral mucous membranes for inadequate fluid volume
normal heart sounds
S1 - first normal heart sound and occurs with closure of the atrioventricular valves and thus signals the beginning of systole
S2 - second normal heart sound and occurs with closure of the semilunar valves and signals the end of systole
auscultated most clearly at the base
S3 - sounds heard after S2 and considered an extra heart sound
best heard at the apex
sometimes normal in children bur usually abnormal in adults
dull, soft sound and its sometimes an early sign of heart failure
S4 - heard late in diastole when the atria contracts
auscultated most clearly at the apex and is heard immediately before S1
sound is soft with a low pitch
sometimes normal and sometimes pathologic, heard in patients with coronary artery disease after an MI
best method to assess skin turgor for hydration of skin
normal skin is warm, dry, and smooth with good turgor
turgor = elasticity of the skin caused by the outward pressure of the cells and interstitial fluid
dehydration results in decreased skin turgor and is manifested by lax skin that, when grasped and raised between 2 fingers, slowly returns to its previous position called tenting
marked edema results in increased turgor, manifested by smooth, taut, shiny skin that cannot be grasped and raised
primarily role of LVN/RN
LVN/LPN
provides direct services under supervision of RN or physician
Demonstrate professional behaviors of accountability and professionalism according to the legal and ethical standards for a competent licensed practical/vocational nurse.
• Effectively communicate with patients, significant support person(s), and members of the interdisciplinary health care team incorporating interpersonal and therapeutic communication skills.
• Collect holistic assessment data from multiple sources, communicate the data to appropriate health care providers, and evaluate patient responses to interventions.
• Collaborate with the RN or other members of the health care team to organize and incorporate assessment data to plan/revise patient care and actions based on established nursing diagnoses, nursing protocols, and assessment and evaluation data.
• Demonstrate a caring and empathic approach to the safe, therapeutic, and individualized care of each patient.
• Implement patient care, at the direction of an RN, a licensed physician, or a dentist through performance of nursing interventions or directing aspects of care, as appropriate, to UAP.
RN
practice in a variety of settings inside and outside of the care facility
duties and tasks vary according to educational background and the states nurse practice act
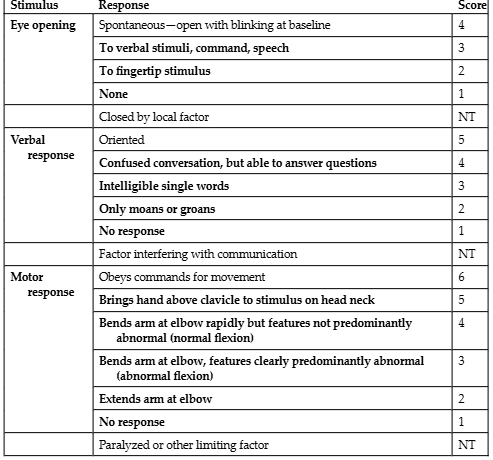
Glasgow coma scale: demonstrating measurement of level of consciousness
assessments for patient
to be done at the start of shift
when symptoms change
history of present illness (OPQRSTUV)
O = Onset-Timing
Onset, duration
P = Precipitating-Provocative-Palliative
What causes it? What makes it worse? What makes it better
Q = Quality-Quantity: describe it: sharp, dull …
How does it feel, look, or sound, and how much of it is there?
How often, when, how long?
R = Region-Radiation
Where is it? Does it spread?
S = Severity scale
Does it interfere with activities? How does it rate on a severity scale of 0–10?
T = Treatments
What helps? For how long?
U = Understanding
What do you think is causing it? How does it affect you?
V = Values
Goals of care; expectations
Foley catheter infection
foul odor
cloudy urine