Ch1 and Ch2: Vesiculobullous & Ulcerative Diseases
Ch1: Vesiculobullous Diseases (11 Lesions)
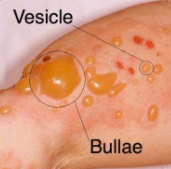
Vesicle: Small fluid-filled sac.
Bullae: Larger fluid-filled sac.
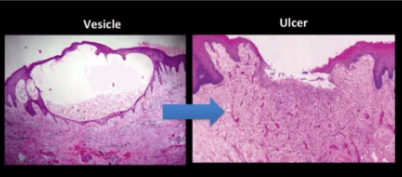
Ulcer: Loss of surface epithelium and exposure of underlying connective tissue.
3 Main Categories
Viral Diseases
Herpes simplex infection
Varicella zoster infection
Hand-foot-mouth disease
Herpangina
Measles
Immune Mediated Diseases
Pemphigus
Pemphigoid
Hereditary
Epidermolysis Bullosa
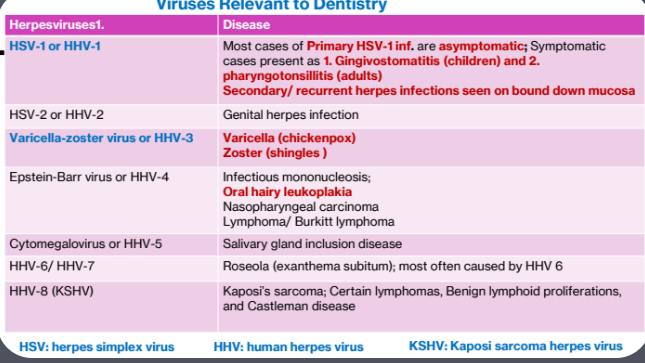
Viral Diseases
Herpesviruses
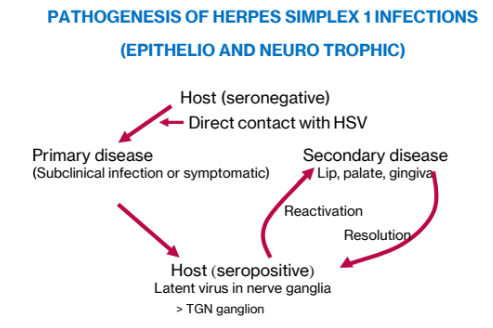
1. Pathogenesis of Herpes Simplex 1 Infections (Epithelio and Neuro Trophic)
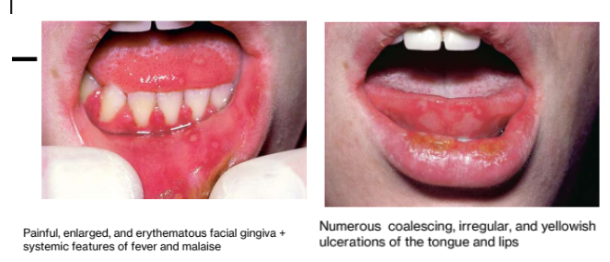
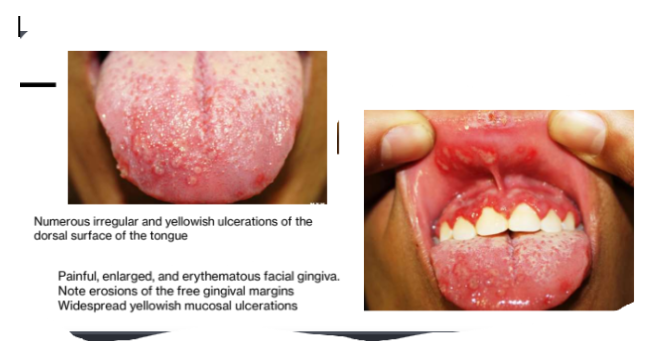
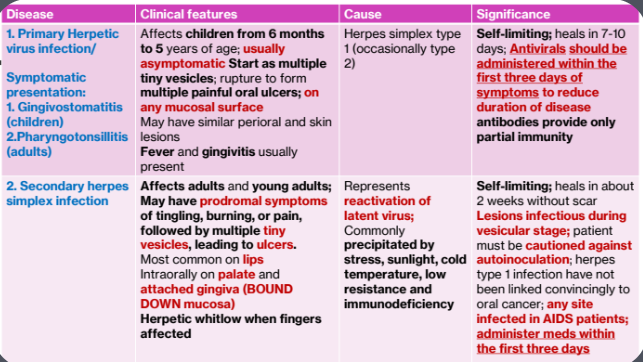
1a.Primary Herpetic Gingivostomatitis
Symptomatic presentation:
Gingivostomatitis (children)
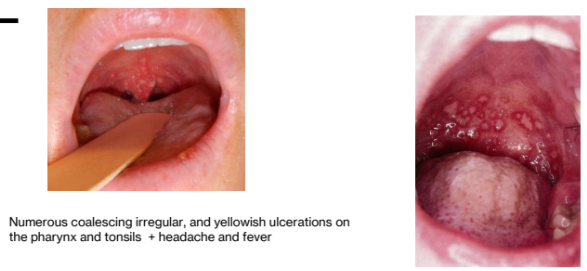
Pharyngotonsillitis (adults)
Clinical Features:
Affects children from 6 months to 5 years of age
usually asymptomatic
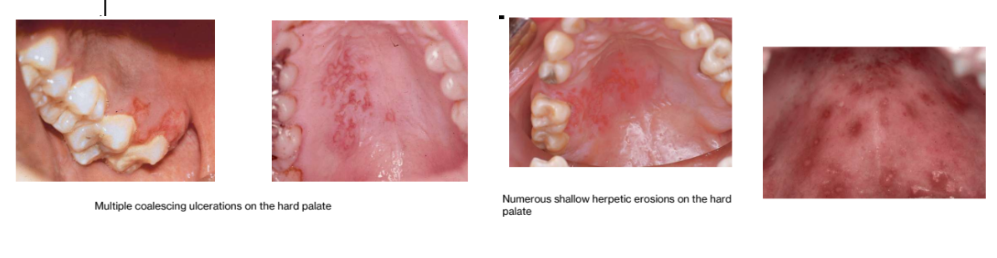
Start as multiple tiny vesicles; rupture to form multiple painful oral ulcers; on any mucosal surface
May have similar perioral and skin lesions
Fever and gingivitis usually present
Cause:
Herpes simplex type 1 (occasionally type 2)
Significance
Self-limiting; heals in 7-10 days
Antivirals should be administered within the first three days of symptoms to reduce duration of disease antibodies provide only partial immunity
Primary herpetic gingivostomatis
Primary Herpetic Pharyngotonsilitis (in adults)

1b. Secondary Herpes Simplex Infection
Clinical Features
Affects adults and young adults
May have prodromal symptoms of tingling, burning, or pain, followed by multiple tiny vesicles, leading to ulcers.
Most common on lips Intraorally on palate and attached gingiva (BOUND
DOWN mucosa)
Herpetic whitlow when fingers affected
Cause
Represents reactivation of latent virus
Commonly precipitated by stress, sunlight, cold temperature, low resistance and immunodeficiency
Significance
Self-limiting
heals in about 2 weeks without scar
Lesions infectious during vesicular stage
patient must be cautioned against autoinoculation
herpes type 1 infection have not been linked convincingly to oral cancer
any site infected in AIDS patients
administer meds within the first three days
Intraoral secondary herpes infection
Seen only on the hard palate and gingiva
Exception to this rule is in AIDS patients, in whom herpes may occur on any mucosal site)
Herpes labialis
most secondary herpetic lesions occur on the vermilion & perioral skin. These patients have lip discomfort but no systemic signs or symptoms.
Are these patients infectious at this stage of the disease?
Yes, the vesicular stage is probably the most infectious stage. Late in the ulcerative stage, the virus has likely retreated to a nerve ganglion

Herpes whitlow
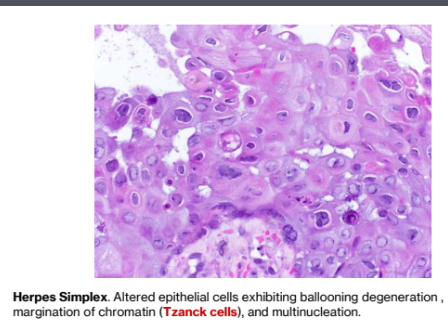
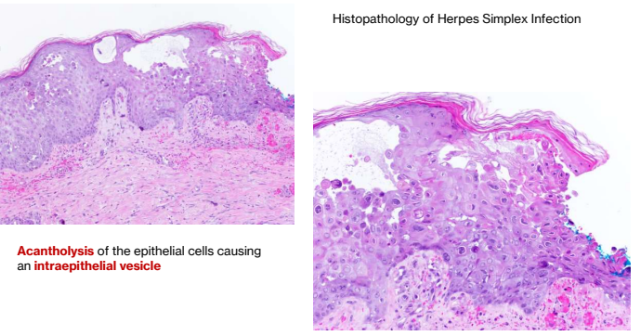
Histopathology of herpes simplex infection
Acantholysis of the epithelial cells causing an intraepithelial vesicle
Altered epithelial cells exhibiting ballooning degeneration ,
margination of chromatin (Tzanck cells), and multinucleation.

HSV-1 Summary
2. Varicella (chicken pox)-Primary infection, Herpes Zoster (Shingles)-Secondary infection, HHV-3 (Varicella Zoster virus)
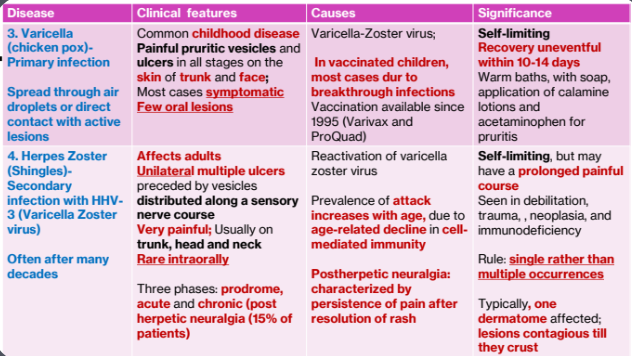
2a.Varicella (Chicken Pox) - Primary Infection (HHV3)
Spread
Spread through air droplets or direct contact with active lesions
Clinical features
Common childhood disease
Painful pruritic vesicles and ulcers in all stages on the skin of trunk and face
Most cases symptomatic
Few oral lesions
Causes
Varicella-Zoster virus
In vaccinated children, most cases dur to breakthrough infections
Vaccination available since 1995 (Varivax and ProQuad)
Significance
Self-limiting
Recovery uneventful within 10-14 days
Warm baths, with soap, application of calamine lotions and acetaminophen for pruritis
Other Facts
Unlike HSV-1, gingival lesions of varicella are painless
In vaccinated children:
few macular papular rashes, few to on vesicles, no fever, and shorter duration of disease
In unvaccinated children starts with malaise, pharyngitis, and rhinitis; followed by an intensely pruritic rash which starts on the skin of trunk and face and spreads to the extremities
Each lesion rapidly progresses through stages of erythema, vesicle, pustule, and hardened crust; lesions continue to erupt for 4 days
Affected individuals are contagious for 2 days before exanthem until
all lesions crust

2b. Herpes Zoster (Shingles) - Secondary Infection with HHV-3 (Varicella Zoster virus)
Often after many decades
Clinical features:
Affects adults
Unilateral multiple ulcers preceded by vesicles distributed along a sensory nerve course
Very painful; Usually on trunk, head and neck
Rare intraorally
Three phases: prodrome, acute and chronic (post herpetic neuralgia (15% of patients)
Cause:
Reactivation of varicella zoster virus
Prevalence of attack increases with age, due to age-related decline in cell-
mediated immunity
Postherpetic neuralgia: characterized by persistence of pain after resolution of rash
Significance:
Self-limiting, but may have a prolonged painful course
Seen in debilitation, trauma, neoplasia, and immunodeficiency
Rule: single rather than multiple occurrences
Typically, one dermatome affected; lesions contagious till they crust
3 phases of Herpes Zoster
1.Prodrome (precedes acute phase rash by 1-4 days)
During initial replication, ganglionitis develops resulting in neuronal necrosis and severe neuralgia
This is responsible for prodromal pain present in more than 90% of cases
As the virus travels down the nerve, the pain intensifies (burning, boring prickly or knife-like)
2.Acute phase
Clusters of vesicles set in an erythematous base
Within 3-4 days vesicles become pustules, and ulcerate, with crusts developing in 7-10 days
3. Chronic phase (post herpetic neuralgia)
Persistent pain after resolution of rash; most resolve within 1 year
Dermal and ocular shingles
Ocular lesions seen in 10%-25% of cases and can cause significant morbidity, including permanent blindness
Hutchison sign
lesions on tip of nose indicating severe ocular infection
Lesions on the tip of the nose (Hutchinson sign) indicate involvement of the nasociliary branch of TGN and an increased risk for severe ocular infection
Ramsay Hunt Syndrome- reactivation of VZV related
Reactivation of the VZV in the geniculate ganglion may cause Ramsay
Hunt Syndrome
RH Syndrome is characterized by:
Cutaneous lesion of the external auditory canal
Involvement of the ipsilateral facial and auditory nerves
Affected individuals may exhibit
Facial Paralysis
Hearing deficit, vertigo and other auditory and vestibular symptoms
Some patients may develop loss of taste in the anterior 1/3 of the
tongue

Shingle treatment
Supportive therapy includes antipruritic (Diphenhydramine) and nonaspirin antipyretics
Skin lesions should be kept dry, clean, and if possible covered to prevent secondary infection
Antibiotics used to treat secondary infections
Vaccinations for Zoster (Shingles/Secondary Infection)
Shingrix; FDA approved
Recommended for adults 50 years and older; 2 doses administrated separated 2-6 months apart
More than 90% effective at preventing shingles and post herpetic neuralgia
Contraindications:
Allergic reactions to any components of vaccination
Currently have shingles
Currently are pregnant
Side effects: sore arm, fever, and stomach pain for 2-3 days; rarely- Guillain-
Barre syndrome
D/D
Recurrent HSV infection
Favor shingles diagnosis when:
Longer duration
Greater intensity or prodromal symptoms
Unilateral distribution with abrupt ending at midline
Post-herpetic neuralgia

HH3 Summary
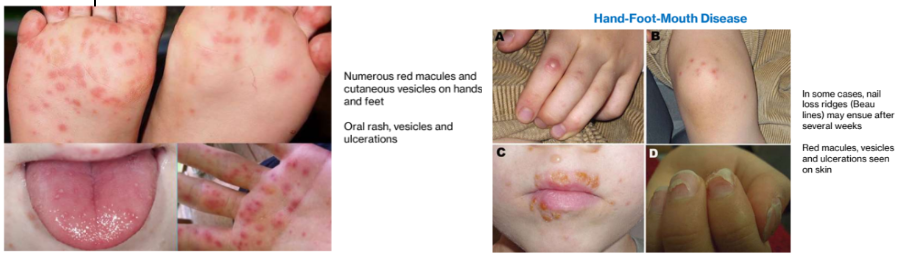
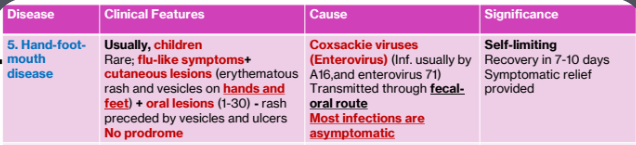
3. Hand-foot-mouth disease
Clinical Features
Usually, children
Rare; flu-like symptoms+ cutaneous lesions (erythematous rash and vesicles on hands and feet) + oral lesions (1-30) - rash preceded by vesicles and ulcers
No prodrome
Cause:
Coxsackie viruses (Enterovirus)
(Inf. usually by A16,and enterovirus 71)
Transmitted through fecal-oral route
Most infections are asymptomatic
Significance
Self-limiting
Recovery in 7-10 days
Symptomatic relief provided
Therapy
Therapy directed towards symptomatic relief: nonaspirin antipyretic and topical anesthetic ( dyclonine hydrochloride)
Summary
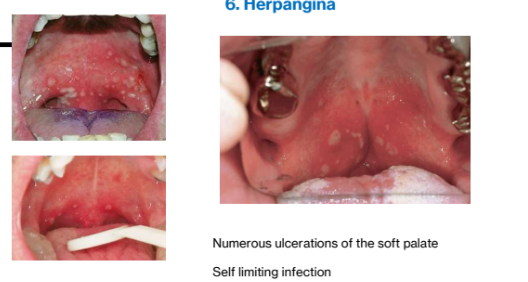
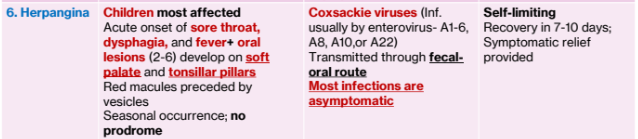
4. Herpangina
Clinical Features
Children most affected
Acute onset of sore throat, dysphagia, and fever+ oral lesions (2-6) develop on soft palate and tonsillar pillars
Red macules preceded by vesicles
Seasonal occurrence; no prodrome
Cause:
Coxsackie viruses (Inf. usually by enterovirus- A1-6, A8, A10,or A22)
Transmitted through fecal-oral route
Most infections are asymptomatic
Significance
Self-limiting
Recovery in 7-10 days
Symptomatic relief provided
Therapy
directed towards symptomatic relief: nonaspirin antipyretic and topical anesthetic ( dyclonine hydrochloride)
Summary
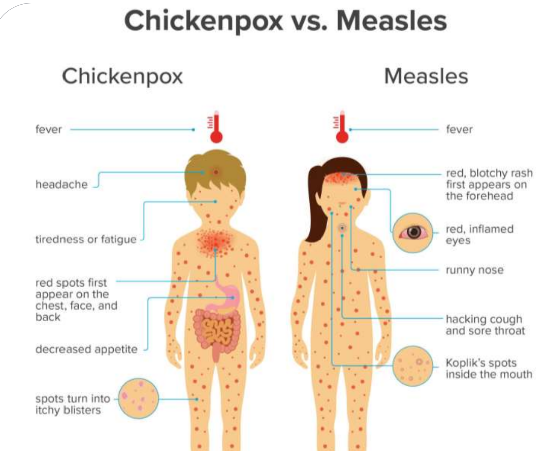
5. Measles (Rubeola)
Clinical Features
Usually children
Oral Kolpik spots precede maculopapular skin rash
Fever, malaise, plus other symptoms of viral infection
Cause:
Measles virus (highly contagious paramyxovirus)
Respiratory droplets spread
Significance
Self-limiting
Recovery in about 2 weeks
Symptomatic relief provided
Universal vaccination 1963
9-day measles 3 stages
First three days 3Cs
Cough, coryza, and conjunctivitis + Koplik spots (oral lesions representing foci of epithelial necrosis; appear as blue-white macules) + fever
Second stage:
fever + Koplik spots fade +erythematous rash on skin
Third stage:
no fever + rash fades
Koplik spots
represent foci of epithelial necrosis and appear as numerous small, blue-white macules surrounded by erythema; Typically involve the buccal mucosa

Summary
Chickenpox vs Measles

Immunobullous Diseases
1. Pemphigus vulgaris
Systemic condition
Clinical Features
> Middle aged patients (50 yrs.)
Multiple painful ulcers preceded by bullae
Positive Nikolsky' s sign
Progressive disease
Remission or control with therapy
Ocular lesions infrequent and do not cause scarring
Cause
Autoimmune
Antibodies, produced due to unknown reasons
directed against desmosome-associated
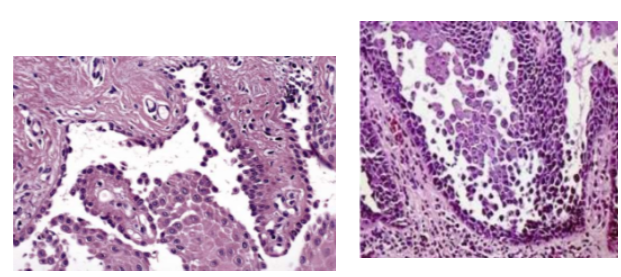
protein, desmoglein 3 (H/P: intraepithelial separation)
Significance
Without treatment, may be fatal
Oral lesions precede skin lesions in half the cases
Prognosis improved if treated early
Nikolsky Sign
bulla induced on normal appearing mucosa or skin because of
slight pressure or rubbing
It is an indication of an autoimmune disease and represents the loss of cohesion between epithelial cells or the loss or cohesion of the epithelium to the basement membrane

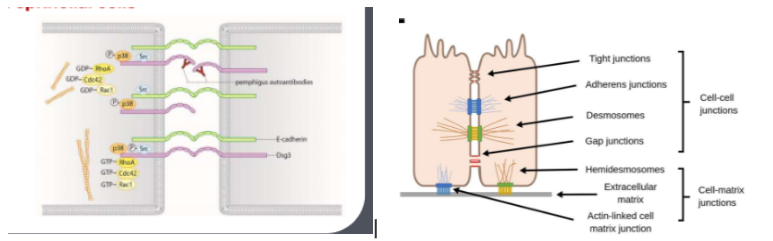
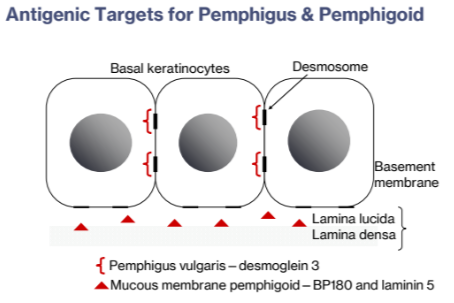
Cellular Level happenings
Autoimmune reaction to intercellular keratinocyte protein (desmoglein 3)
results in intraepithelial blisters caused by autoantibodies attacking the junction between epithelial cells (intraepithelial vesicle)
desmosome proteins (desmoglein) are attacked by the autoantibodies
Oral lesions
Oral lesions are often the first sign of the disease
Oral lesions are most difficult to resolve with therapy
Oral lesions are "first to show and last to go"
Rare to see bullae intraorally due to thin epithelial roof ; bullae are more
commonly seen in pemphigoid due to the subepithelial splitting of epithelium
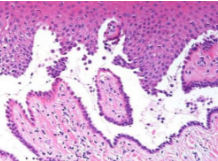
Histopathology
Rounded, acantholytic epithelial cells sitting within the intraepithelial cleft
The basal cells are attached to the basement membrane "row of tombstones"
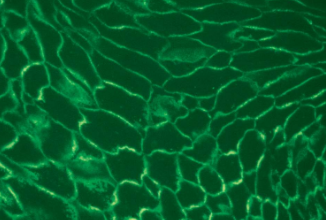
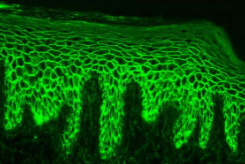
Diagnosis should be confirmed by direct immunofluorescence studies (antibodies against desmosomes)
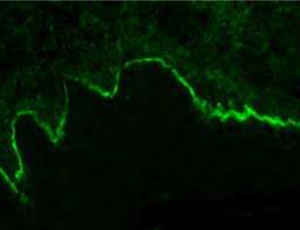
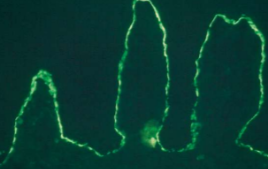
Direct immunofluorescence pattern:
Autoantibodies (usually IgG or IgM) and complement component (usually C3) can be demonstrated in the intercellular spaces between the epithelial cells in almost all patients with this disease( "chicken wire' pattern)
Indirect immunofluorescences
typically positive in 80%-90% of cases, demonstrating the presence of circulating antibodies in the patient's serum (systemic disease needing systemic corticosteroids)
Notes:
Diagnosis of PV should be made as early in its course as is possible because control is easier to achieve
PV is a systemic disease, because circulating antibodies in the patent's serum is seen in 80% - 90% of cases
Perilesional tissue should be obtained for both light microscope and direct immunofluorescent studies to maximize the probability of a diagnostic sample
If ulcerate mucosa is submitted for testing, the results are inconclusive as the epithelium is lost
Treatment
Requires a systemic approach
Currently, the use of Rituximab, a monoclonal antibody that targets B-lymphocytes, is often mentioned as a first-line of approach
Rituximab targets cells responsible for producing the autoantibodies that cause pemphigus
Rituximab is used in combination with a lower dose of systemic corticosteroids, resulting in a more rapid clearing of the lesions
Ideally, physician with expertise in immunosuppressive therapy should manage the patient
Summary:
2. Mucous membrane pemphigoid
Clinical Features
> Middle aged or elderly women
Multiple painful ulcers preceded by vesicles and bullae
Lesions may heal with scars
Positive Nikolsky' s sign
May affect mucous membrane of oral cavity, eyes, and genitalia
Cause
Autoimmune
Antibodies directed against basement membrane antigens, laminin 5, BP 180 and others (H/P: subepithelial separation)
Significance
Protracted course
may cause significant morbidity
If severe, ocular scarring may lead to blindness
Death uncommon
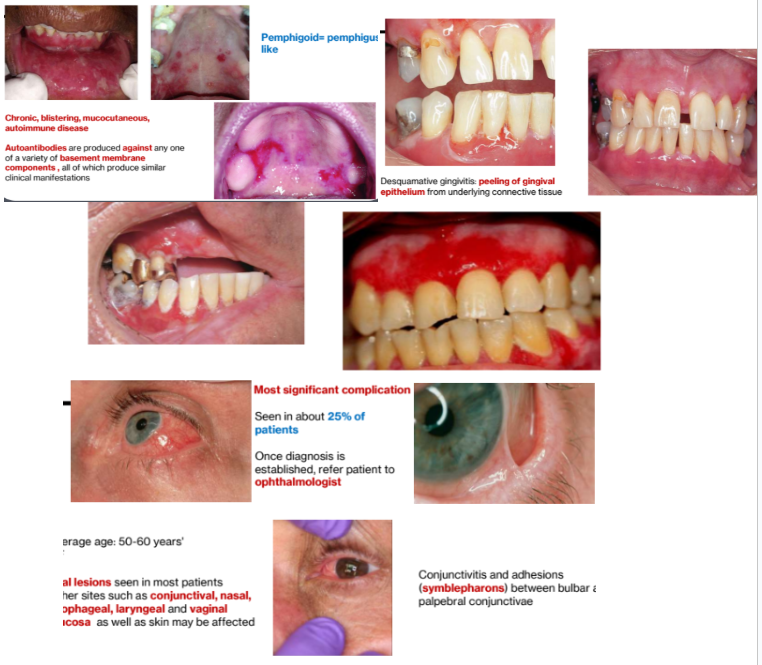
Pemphigoid= pemphigus- like
Autoantibodies are produced against any one of a variety of basement membrane
components , all of which produce similar clinical manifestations
Desquamative gingivitis
peeling of gingival epithelium from underlying connective tissue
Pattern of gingival involvement "desquamative gingivitis" is seen in:
Pemphigus vulgaris
Pemphigoid
Erosive Lichen Planus
Ocular Lesions
Most significant complication
Seen in about 25% of patients
Once diagnosis is established, refer patient to ophthalmologist
Conjunctivitis and adhesions (symblepharons) between bulbar and palpebral conjunctivae
Average age: 50-60 years',> F
Oral lesions seen in most patients
Other sites such as conjunctival, nasal, esophageal, laryngeal and vaginal mucosa as well as skin may be affected
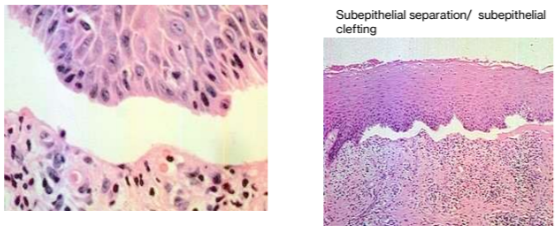
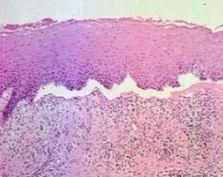
Histopathology:
Mucous membrane pemphigoid showing characteristic subepithelial separation (antibodies directed against basement membrane proteins)
Direct immunofluorescence studies
Direct immunofluorescence studies + in 90% of patients
Indirect immunofluorescence studies + in 5%-25% of patients
Deposition of immunoreactants at the basement membrane zone of the
epithelium
Immunoreactants: Primarily IgG and C3
Biopsy: Pemphigus Vulgaris, Pemphigoid or Lichen Planus (Formalin Solution)
Biopsy specimen in 10% FORMALIN solution
Lesional tissue is an ulcer (epithelium is lost) and is nondiagnostic
The biopsy specimen must be taken from perilesional mucosa (normal looking mucosa, close to the ulcer)
Biopsy shows splits and acantholysis (disintegration of prickle cell layer) above the basal cell layer
Direct Immunofluorescence Pemphigus Vulgaris, Pemphigus, or Lichen Planus (Michel's solution)
Direct Immunofluorescence specimen in MICHEL'S
solution
Autoantibodies are seen to bind around the edges of prickle cells at site of desmosomes
Perilesional biopsy
Indirect immunofluorescence shows circulating auto antibodies in serum:
Pemphigus: positive in 80-90% of cases (SYSTEMIC DISEASE)
Pemphigoid: positive in 5- 25% of cases (LOCAL DISEASE)
Pemphigus Biopsy Results
Suprabasilar acantholysis near the tips of two adjacent rete pegs is recognized
Deposition of IgG or IgM and C3 found between the epithelial cells
PEMPHIGOID Biopsy Results
Subepithelial separation
Deposition of IgG and C3 at the basement membrane zone
Treatment of Mucous Membrane Pemphigoid
If only oral lesions are present, sometimes it can be controlled with topical corticosteroids, applied several times/day
Once controlled, the application can be discontinued
Mild-to-moderate involvement can be treated with Dapsone
Another alternative therapy for mild-to-moderate disease is tetracycline or minocycline and niacinamide (systemic daily doses of 0.5-2 g of each drug)
Patients with severe disease, require corticosteroids plus other immunosuppressants/immune modulating agents (Rituximab, cyclophosphamide, mycophenolate mofetil)
Summary

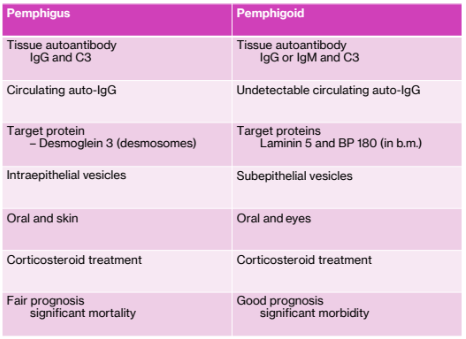
Pemphigus vs Pemphigoid
3. Bullous pemphigoid
Most common
Clinical Features
> elderly (75-80yrs.)
Skin disease (trunk and extremities); with infrequent oral lesions (10%-20%)
ulcers preceded by bullae; no scarring
Cause
Basement membrane autoantibodies detected in tissue and serum;
subepithelial separation
Significance
Clinical course characterized periods of remission, followed by relapse
Primarily skin lesions
subepithelial clefting
Direct immunofluorescence:
Positive basement membrane zone
Indirect immunofluorescence
positive

Summary

Hereditary Disease
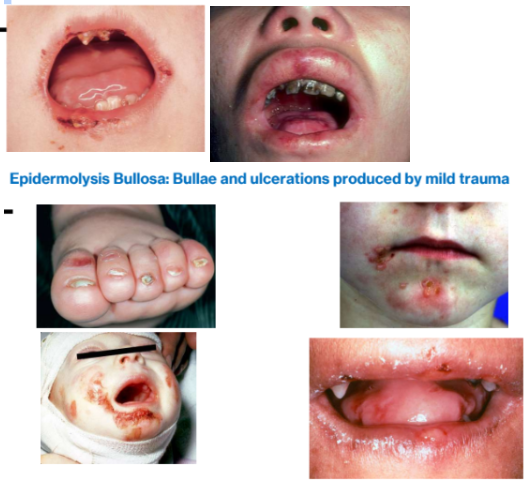
1. Epidermolysis bullosa
30 different forms
Clinical Features
Inheritance pattern determines age of onset during childhood and severity
Multiple ulcers preceded by bullae
Positive Nikolsky sign
May heal with scars
Primarily a skin disease but oral lesions often present
Cause
Hereditary (AD or AR)
Acquired adult form also exists
Defects in keratin genes, hemidesmosomes, or type VII collagen
Significance
Severe debilitating disease that may be fatal in recessive form
Simple operative procedures may elicit bullae
Acquired form less debilitating
Initially bullae form, they ulcerate and heal with scarring
Scarring often leads to microstomia
Heterogenous group of inherited blistering mucocutaneous disorders
Each has a specific defect in the attachment mechanism of the epithelial cells, either to each other or to the underlying connective tissue
Treatment:
Management depends on type of disease
Dental manipulation should be minimum
Topical fluoride solutions and occlusal sealants recommended to prevent dental caries
No cure for the disease
CH2: Ulcerative Diseases (19 Lesions)
Ulcerative Lesions
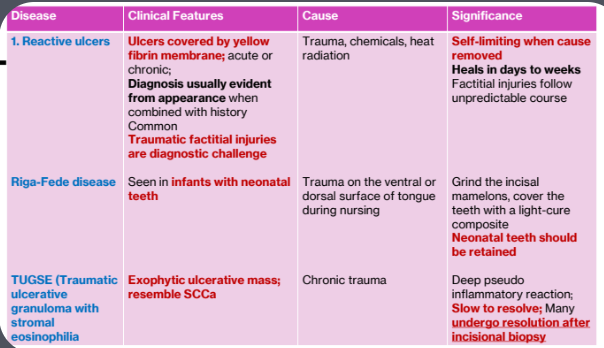
1. Reactive Ulcers
Traumatic ulcers
Traumatic granuloma (TUGSE)
Riga-Fede disease
2. Infectious Diseases causing Ulcers
Bacterial (Syphilis, gonorrhea tuberculosis, leprosy, actinomycosis, and NOMA)
Fungal (Deep fungal infections: histoplasmosis; Opportunistic fungal infections: mucormycosis)
3. Immune Diseases causing Ulcers
Aphthous ulcers
Bechet syndrome
Cyclin neutropenia
Erythema multiforme
Stomatitis medicamentosa
Polyangiitis with granulomatosis (Wegner disease)
4. Neoplasms causing ulcers
Oral squamous cell carcinoma
1. Reactive Ulcers
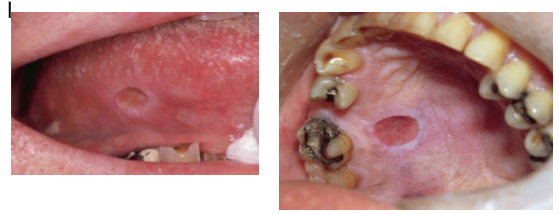
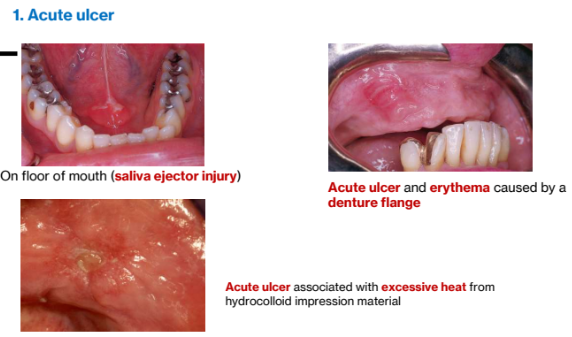
1a. Reactive Ulcers
Clinical Features:
Ulcers covered by yellow fibrin membrane; acute or chronic;
Diagnosis usually evident from appearance when combined with history
Common
Traumatic factitial injuries are diagnostic challenge
Cause
Trauma, chemicals, heat radiation
Significance
Self-limiting when cause removed
Heals in days to weeks
Factitial injuries follow unpredictable course
Acute ulcer
Chronic Ulcers
Well-circumscribed ulceration with a faintly hyperkeratotic collar
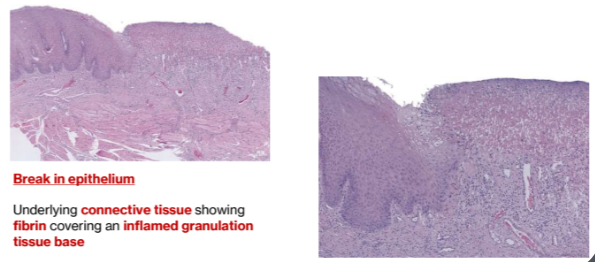
Ulcer
Break in epithelium
Underlying connective tissue showing fibrin covering an inflamed granulation tissue base
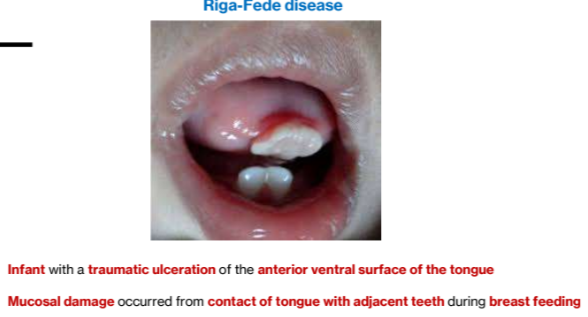
1b. Riga-Fede disease
Clinical Features
Seen in infants with neonatal teeth
Cause
Trauma on the ventral or dorsal surface of tongue during nursing
Significance
Grind the incisal mamelons, cover the teeth with a light-cure composite
Neonatal teeth should be retained
1c. TUGSE (Traumatic ulcerative granuloma with stromal eosinophilia)
Clinical Features
Exophytic ulcerative mass; resemble SCCa
Cause
Chronic trauma
Significance
Deep pseudo inflammatory reaction
Slow to resolve; Many undergo resolution after incisional biopsy
Summary
2. Infectious Diseases Causing Ulcers
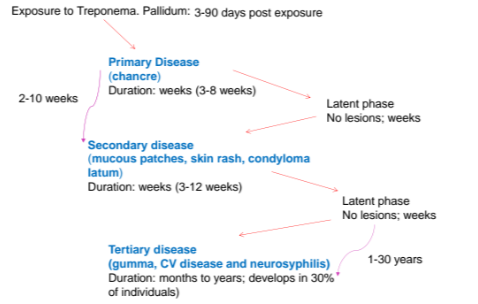
2a. Syphilis (Lues) Bacterial infection
4 Stages
Clinical features
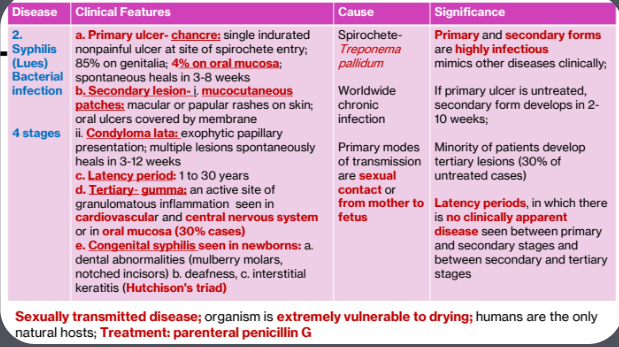
1.Primary ulcer
chancre: single indurated nonpainful ulcer at site of spirochete entry
85% on genitalia; 4% on oral mucosa
spontaneous heals in 3-8 weeks
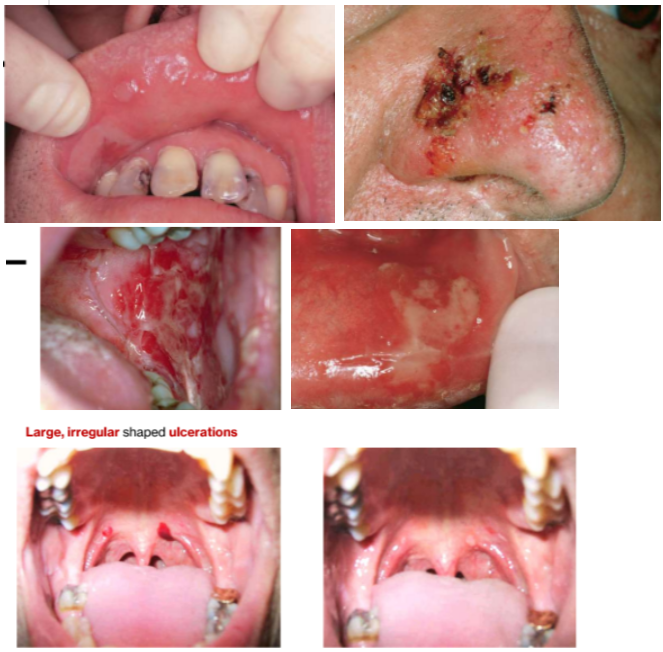
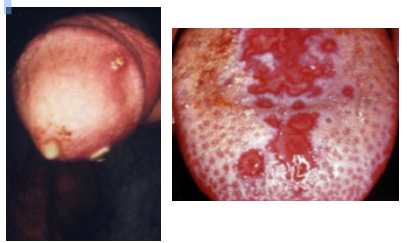
2. Secondary lesion
mucocutaneous patches: macular or papular rashes on skin; oral ulcers covered by membrane
Condyloma lata: exophytic papillary presentation; multiple lesions spontaneously heals in 3-12 weeks
3. Latency period: 1 to 30 years
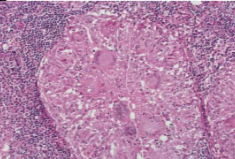
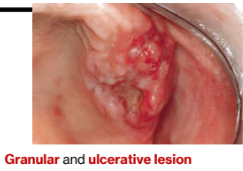
4. Tertiary- gumma
an active site of granulomatous inflammation seen in
cardiovascular and central nervous system or in oral mucosa (30% cases)
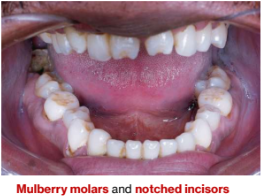
5.Congenital syphilis seen in newborns:
a. dental abnormalities (mulberry molars,
notched incisors)
b. deafness,
c. interstitial keratitis
(Hutchison's triad)
Cause
Spirochete-Treponema pallidum
Worldwide chronic infection
Primary modes of transmission are sexual contact or from mother to fetus
Significance
Primary and secondary forms are highly infectious mimics other diseases clinically
If primary ulcer is untreated, secondary form develops in 2- 10 weeks;
Minority of patients develop tertiary lesions (30% of untreated cases)
Latency periods, in which there is no clinically apparent disease seen between primary and secondary stages and between secondary and tertiary stages
Sexually transmitted disease; organism is extremely vulnerable to drying; humans are the only natural hosts; Treatment: parenteral penicillin G
Syphilis Pathogenesis
Primary oral syphilis→ Chancre
4% cases in oral cavity, > lips
Usually solitary
Painless, cleaned based ulcer
Bilateral regional lymphadenopathy; the organism spreads systemically through lymphatic channels

Primary genital syphilis→ Chancre
85% cases on genitalia
Becomes clinically evident 3-90 days after initial exposure
Resolve within a few days
Secondary syphilis: mucocutaneous patch or condyloma LATA
Multiple lesions
Systemic infection so systemic symptoms arise
Painless lymphadenopathy, sore throat, malaise, headache, weight loss, fever, & musculoskeletal pain

Tertiary syphilis: gumma
30% cases
Gumma causing a palatal fistula
Period of latency may last 1-30 years
Gumma may be an indurated and ulcerated lesion or may produce destruction (Granulomatous inflammation)
Congenital syphilis
Hutchinson triad:
altered formation of anterior and posterior teeth (mulberry molars and notched incisors)
Ocular interstitial keratosis
Eighth nerve deafness
Summary:

2b. Gonorrhea
Bacterial infection
Clinical Features
Typically, genetical lesions with rare oral manifestations, painful erythema or ulcers, or both
Cause:
Neisseria gonorrhoeae (STD)
Significance:
Infectious; STD; may be confused with many oral ulcerative diseases
Incubation period 2-5 days
Affected areas shows purulent discharge
Rare in oral cavity
Area of infection appear as erythematous, pustular, erosive, or ulcerated
Only one class of antibiotics, cephalosporins, is considered to be sufficiently effective
Summary

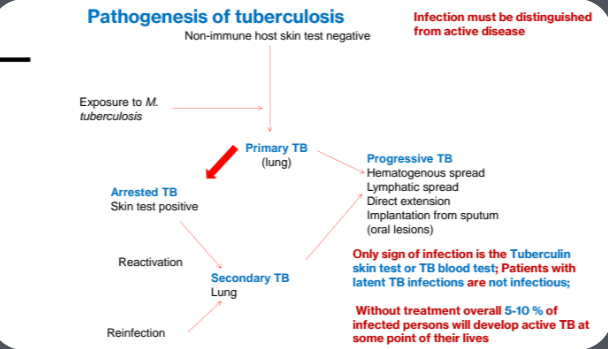
2c. Tuberculosis
Bacterial infection
Clinical Features
Indurated, chronic ulcer that may be painful- on any mucosal surface
Cause:
Mycobacterium tuberculosis (transmitted through respiratory droplets)
Significance
Active TB is transmissible;
Lesions are infectious
oral lesions almost always a result of lung lesions
differential diagnosis includes oral cancers
Chronic infectious disease
Primary TB is asymptomatic; occasionally fever and pleural effusion
Secondary TB occurs at apex of lungs, but may spread to different sites by expectorated infected material or through lymphatic and vascular channels
Patient has low grade fever, anorexia, weight loss, and night sweats
Oral lesions of TB are uncommon; presents as chronic ulcerations or swellings
Cell-mediated hypersensitivity reaction (IV)
Granulomas, often with central caseous necrosis
Granuloma is a circumscribed collection of epithelioid histiocytes, and multinucleated giant cells, surrounded by lymphocytes
Therapy
Multiagent therapy is treatment of choice because it can mutate and become resistant to a single medication
Pathogenesis
D/D of non healing ulcers
Chronic traumatic ulcer
Oral manifestations of deep fungal or bacterial infections
TB
Squamous cell carcinoma
Summary:

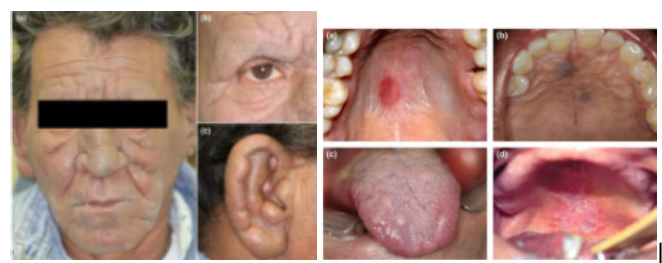
2d. Leprosy (Hansen disease)
Clinical Features
Chronic infectious disease, with rare oral ulcers and nodules
Cause:
Mycobacterium Leprae (transmitted through prolonged direct contact)
Significance:
Low -infectivity; rare in the US but relatively common in Southeast Asia, India, and South America
Facial leprosy
diffuse thickening of the facial skin, and deepening of natural facial lines known as ‘leonine facies’
multiple nodules on ears and loss of eyebrow hair and eyelashes
Oral leprosy
well-defined red macule
purple papules on hard palate
multiple papules and nodules on dorsal tongue
ulcer on hard and soft palate
tuberculoid leprosy
develops in patients with high immune reaction; skin lesions seen; oral lesions rare; well formed granulomas
Lepromatous leprosy
develops in patients with reduced cell mediated immune response; leonine faces, nerve involvement leads to loss of sweating; no well-formed granulomas
Multidrug therapy
Summary

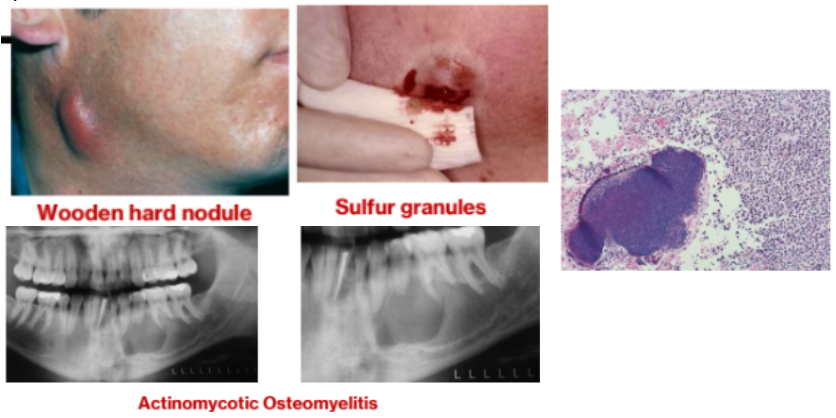
2e. Actinomycosis
Bacterial infection
Clinical Features
Typically, seen in mandible, with draining skin sinus; wood-hard nodule with sulfur granules
Cause
Actinomyces Israelii (filamentous gram + anaerobic bacteria)
Significance
Component of oral cavity; Infection follows entry through a surgical site, periodontal disease, or open root canal
Actinomycetes are normal saprophytic components of oral flora
Histopathology
Actinomycosis colony (sulfur granule) surrounded by pus
The bacterial organisms attracts neutrophils- pus is formed
Treatment
Treated by prolonged high dose of antibiotics in association with abscess drainage and excision of sinus tract
Typically, 5–6-week course of penicillin
Summary

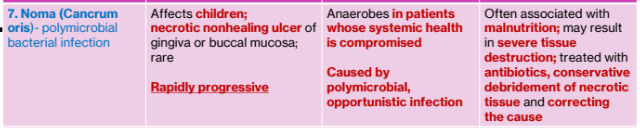
2f. Noma (Cancrum oris)
Polymicrobial bacterial infection
Clinical Features
Affects children
necrotic nonhealing ulcer of gingiva or buccal mucosa
rare
rapidly progressive
Cause:
Anaerobes in patients whose systemic health is compromised
Caused by polymicrobial, opportunistic infection
Significance:
Often associated with malnutrition
may result in severe tissue destruction
treated with antibiotics, conservative debridement of necrotic tissue and correcting the cause
Rapidly progressive, polymicrobial, opportunistic infection
Caused by components of the normal flora that become pathogenic during periods of compromised immune status

Summary
2g. Deep fungal infections (Histoplasmosis)
Clinical Features
Indurated, nonhealing, frequently painful, chronic oral ulcer, usually following implantation of organisms from lungs
Cause
Histoplasma capsulatum, coccidiosis immitis, others
Significance
Oral lesions because of systemic lesion; some types are endemic;
antifungal treatment
Most common systemic fungal infection
Seen in humid areas with soil enriched by bird or bat excrement
Most cases asymptomatic or cause mild symptoms
Types
Acute: self limiting pulmonary infection; fever, headaches, myalgia, nonproductive cough and anorexia
Chronic: primarily affects lungs
Disseminated: spread of infection to extrapulmonary sites; older debilitated individuals; oral lesions seen (painful chronic ulcers)
Summary

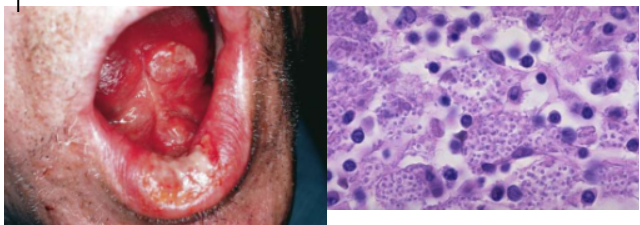
2h. Opportunistic fungal infections (Mucormycosis)
Clinical Features
Occurs in compromised host
necrotic nonhealing ulcers
seen in insulin-dependent diabetics who have uncontrolled diabetes
Rhinocerebral form most relevant to dentists
Cause:
Mucormycosis (zygomycosis, phycomycosis), Rhizopus, others
Significance
Frequently fatal
treated with high dose of amphotericin B, debridement, and control of diabetes or other underlying disease
Rhinocerebral form
most relevant to dentistry: nasal obstruction, bloody nasal discharge, facial pain or headaches, facial swelling, and visual disturbances and proptosis; if untreated - massive tissue destruction
Radiographic opacification of sinuses along with patchy defacement of bony walls of the sinus
Non septate fungal hyphae are characteristic
Seen in insulin-dependent diabetics who have uncontrolled diabetes
Summary

3.Immune Diseases causing Ulcers
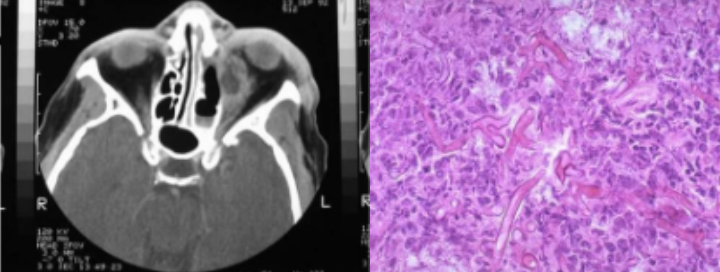
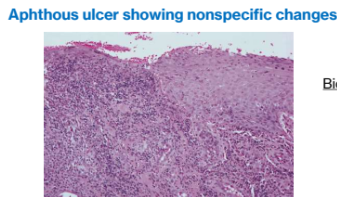
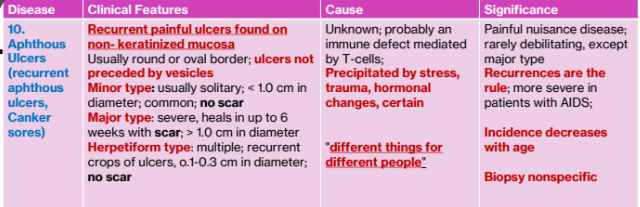
3a.Aphthous Ulcers (recurrent aphthous ulcers, Canker sores)
Clinical features
Recurrent painful ulcers found on non- keratinized mucosa
Usually round or oval border; ulcers not preceded by vesicles
Minor type: usually solitary; < 1.0 cm in diameter; common; no scar
Major type: severe, heals in up to 6 weeks with scar; > 1.0 cm in diameter
Herpetiform type: multiple; recurrent crops of ulcers, o.1-0.3 cm in diameter; no scar
Cause:
Unknown; probably an immune defect mediated by T-cells
Precipitated by stress, trauma, hormonal changes, certain
"different things for different people"
Significance:
Painful nuisance disease; rarely debilitating, except major type
Recurrences are the rule
more severe in patients with AIDS
Incidence decreases with age
Minor aphthous ulcers
Very painful; pain dipropionate to size
Seen in anterior regions of mouth
May be associated with prodromal symptoms of burning, itching or stinging
Major aphthous ulcer
Larger than minor aphthae
Last for longer duration per episode
Take 2-6 weeks to heal
May cause scarring

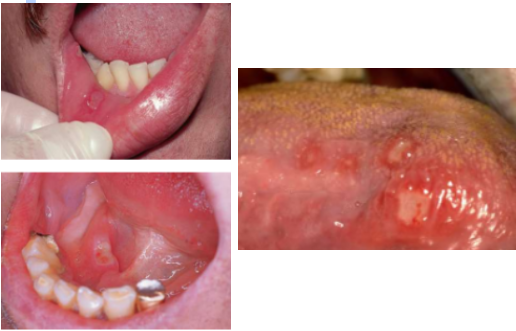
Herpetiform aphthous ulcers
Up to 100 lesions
1-3 mm
Bear resemblance to primary HSV infection
Histopathology
Biopsy not diagnostic
Mucosal barrier appears to be important in the prevention of aphthous stomatitis
Factors that reduce the mucosal barrier increase frequency of occurrences (trauma, nutritional deficiencies, and smoking cessation)
Treatment: medical history thoroughly investigates; mild cases: most patents receive no treatment; severe cases: potent corticosteroids
Summary
3b. Behcet syndrome (GOES)
Clinical Features:
Minor oral aphthae
eye lesions (uveitis, conjunctivitis)
genital lesions (ulcers)
skin
arthritis occasionally seen
Cause:
Probably an immune defect
possible autoimmune heredity and presence of HLA-B51 may be factors
Significance
Biopsy shows vasculitis and lab studies give nonspecific results
complications may be significant
GOES: genital, oral, eyes, and skin lesions or ulcerations

Summary

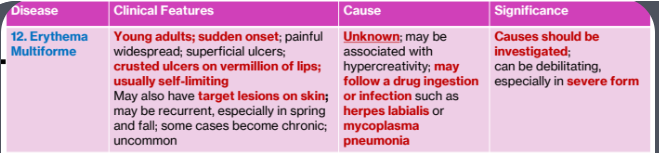
3c. Erythema Multiforme
Clinical Features
Young adults; sudden onset
painful widespread; superficial ulcers; crusted ulcers on vermillion of lips
usually self-limiting
May also have target lesions on skin; may be recurrent, especially in spring and fall; some cases become chronic; uncommon
Cause
Unknown
may be associated with hypercreativity
may follow a drug ingestion or infection such as herpes labialis or mycoplasma pneumonia
Significance
Causes should be investigated
can be debilitating, especially in severe form
Cutaneous target lesions
Blistering, ulcerative, mucocutaneous condition of uncertain pathogenesis;
probably immune mediated; poorly understood
Hemorrhagic crusting of the lips
Precipitating cause:
Herpes simplex infection or mycoplasma pneumoniae (young adults)
Exposure to a drug (less common factor; seen in elderly and middle aged)
These agents precipitate immune derangement
Treatment
Identify precipitating factor if possible
Self limiting disease (lasts 2-6 weeks)
IV rehydration if necessary
Not life threating unless severe

Summary
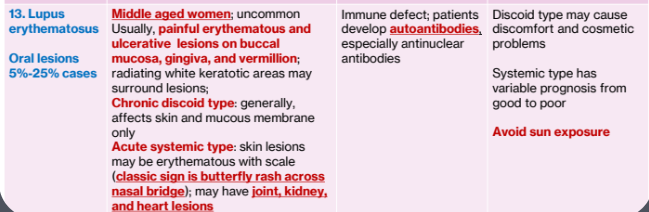
3d. Lupus erythematosus
Oral lesions 5%-25% cases
Clinical Features
Middle aged women; uncommon
Usually, painful erythematous and ulcerative lesions on buccal mucosa, gingiva, and vermillion
radiating white keratotic areas may surround lesions;
Chronic discoid type: generally, affects skin and mucous membrane only
Acute systemic type: skin lesions may be erythematous with scale (classic sign is butterfly rash across nasal bridge); may have joint, kidney,
and heart lesions
Cause
Immune defect; patients develop autoantibodies, especially antinuclear antibodies
Significance
Discoid type may cause discomfort and cosmetic problems
Systemic type has variable prognosis from good to poor
Avoid sun exposure
Most common of the connective tissue disease in the US
Results from abnormal function of T lymphocytes and increased activity of B lymphocytes
Mild disease managed with NSAIDs
Severe disease managed with corticosteroids
Oral lesions seen on palate, BM, and gingiva
Very nonspecific; may be lichenoid
Butterfly- rash of SLE

Summary
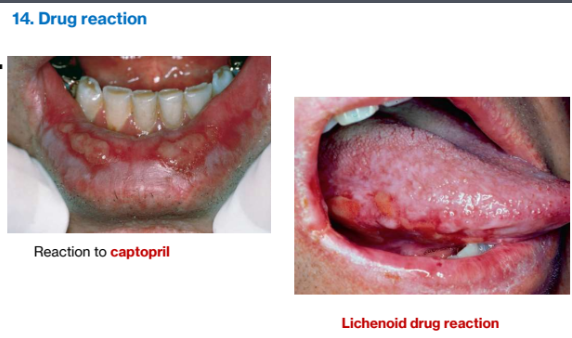
3e. Drug reactions
Clinical features
May affect skin or mucosa
Erythema, white lesions, vesicles, ulcers may be seen; history of recent drug ingestion is important
Cause
Potentially any drug via stimulation of immune system
Significance
Reactions, such as anaphylaxis or angioedema,
may require emergency care; highly variable clinical picture can make diagnosis difficult
Summary

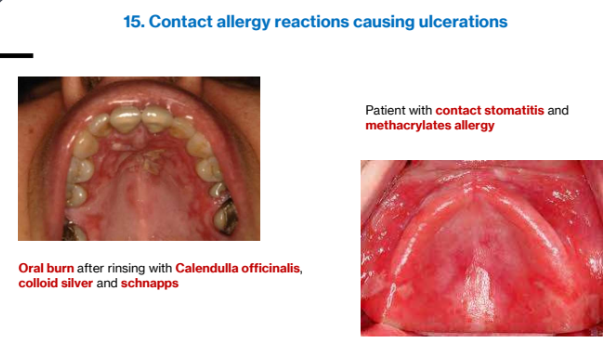
3f. Contact Allergy
Clinical features
Lesions caused by direct contact with foreign antigens; erythema, vesicles, ulcers may be seen
Cause
Potentially any foreign antigen that contacts skin or mucosa; cinnamon frequently sited
Significance
Patch testing may be helpful for diagnosis; history is important
Summary

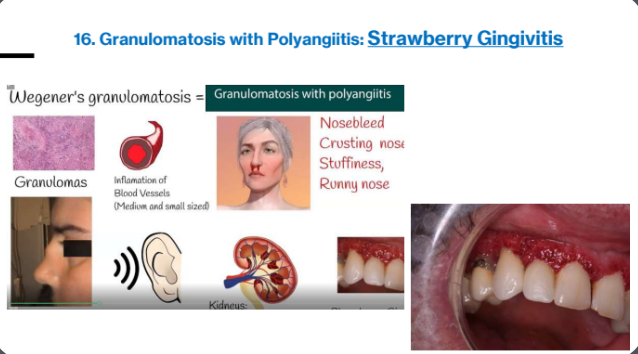
3g. Granulomatosis with polyangiitis (Wegner granulomatosis)
Clinical Features
Inflammatory lesions (necrotizing vasculitis) of lung, kidney, and upper airway
may affect gingiva (strawberry gingivitis) when intraoral; rare
Cause
Unknown; possible immune defect or infection
Significance
May become life threatening because of tissue destruction in any of the three involved sites
Summary

3h. Cyclic neutropenia
Clinical Features
Oral ulcers with periodicity (every 3-6 weeks); infection
adenopathy
3-5 days duration
periodontal disease
Cause
Mutation in neutrophil elastase gene ELA2; AD or new mutation
Significance
Rare blood dyscrasia
Rare blood disorder that causes episodes of low levels of neutrophils
Neutrophils are vital for fighting infections
Neutrophil levels drop for about three to five days, return to normal and then drop again around every three weeks.
Hereditary: mutation in neutrophil elastase gene
Acquired: drugs and toxins

Summary

4.Neoplasms Causing Ulcers
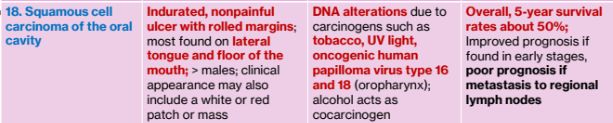
4a. Squamous cell carcinoma of the oral cavity
Clinical Features
Indurated, nonpainful ulcer with rolled margins
most found on lateral tongue and floor of the mouth
> males
clinical appearance may also include a white or red patch or mass
Causes
DNA alterations due to carcinogens such as tobacco, UV light, oncogenic human papilloma virus type 16 and 18 (oropharynx)
alcohol acts as cocarcinogen
Significance
Overall, 5-year survival rates about 50%
Improved prognosis if found in early stages, poor prognosis if metastasis to regional lymph nodes
May present as an:
Exophytic (mass-forming; papillary)
Endophytic (invasive, ulcerated
Leukoplakic (white patch)
Erythroplakic (red patch)
Erythroleukiplakic (combined red and white patch)
Most common intraoral sites:
tongue (posterior lateral and ventral surface); accounts for > 50% cases in the US
floor or the mouth
Gingival and alveolar SCCa are usually painless, and most frequently arise from, posterior mandibular mucosa
Gingival carcinoma least associated with tobacco smoking
> F
Mimic common benign inflammatory and reactive lesions and often destroy the underlying bone
Metastasis occurs largely via the lymphatics to the ipsilateral cervical lymph nodes
A cervical LN that contains metastasis is usually form to stony hard, nontender, and enlarged
Histopathology: malignant epithelial cells and islands seen in underlying connective tissue

Summary
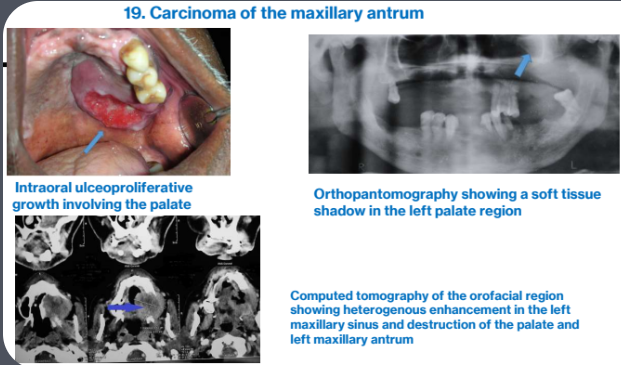
4b. Carcinoma of maxillary sinus
Clinical Features
Patients may have symptoms of sinusitis or referred pain to teeth
may cause malocclusion or mobile teeth
may appear as ulcerated mass in palate or alveolus
Cause
Unknown; some occur in woodworkers
Significance
Prognosis only fair; metastasis are not common
Intraoral ulceoproliferative growth involving the palate
Orthopantomography showing a soft tissue shadow in the left palate region
Computed tomography of the orofacial region showing heterogenous enhancement in the left maxillary sinus and destruction of the palate and left maxillary antrum
Summary

HPV Comparisons (HPV-positive and HPV-negative Oropharyngeal Squamous Cell Carcinoma (OPSCCA))
HPV +ve OPSCCA
Age: younger (40-60 years)
Gender: men > females (8:1)
Race: whites >>> nonwhites
Geographical distribution: Northern Europe and North America
Socioeconomic status: higher
Prevalence estimates and trend: increasing (13–56%)
Etiologic factors: HPV-16 (90–95%)
Risk factors: sexual behavior (high number of sexual partners, history of oral-genital sex, and history of oral-anal sex)
Site: lingual and palatine tonsils, base of tongue, tonsillar crypts
Prognosis: favorable
HPV –ve OPSCCA
Age: older (>60years)
Gender: men > females (3:1)
Race: whites > nonwhites
Geographical distribution: Asia-Pacific
Socioeconomic status: low to middle
Prevalence estimates and trend: stable
Etiologic factors: unknown
Risk factors: smoking, alcohol, smokeless tobacco, betel quid chewing
Site of origin: anywhere in the oral cavity
Prognosis: unfavorable
Characteristic
HPV-positive OPSCCA
HPV-negative OPSCCA
Age
Younger (40–60 years)
Older (>60 years)
Gender
Men > Women (8:1)
Men > Women (3:1)
Race
Whites >>> Nonwhites
Whites > Nonwhites
Geography
Northern Europe and North America
Asia-Pacific
Socioeconomic Status
Higher
Low to middle
Prevalence Trend
Increasing (13–56%)
Stable
Etiologic Factors
HPV-16 (90–95%)
Unknown
Risk Factors
Sexual behavior (multiple partners, oral-genital/anal sex)
Smoking, alcohol, smokeless tobacco, betel quid chewing
Primary Site
Lingual & palatine tonsils, base of tongue, tonsillar crypts
Anywhere in oral cavity
Prognosis
Favorable
Unfavorable