The Heart Beat
Lecture Outline
Electrical conduction in the heart
Cardiac action potentials
Electrocardiogram (EKG/ECG)
Cardiac pumping
Cardiac Cycle
Aims I
Define Sinoatrial node, Atrioventricular node, and Purkinje Fibres.
Describe the conduction of electrical signals (action potentials) through the heart.
Define automaticity, ectopic beat, and chronotropic.
Describe the origin of the heartbeat and the actions of autonomic neurotransmitters on heart rate.
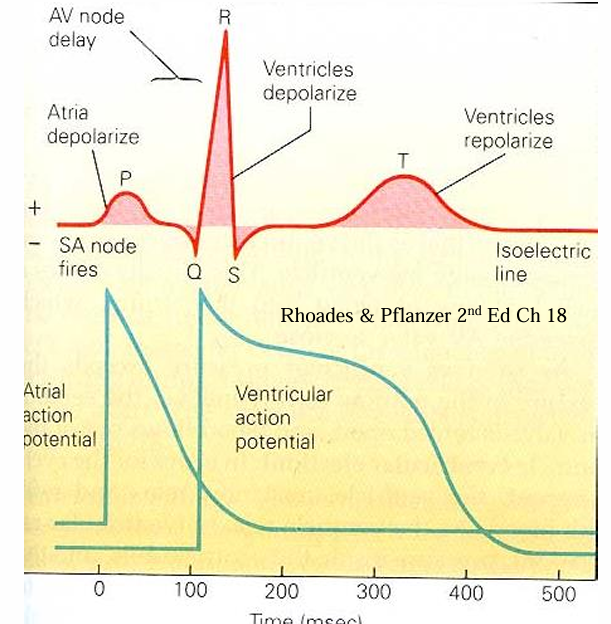
Define EKG/ECG, and list the main waves.
Draw and label a normal EKG.
Aims II
Explain the cause of the main waves present on a normal EKG.
Predict how simple changes in the electrical activity of the heart will alter the EKG.
Define atrioventricular and semilunar valves.
Describe the function of the heart valves and the origin of the heart sounds.
Describe the changes in ventricular pressure and volume that occur during the cardiac cycle.
Draw and label a diagram showing the EKG, heart sounds, and ventricular pressure and volume.
Contraction is Signaled Electrically
Cells are electrically charged.
Nerves and muscle use changes in charge to send electrical signals called Action Potentials.
Cardiac Muscle cells use action potentials to coordinate contraction across the heart and activate contraction.
Electrical Conductivity in the Heart
Myocardial cells are connected by gap junctions, allowing the cardiac action potential to propagate from cell to cell through a low resistance pathway.
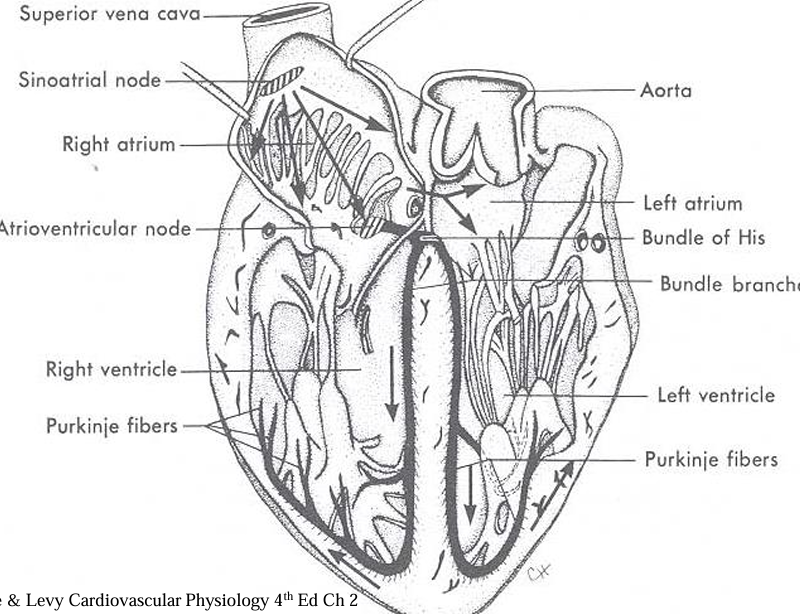
Specialized electrically active cells form the Sinoatrial (SA) node, Atrioventricular (AV) node, Bundle of His, and Purkinje Fibres.
Electrical activity normally originates in the SA node.
The AV node forms the only site of electrical connection between the atria and ventricles.
Propagation of the Cardiac AP*
Action potential (AP) starts at the SA node.
AP conducted through atrial muscle.
AP delayed at the AV node before entering the Bundle of His.
Conduction through the Bundle of His and Purkinje fibres is extremely rapid.
Ventricles depolarize from endo to epicardium and from apex to base.
Autorhythmicity
Some heart cells (SA, AV node, and Purkinje network) show automaticity, the ability to generate a heartbeat.
These cells have an intrinsic rhythmicity which generates a pacemaker potential.
The heart does not require nerve or hormonal input to beat.
In heart transplant patients, the nerves are severed but the heart beats on.
Cardiac Pacemakers
Sinoatrial node has the fastest pacemaker potential (~90-100 beats/min) and is the normal pacemaker.
Atrioventricular node is the next fastest (~40-60 beats/min) followed by cells in the bundle of His (15-30 beats/min).
The fastest pacemaker normally drives the heart and suppresses other pacemakers (overdrive suppression).
A beat generated outside the normal pacemaker is an ectopic beat.
The site that generates an ectopic beat is known as an ectopic focus (foci pl.) or ectopic pacemaker.
Neural Control of Heart Rate
Agents that alter heart rate are chronotropic.
Positive chronotropic agents increase heart rate (e.g., Adrenaline and Noradrenaline acting on β-adrenergic receptors).
Negative chronotropic agents slow the heart (e.g., Acetylcholine acting on M-cholinergic receptors).
At rest, the heart is under parasympathetic tone which slows the natural rhythm of the heart.
Electrical Activity in the Heart
Uses of the EKG:
Heart Rate
Conduction in the heart
Arrhythmias
Direction of the cardiac vector
Damage to the heart muscle
Provides NO information about pumping or mechanical events in the heart.
Heart Valves
The Heart has four valves:
Atrioventricular (AV) valves: Between the atria and ventricles.
Semilunar (SL) valves: Between the ventricles and arteries.
Heart valves prevent backflow of blood.
Forward flow of blood is not impeded.
Closing of the valves produces sounds audible by stethoscope.
Abrupt closure of the AV valves produces S1, the loudest heart sound.
Closure of SL valves produces the second sound, S2.
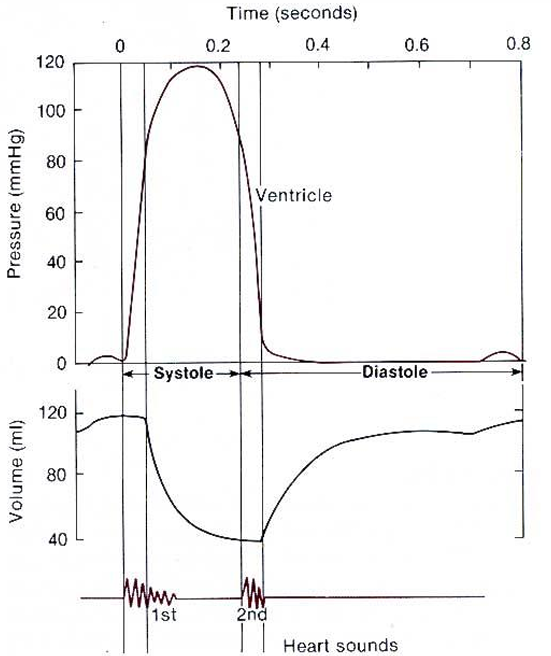
Ventricular Pressure and Volume
After the P wave, atrial contraction slightly increases ventricular pressure.
Following the QRS complex, ventricular contraction greatly increases ventricular pressure.
S1 occurs during ventricular pressure rise.
S2 occurs during the fall in ventricular pressure.
During diastole, the ventricle fills with blood.
Atrial systole adds more blood.
Isovolumic contraction of the ventricles occurs when all heart valves are closed at the start of systole.
During relaxation, there is an isovolumic phase when all heart valves are closed.
Summary
Electrical action potentials initiate the heartbeat.
Action potentials start in the SA node and spread to the ventricles through the AV node.
The ECG/EKG shows electrical events in the heart: P, QRS, and T waves from atrial depolarization, ventricular depolarization, and ventricular repolarization.
Closure of the heart valves produces the heart sounds and prevents reverse flow of blood.
The Cardiac cycle shows the ECG, heart sounds, and the changes in ventricular pressure and volume during the heartbeat.