Unit3- Hemorrhagic Conditions of Late Pregnancy, Placenta Previa, Placenta Abrupto
Hemorrhagic Conditions of Late Pregnancy
Chapter 24 – pp. 507-528
Chapter 25 – pp. 529-554
Chapter 26 – pp. 555-578
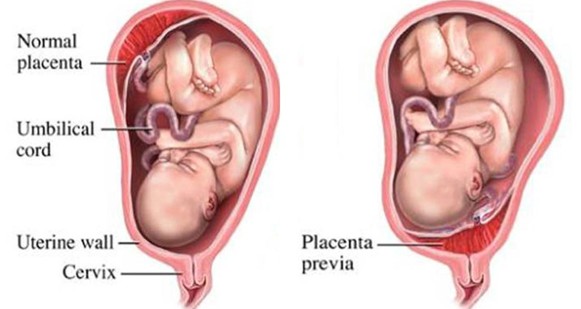
Placenta Previa
Definition:
Implantation of the placenta in the lower part of the uterus leading to potential obstruction of the cervix, which may be either partially or fully obstructed.
Risk Factors for Placenta Previa
Multiparity
History of Cesarean Birth
Previous Placenta Previa
Smoking
Cocaine Use
Signs & Symptoms of Placenta Previa
Painless Uterine Bleeding: Observed particularly in the latter half of the pregnancy.
Teach patients to report any vaginal bleeding that is bright red
No abdominal pain
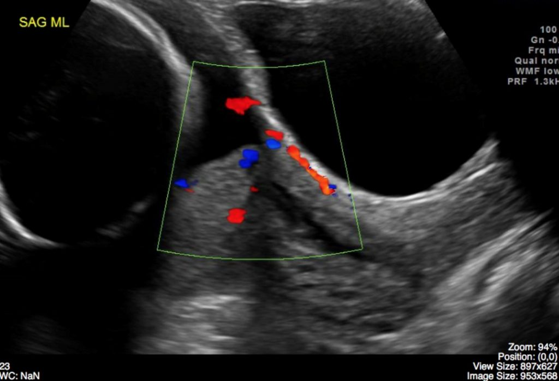
Diagnosis of Placenta Previa
Ultrasound Detection: The primary method for identifying placenta previa during pregnancy.
Therapeutic Management of Placenta Previa
Cesarean Delivery: A planned cesarean section is often necessary if previa is diagnosed.
Patient is bradycardic and hypotensive
Low urinary output
Vaginal pad soaked every 15 minutes
Have emergency equipment handy
Baby may be preterm
Bed Rest: May be indicated if contractions or bleeding occur to decrease complications.
Antepartum Nursing Care - Outpatient Guidelines
Monitoring: Instruct patients to observe and report:
Vaginal discharge or bleeding
Changes in fetal activity
Any contractions or cramping- do not want labor
Pelvic Rest: Avoiding vaginal intercourse to minimize risk of bleeding.
no intercourse
Penetration is a problem
no cervial exams
Antepartum Nursing Care - Inpatient Guidelines
Monitoring:
Continuous assessment of bleeding.
Fetal surveillance via Non-stress tests and/or biophysical profiles.
Prepare for Delivery:
Anticipate an upcoming cesarean delivery.
Obtain consent for potential procedures and blood transfusion.
Ensure IV access for medication and fluids.
Anticipate neonatal needs due to the potential risks.
Caveat: No vaginal examinations should be performed to prevent exacerbating bleeding.
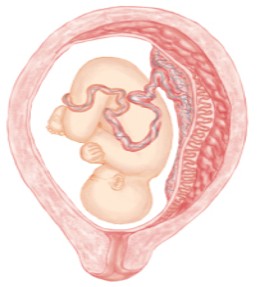
Placental Abruption
Definition:
The premature separation of the placenta from the uterine wall before birth, potentially leading to bleeding and hematoma formation on the maternal side of the placenta.
Blood Flows out

Hematoma
Risk Factors for Placental Abruption
Hypertension
Multigravida
Trauma
History of Abruption
Smoking and Cocaine Use
> 35 years old
Signs & Symptoms of Placental Abruption
Fundal Height Increase
Hard, Board-like Abdomen
Intrauterine Pressure Catheter (IUPC)
Persistent Abdominal Pain
Systemic Signs of Early Hemorrhage
Fetal Heart Rate Patterns:
Persistent late decelerations or decreasing baseline variability.
Vaginal Bleeding: May be present or absent depending on the severity of the condition.
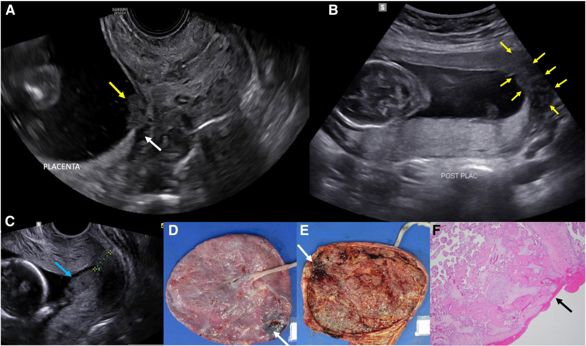
Diagnosis of Placental Abruption
Presumptive Diagnosis: Based primarily on presenting symptoms and history.
Ultrasound Utilization: Gold Standard
Placental Pathology: Examination of the placenta after delivery can provide further insights.
Therapeutic Management of Placental Abruption
Dependent on Maternal and Fetal Status
Cesarean Delivery: May be necessary depending on the stability of maternal and fetal conditions.
Expectant Management: In cases of minor abruption where the mother and baby are stable.
Nursing Care in Cases of Placental Abruption
Priority: Administer cryoprecipitate intravenously
Patients must give informed consent
Side effects: Mild: fever, chills Serious: allergic reaction
Monitoring: Regular assessment of maternal vital signs and fetal heart rate q 15 minutes
Monitor appearance of vaginal bleeding
Monitor uterine resting tone after each contraction
Monitor maternal abdominal girth every hour
Promote Oxygenation:
Position the patient lying flat and lateral to improve blood return and oxygenation to the placenta.
Restrict maternal movement to reduce metabolic demands for oxygen.
Informational Support: Provide simple explanations and reassurance to the patient and family to alleviate anxiety.
IV Access: Ensure intravenous access for fluids, medications, and monitoring.
Just in of fluid and blood being needed
Anticipate Emergency Delivery: Be prepared for possible urgent intervention and neonatal needs based on the condition's progression.
Steroids for baby for lung development- surfactant development