Lec 13 Multisystem Respiratory Conditions: COVID-19 and POTS Study Guide
Fundamentals of Multisystem Respiratory Conditions
Definition: Multisystem respiratory conditions are complex disorders characterized by lung pathology that is intrinsically linked to damage, inflammation, or dysfunction in other major organ systems.
Organ-System Axes: These diseases involve complex interactions including:
Heart-lung axis.
Kidney-lung axis.
Brain-lung axis.
Neuro-lung axis.
Pathophysiological Impact: These interactions lead to inflammatory reactions, hypoxia, and metabolic disturbances, which profoundly impact a patient's overall health and prognosis.
COVID-19: Acute Pathology and Impacts
Etiology: Respiratory disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 ().
Clinical Presentation Categories:
Asymptomatic COVID-19: Observed in approximately of healthy individuals who test positive. While they exhibit no noticeable symptoms, recovery may still show lung damage, predisposing them to future health issues.
Symptomatic COVID-19: Ranges from very mild (barely noticeable) to mild (weak) or moderate (pronounced but manageable).
Severe/Critical: Involves significant respiratory failure and multiorgan impact.
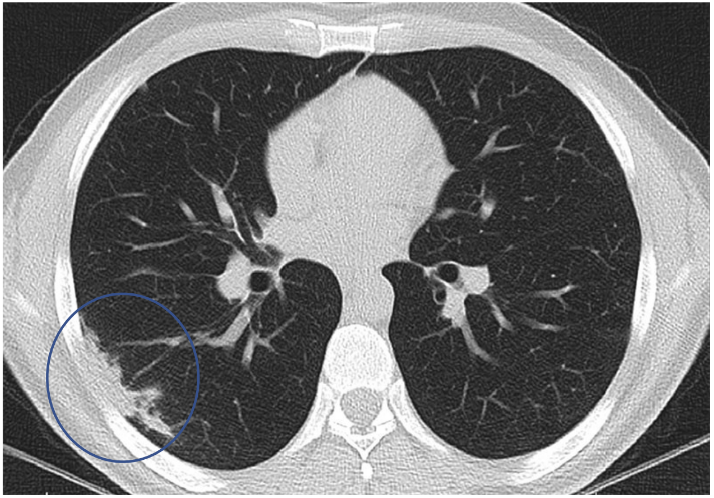
Lung Pathology Findings (Post-Mortem):
Early evidence indicates that lung damage occurs in approximately 20% of patients discharged from hospital
Extensive alveolar damage.
Capillary congestion.
Necrosis of pneumocytes.
Interstitial and alveolar oedema (fluid in air spaces).
Acute Respiratory Distress Syndrome (ARDS): A lung disease triggered by COVID-19 where lungs fill with fluid, making breathing impossible and causing oxygen levels to plunge. The primary treatment is time, involving artificial ventilation until inflammatory fluid subsides.
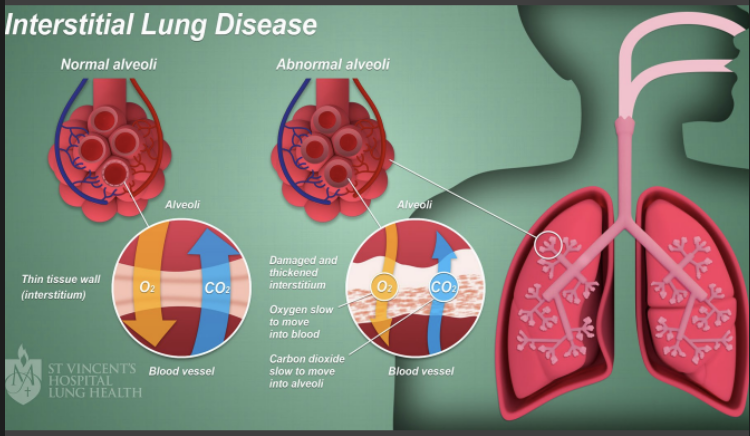
Mechanisms of Lung Damage:
Oxygen enters the lung.
Healthy breathing: Oxygen passes through the air sac (alveoli) into the blood, and oxygenated blood flows to the heart and body.
Breathing with COVID-19: Inflammatory cells pour into the lungs, thickening the membrane and suffocating the alveoli. Oxygen cannot reach the blood, leading to organ failure.
Classification of Disease Severity in Adults
Mild Illness:
No clinical features of moderate or severe disease.
Symptoms: Fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhoea, loss of taste/smell.
No new shortness of breath or difficulty breathing on exertion.
No evidence of lower respiratory tract disease on imaging.
Moderate Illness:
Stable patient with evidence of lower respiratory tract disease.
Oxygen saturation () between on room air at rest.
Desaturation or breathlessness with mild exertion.
Severe Illness:
Patient with signs of moderate disease who is deteriorating OR meeting any of the following:
Respiratory rate .
Oxygen saturation () < 92\% on room air at rest or requiring oxygen.
Lung infiltrates > 50\%.
Critical Illness:
Respiratory failure: Severe respiratory failure (PaO_2/FiO_2 < 200), or presence of ARDS.
Deterioration despite non-invasive support ( or ).
Requirement for mechanical ventilation.
Hypotension, shock, impairment of consciousness, or other organ failure.
Risk Factors for Deterioration and Comorbidities
Age-Based Risks: Individuals over (over for Aboriginal and Torres Strait Islander people).
Demographic/Contextual Factors: Geographical remoteness, socio-economic determinants, and vaccination status (not up-to-date).
Primary Comorbidities:
Respiratory compromise: , asthma, bronchiectasis.
Cardiovascular disease: Hypertension, ischemic heart disease ().
Obesity: BMI > 30\,kg/m^2.
Diabetes and Renal failure.
Immunocompromising conditions: Leukaemias, lymphomas, post-transplant status, high-dose corticosteroids (> 20\,mg prednisone per day for ).
NSW Mortality Data (January 2022 - Under 65s):
Cardiac disease:
Diabetes:
Cancer:
Chronic lung disease:
Obesity:
Kidney disease:
Liver disease:
Asthma:
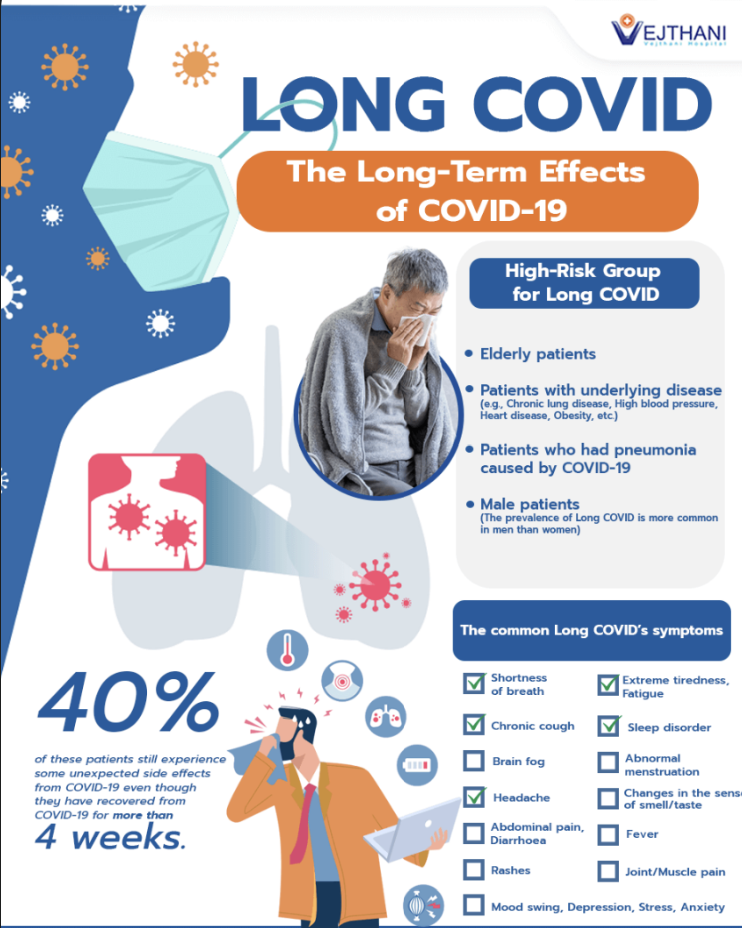
Long COVID and Post-COVID-19 Condition
Temporal Definitions:
Long COVID: Symptoms continuing to after infection.
Post-COVID-19 Condition: Symptoms persisting beyond .
Physiological Impact: Pulmonary fibrosis (stiffness in lungs) leading to long-term breathlessness. This inflammation and scarring is termed Interstitial Lung Disease ().
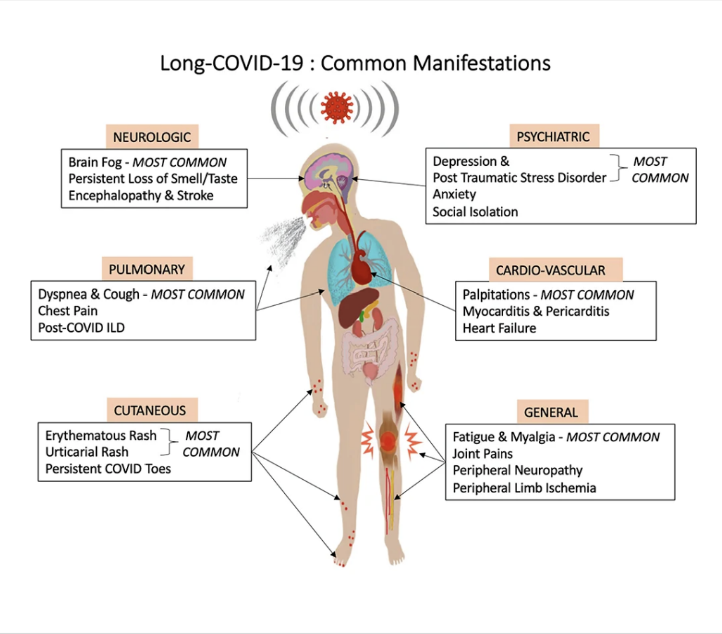
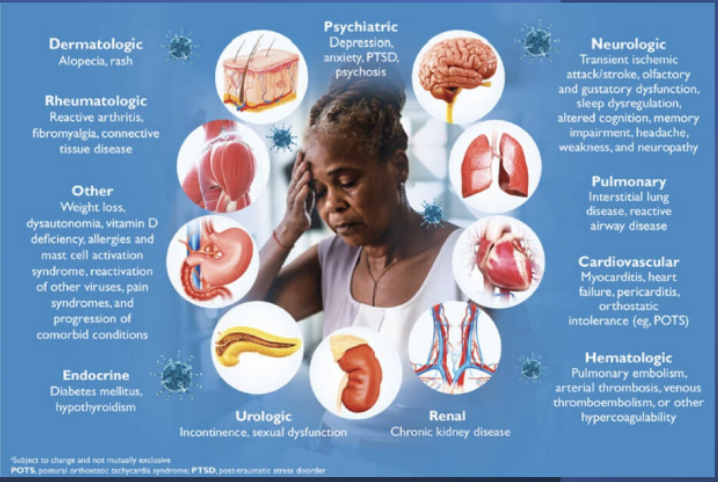
Multisystem Symptoms:
Neurologic: Cognitive impairment (brain fog), memory loss, headache, sleep dysregulation, olfactory/gustatory dysfunction.
Cardiovascular: Myocarditis, heart failure, pericarditis, dysrhythmias, and orthostatic intolerance (e.g., ).
Pulmonary: , reactive airway disease.
Hematologic: Pulmonary embolism, arterial/venous thromboembolism.
Psychiatric: Depression, anxiety, .
Research Findings on Medium-term Effects (2-3 months post-discharge):
Lungs abnormality:
Heart abnormality:
Kidney abnormality:
Fatigue and breathlessness: and respectively.
Assessment and diagnosis of post covis 19 conditions
Confirm with positive PCR
Document details of acute illness
Check current symptoms and ask concerns
Cardiovascular Risks of COVID-19 Antivirals
Remdesivir:
Disrupts viral replication but increases vasodilation of adenosine, inducing catecholamine release. Risks include , , , and
When administered intravenously prolongation (Torsade de Pointes). Requires continuous heart monitoring.
Paxlovid:
May cause bradycardia and sinus dysfunction. High toxicity risk when combined with tacrolimus; increases bleeding risk with anticoagulants (warfarin); may cause myopathy and skeletal muscle breakdown.
Ivermectin: Accumulates in the heart and inhibits potassium currents. Requires monitoring for arrhythmias and prolongation.
Initial Screening for long covid
What severity category did the client fall into
What symptoms did the client have during infection
was the client treated at home
if hospitalised, how long for, was the client in ICU, were they on ventilator, did they develop any related disorders or disease
what population
does client have any pre-exisiting conditions
pre existing PA levels
what is the clients current infection status
how many days since last day of symptoms

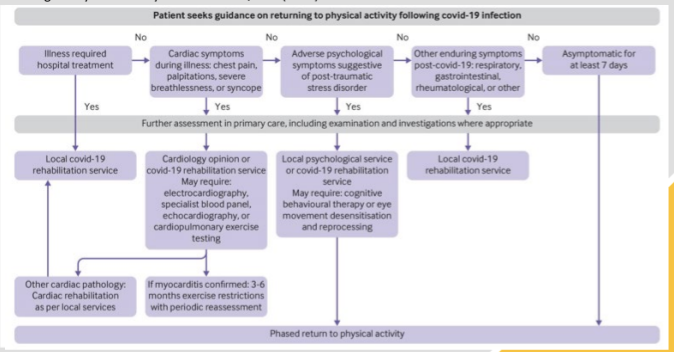
Exercise Rehabilitation for Post-COVID-19 Syndrome
Risk Stratification (BMJ 2021): Return to exercise only after at least symptom-free. If the patient had severe illness or cardiac symptoms (chest pain, palpitations), a cardiology opinion is required.
The Phased Return to Physical Activity:
Phase 1 (): Preparation; deep breathing, stretching, balance, gentle walking.
Phase 2 (): Low intensity; yoga, light garden tasks. Graduate by .
Phase 3 (): Moderate intensity aerobic/strength; 2 intervals of aerobic activity.
Phase 4 (): Coordination and functional skills; training to recovery day ratio.
Phase 5 (RPE > 15): Baseline exercise; return to regular exercise pattern.
Johns Hopkins Phases:
Beginning: Deep breathing (back/stomach), eye nods, bed rolling, seated cross-crawl.
Building: Deep breathing (sitting/standing), head rotations, rocking to stand, bird-dog, bicep curls ( cardio).
Being: Standing deep breathing, mini squats, wall push-ups ( cardio).

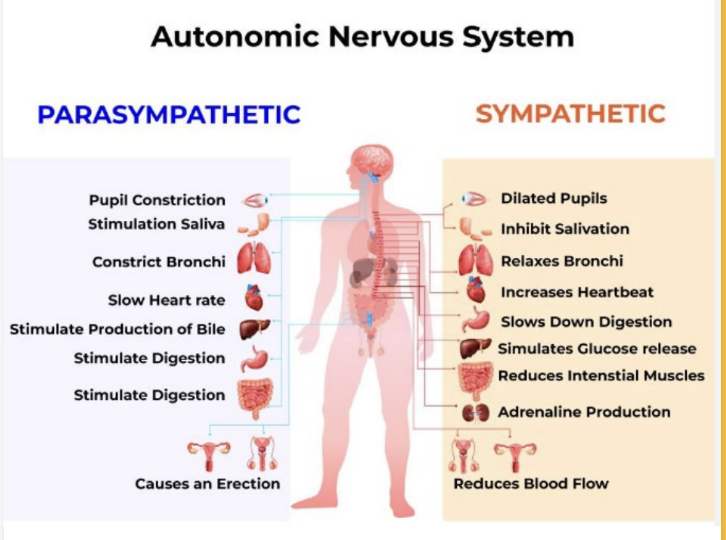
Postural Orthostatic Tachycardia Syndrome (POTS)
Definition: A clinical syndrome lasting at least involving the Autonomic Nervous System ().
Heart Rate () increase > 30\,\text{bpm} (> 40\,\text{bpm} for ages ) within of quiet standing.
Absence of orthostatic hypotension (> 20\,mmHg drop in or drop in ).
Typical Demographic: Young women (mean age ; women).
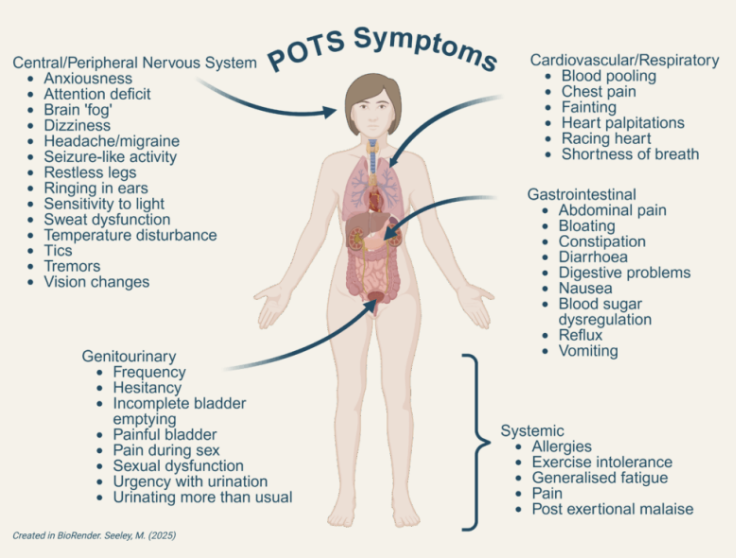
Symptoms:
Heart: Palpitations, chest pain, tachycardia.
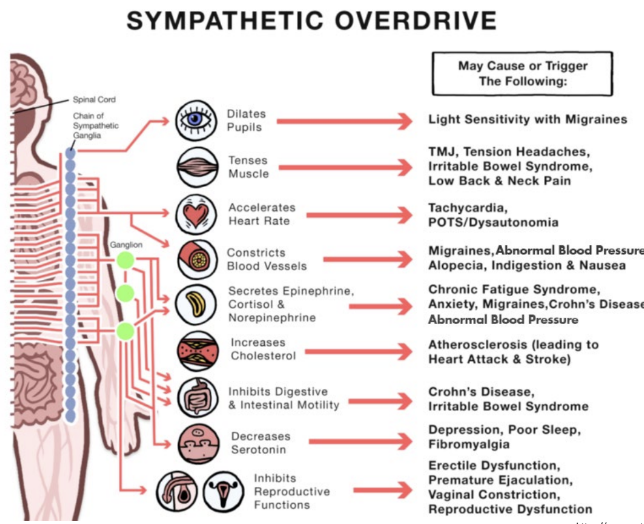
Neurological: Brain fog, light sensitivity, migraines, tremors.
Gastrointestinal: Nausea, bloating, diarrhoea, abdominal pain (often due to decreased motility from sympathetic activation).
Other: Exercise intolerance, generalized fatigue, temperature disturbances.
POTS Sub-types:
Neuropathic: Decreased sympathetic innervation in legs; blood pooling, blue/warm feet.
Hyperadrenergic: Increased noradrenaline and ; tachycardia, palpitations, tremor.
Hypovolemic: Low blood volume (plasma and ); weakness, low exercise tolerance.
Volume Dysregulation: Secondary to impaired functioning.
Pathophysiology and Mechanisms of POTS
Deconditioning: Cardiovascular deconditioning characterized by cardiac atrophy and hypovolemia (similar to astronauts post-spaceflight).
Venous Return Mechanisms:
Skeletal Muscle Pump: Limb muscles squeeze veins (e.g., Calf Raises).
One-Way Valves: Prevent backflow.
Respiratory Pump: Inhalation pressure changes push blood upward.
Venomotor Tone: Sympathetic activation constricts veins.
Cardiac Suction: Expansion of the right atrium draws blood in.
Trigger Events: Infection (most common), surgery, concussion, or enforced bedrest.
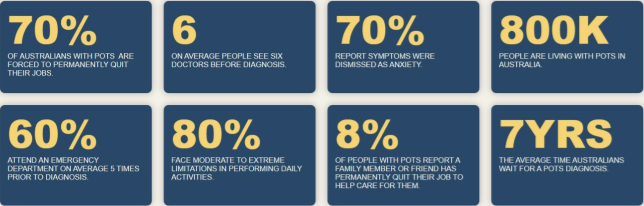
Societal Impact in Australia:
people living with .
forced to quit jobs.
average time for diagnosis.
Management and Exercise in POTS
Conservative Management:
Fluid intake: .
Salt intake: .
Eating: Small, frequent meals.
Garments: Compression leggings to aid venous return.
Environment: Avoid heat and large alcohol intake.
Medications:
Midodrine (vasoconstrictor).
Ivabradine (lowers heart rate).
Fludrocortisone (increases blood volume).
Propranolol (beta-blocker).
Exercise Prescription Guidelines:
Horizontal Exercise: Start with rowing or recumbent cycling to maximize venous return without orthostatic stress.
Heart Rate Control: Keep below sympathetic activation ().
Resistance Training: Focus on lower limb muscles to enhance the skeletal muscle pump (Leg press, Calf press, Glute bridges).
Progression: Gradually add upright exercise as tolerance increases.
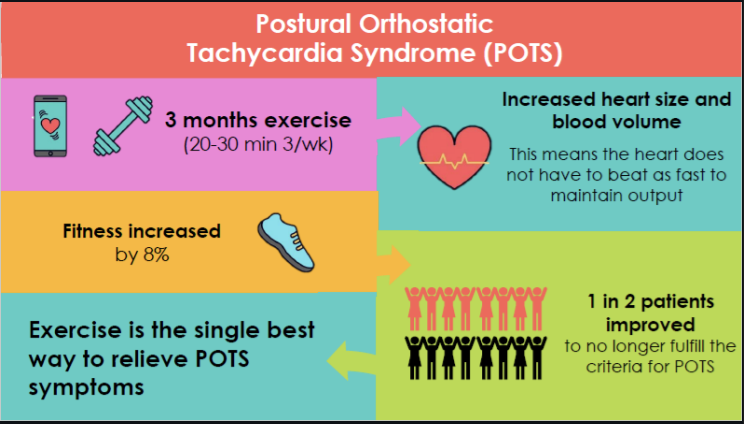
Efficacy: A program (, ) can increase heart size and blood volume, with in patients no longer fulfilling criteria.

Complementary Practice: Vagus nerve stimulation via deep breathing, humming, singing, and mindfulness.
Calf raises
avoid deep squats and leg crosses
Eccentric exercises