V. PERIPHERAL VASCULAR DISEASE
Positioning
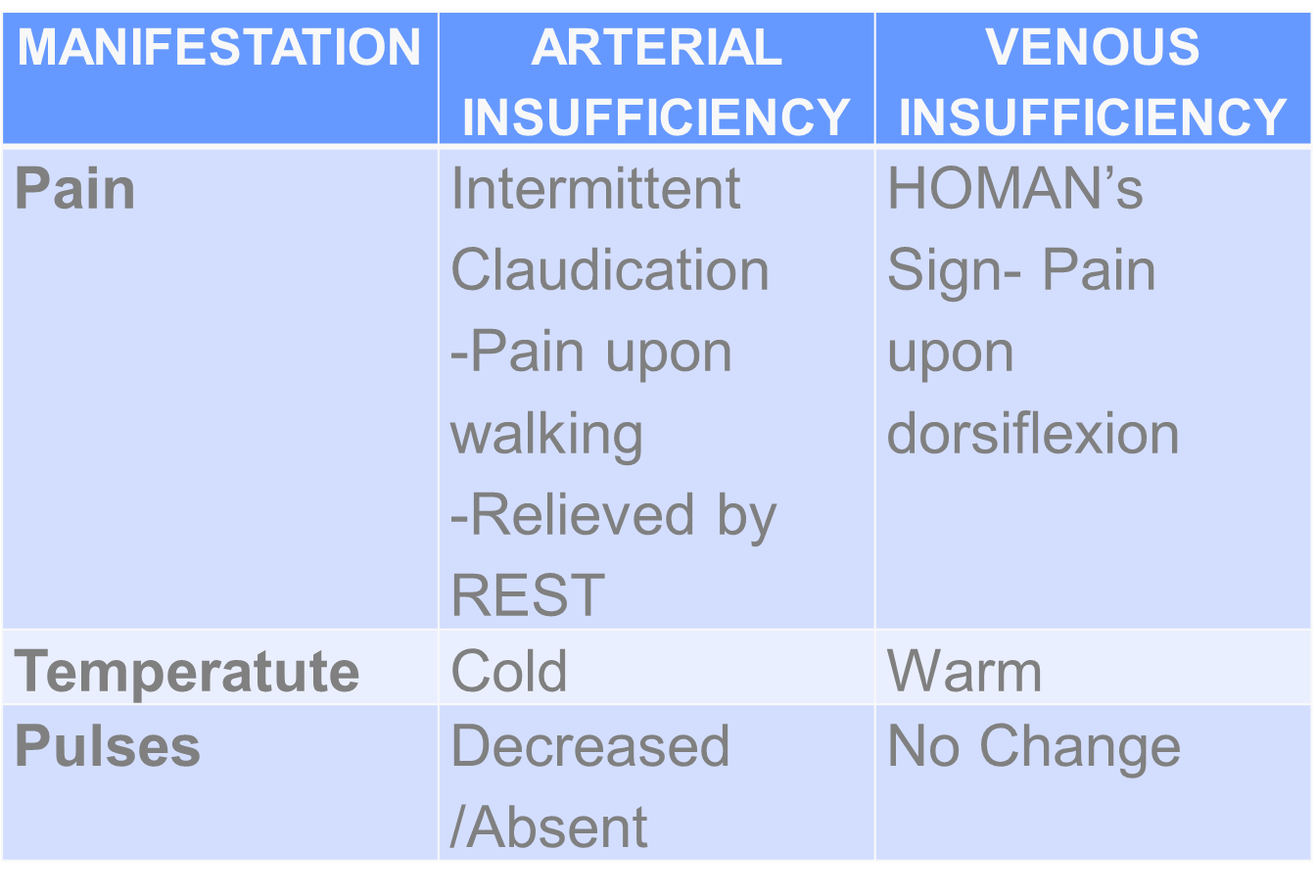
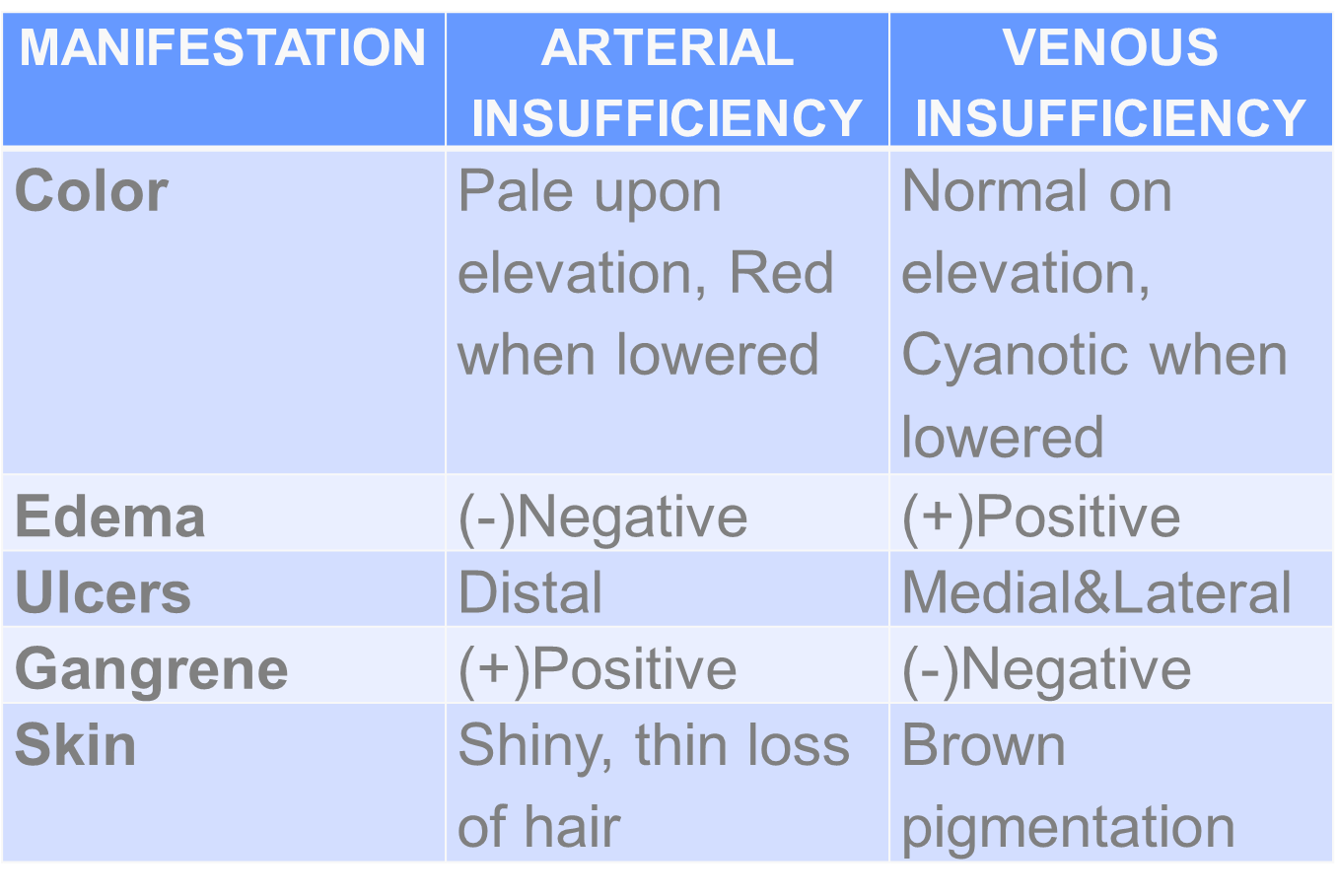
ARTERIAL: Flat on Bed
VENOUS: Elevated
Patency of the vessel
1. ATHEROSCLEROSIS OBLITERANS (ASO)
Chronic inflammation of vessels due to atheroma
2. THROMBOANGINITIS OBLITERANS (TAO)
Buerger’s Disease
Common: Men
Trigerred by: Smoking
BV = small and medium sized arteries of hands and feet
Hallmark Signs ( 6 P’s)
Paresthesia (Earliest)
Pain
Pallor
Paralysis
Poikilothermia
Pulselessness
Diagnostic Test:
Ankle Brachial Index
Formula: Ankle Pressure/Arm Pressure
110/70 / 120/80
40/40 = 1
Interpretation: If >.90 = Normal
0.71-0.90 = Mild
0.41-0.70 = Moderate
0.00-0.40 = Severe
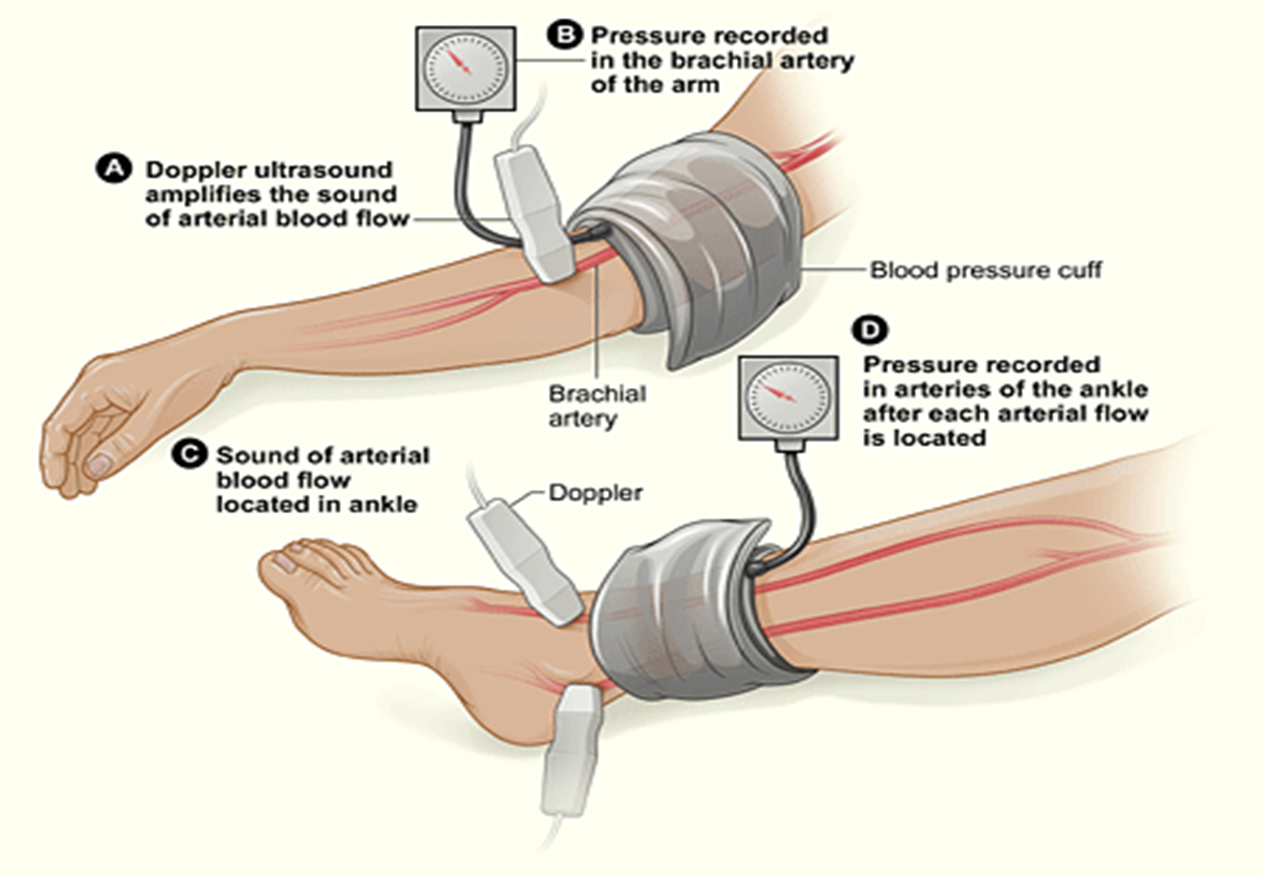
Doppler UTZ= monitor BV based on turbulence
Arteriography – Most reliable
MANAGEMENT
P – Promote adequate tissue perfussion
U – Understand Medications
Pentoxifylline
Papavarine
Plasma Expanders (Dextran)
Anticoagulant
Platelet Inhibitor
Antithrombotic (Cilostazol)
L – Limit/Stop Smoking and Caffeine
S – Safety of the leg = heat sensitive
No warm compress on the leg
Place it on the abdomen
Insulated leather shoes
E – Exercise: Buerger-Allen’s Exercise
Elevate extremities 5 degrees
Dangle the legs
Flat on bed
S – Surgery
Femoral-popliteal bypass graft
Rotational Atherectomy
Amputation
Pre-Op:
Psychological Preparation
Teach to prevent deformity
Phantom limb sensation
Post-Op:
Monitor for bleeding (always have a tourniquet)
No pillow under the knee (can cause flexion deformity)
Passive ROM
Prepare for crutchwalking
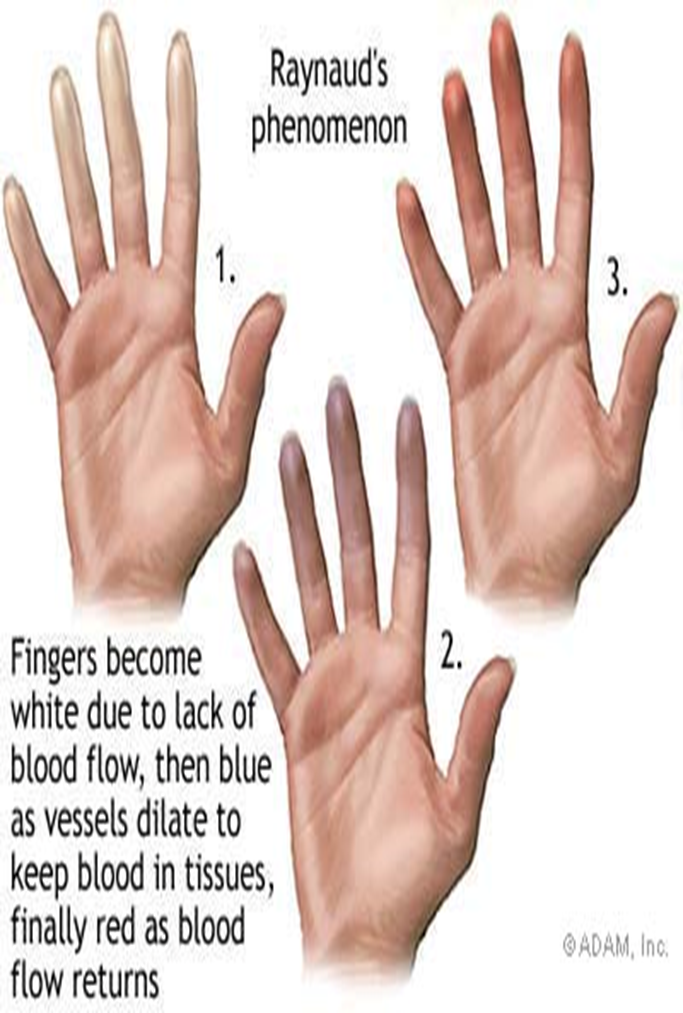
3. RAYNAUD’s PHENOMENON
– unknown etiology
Common : Female
Trigerred by : Smoking, Stress, Cold environment
Hallmark Sign: Flat color changes sign
Pallor = Whole - Vasoconstriction
Cyanotic = Blue - Vasoconstriction
Erythema = Red - Vasodilation
Diagnostic Test: Allen’s Test
Management
Reduce stress
Avoid cold environment
Use gloves and mittens
Use brandy/whisky (black label, red label)
Monitor pulse
Administer vasodilator
4. VENOUS DISORDERS (DVT)
PATENCY OF THE VESSELS
A. Inflammatory: Thrombophlebitis
Etiology
Hypercoagability of the blood
Endothelial Injury – blood vessel wall damage
Venous/Blood stasis- decrease venous return
Signs and Symptoms
Homan’s Sign
Increase in leg girth
Erythema of the leg
Edema
Management
Bedrest
Don’t massage(leg)
Elevate
Apply warm compress
Use elastic support
Improve hydration
Anti-coagulants
B. Functional: Varicose Vein
– abnormal dilation of vessel wall of vein
Etiology
Congenital, genetically weak BV
Prolonges sitting and standing
Signs and Symptoms
Dilated Tortorous vein
Dull achy sensation of the leg at the end of the day
Management
Elevate the leg
Foot massage
Note color changes
Hose applications
Ulcer treatment:
Stasis Dermatitis = non-healing ulcer of the leg
UNNA PASTE BOOT = dressing with zinc oxide to facilitate wound healing
Vein Stripping = veins larger for 4 months
Sclerotherapy = injection of solution to hardened vessels (2 -3 weeks)
Incision and Drainage
Pressure dressing for 12-18 hours
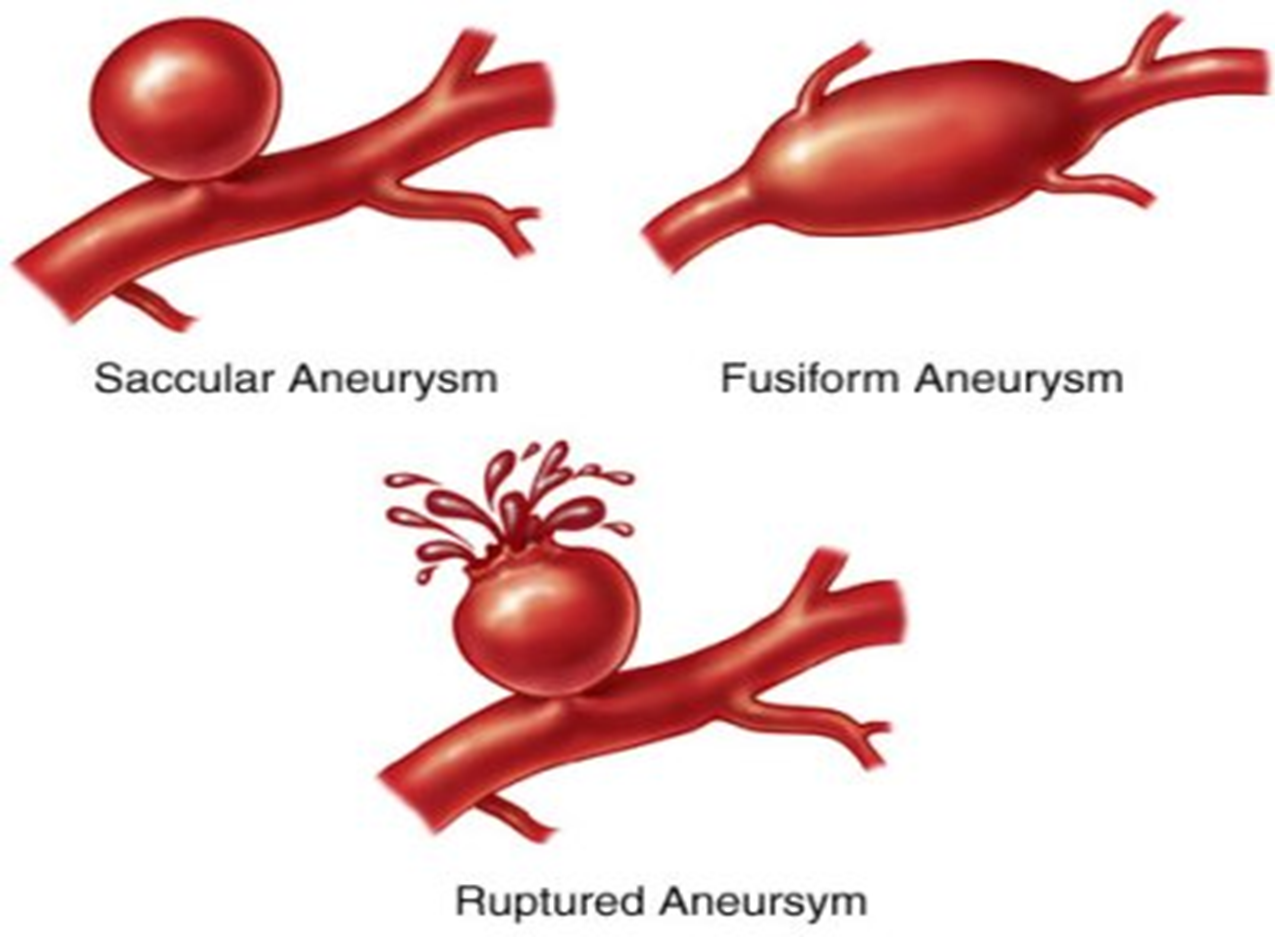
C. DEGENERATIVE: ANEURYSM
out patching of the artery due to damage in tunica media (congenitally weak)
Etiology:
S - Syphilis
A - Artherosclerosis (70%) enhanced by HTN
M - Marfan Syndrome
S – Sacular (one-sided dilated)
F – Fusiform ( 2 sided dilated)
D – Disecting (more sided dilated)
A – Abdominal
A – Aortic
A – Aneurysm
Consideration:
Do not palpate the abdomen = it can rupture
Asymptomatic
Abdominal mass pulsation
Flank pain/ Abdominal Pain (sign of aneurysm)
Sudden sharp knifelike pain (ruptured aneurysm)
D. CONSTRICTIVE: HYPERTENSION
TYPES
Primary = BP grading of 140/90 mmHg in 2 consecutive readings with 4-6 hours apart, unknown cause
Secondary = Secondary to disease
Ex. Chronic Renal Failure
Isolated = Calcification of Aorta R/T aging process
Seen in elderly
Asymptomatic
Most dangerous because it is related to high incidence of stroke
Malignant = Occipital headache due to anatomical placement of brain stem
Epistaxis
Paresthesia
Occipital Headache
MANAGEMENT
1. Lifestyle Modification
Diet: Prudent diet
Low alcohol
Stop smoking
2. Pharmacologic approach
A – ACE INHIBITORS “PRIL”
Vasoconstrictor
Side Effects: Bradycardia, HOPN, Pruritus, Cough, Angioedema
Nursing Considerations
Monitor the action of the drug
Contraindications
Patients with Renal Insufficiency
B – BETA BLOCKERS “OLOL”
B1 = Heart
Increase in Cardiac Rate, Increase BP
B2 = Lungs
Bronchodilation
P – Propranolol (Inderal)
A – Atenolol
T – Timolol
Contraindications: CHF/COPD
M – Metoprolol (Lopressor)
N – Nadolol (Corgard)
Blocks B1 can be given to asthmatic patients
C – CALCIUM – CHANNEL BLOCKERS
(-) INOTROPIC EFFECT = blocks the entrance of Calcium in the myocardial cell
Decreases Cardiac Contraction
C – Calan (Verapamil)
C – Cardizem
C – Calcibloc
A – Amlodipine (Norvasc)
N – Nifedipine (Procardia)
Contraindications: CHF
D – DIURETICS
A – Aldactone (Spinorolactone) K Sparring
Side Effects: Hyperkalemia = Irregular heartbeats
B – Bumex = Ototoxicity
C – Chlorthiazide ( Diuril) = K wasting; can cause Pancreatitis- monitor Amylase
F – Furosemide (Lasix) = Loop Diuretic