psychotropics and psychostimulants: use and abuse (adrenergic pharmacology)
The monoamines are noradrenaline, dopamine (catecholamines - catechol group) and serotonin (tryptamine - indol group)
Noradrenaline
There are two main nuclei in the brain that produce noradrenergic fibres:
locus coeruleus which has projectrions throughout the brain
lateral tegmental area which has projections and signals through the spinal cord
Activation of the noradrenergic fibres result in different behaviours such as alertness, arousal (forebrain - fight or flight) as well as regulating mood , pain and blood pressure
Dopamine
there are a few nuclei where dopaminergic fibres arise from:
ventra tegmental area - projections to the forebrain
important for decision making
affected by addiction - drug target
substantia nigra - projections to the middle brain
dopaminergic neurons degenerate in parkinson’s diseases
activation of dopaminergic fibers result in control in motor, behaviour, mood and endocrine function
ALL DOPAMINERGIC RECEPTORS AND G PROTEIN COUPLED
There are two major dopamine receptors: D1 and D2 like each of which can be broken down into groups
D1-LIKE
These can be broken down into D1 and D5 subgroups which are coupled to the g protein subgroup Gas. The second messengers for this include increased cAMP and PKA activity
D2 LIKE
These have the subgroups D2,D3 and D4 subgroups that are coupled to Gai g proteins. The second messengers to the activation of these are reduced cAMP and PKA activity. the gby subgroup also reduces the activity of VG Ca2+ channels and opens K+ channels
Activation of any receptors leads physiological responses such as voluntary movements, reward, sleep, mood/cognition/attention, hormonal activity, nausea and sympathetic activity
Serotonin
Serotonin has very extensive projections through the brain with the primary nucleus being the Raphe nucleus. It extends all the way through the brain meaning it is involved in many different behaviors such as:
sleep, wakefulness and mood
feeding behaviour
control of pain and sensory transmission
There are many receptors for serotonin ( 5-HT1-7)
5-HT1 is coupled to a gai receptor
5-HT2 is coupled to a gaq receptor
second messenger include PKC and Ca2+
5-HT3 is an ion channel for Na+ and Ca2+
5-HT4,5,6,7 are coupled to Gas
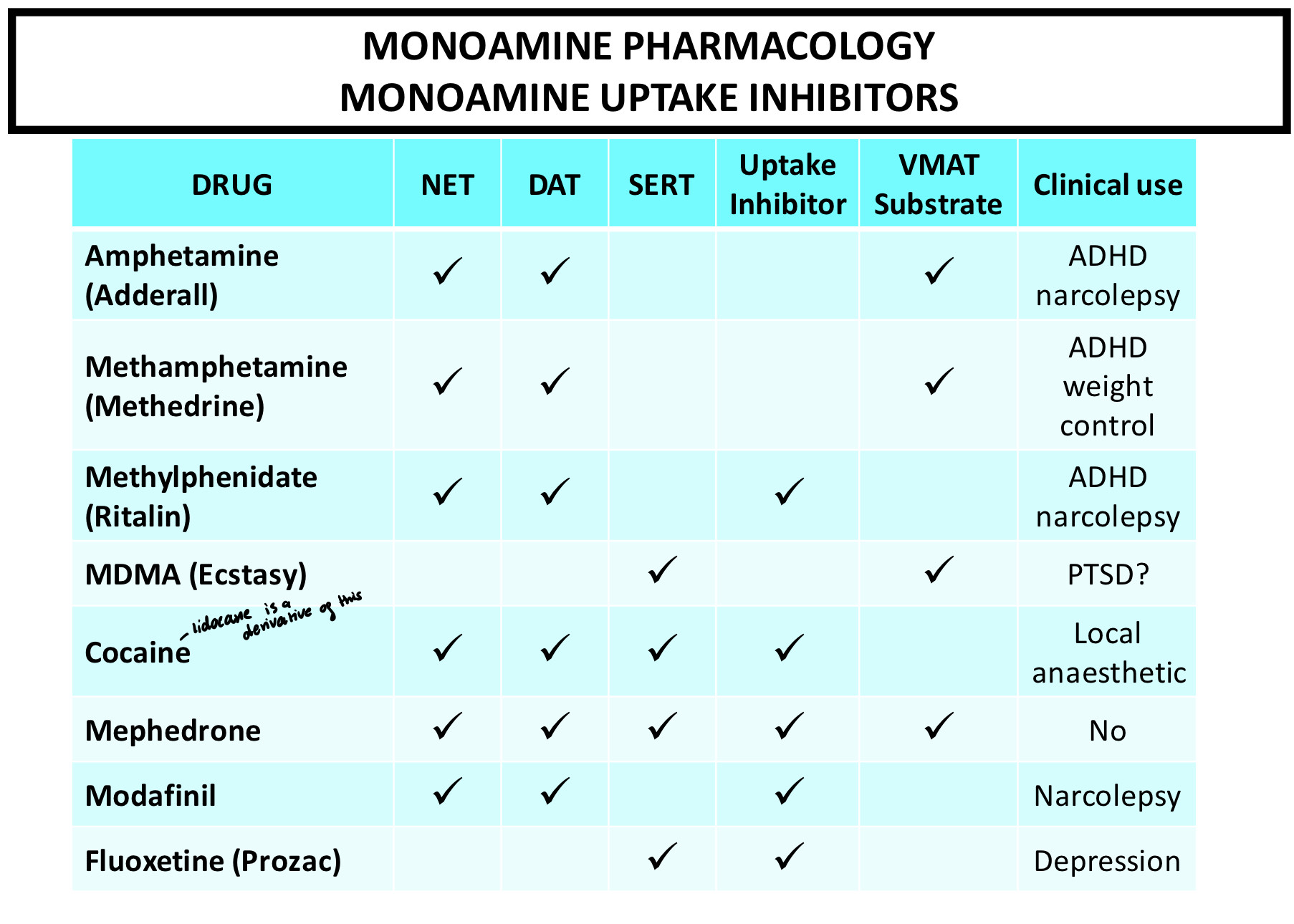
Monoamine uptake and inhibition
Monoamine uptake into vesicles happens via the same mechanism as the uptake of ACh into vesicles. Many psychoactive drugs target and inhibit the uptake of monoamines at the plasma membrane or the synaptic vesicles and lead to monoamine accumulation in the cleft
Cocaine and dopamine
Cocaine inhibits dopamine uptake by blocking the transporter which allows the reuptake of it into the presynaptic terminal. This leads to accumulation of dopamine in the cleft which is responsible for the immediate rush felt after
MDMA and serotonin
MDMA is taken up the serotonin transporter which allows the accumulation of serotonin in the cleft. It also competes for the vesicle which means more secretion of it
Amphetamine and noradrenaline
Amphetamines are taken up by the noradrenaline transporter and also compete for the vesicle with it however they also inhibit MAO enzymes so noradrenaline in the cleft is not broken down
 Stimulant properties of amphetamines
Stimulant properties of amphetamines
The main effects of amphetamines are:
increased motor activity
euphoria and excitement
insomnia
anorexia <3
The effects are due mainly to increased levels of monoamines in the synaptic cleft. They were used at stimulants during WW2 due to these effects
They can also induce strong psychological dependance and psychosis can occur with prolonged use which resemble schizophrenia
Clinically, they can be used to read ADHD or narcolepsy as low doses help to focus attention. Obesity can also be treated in severe cases
Stimulant properties of cocaine
The main effects of cocaine are:
increased motor activity
euphoria, excitement and garrulousness
increased peripheral sympathetic NS activity
They cause strong psychological dependance and the effects are mainly due to the increased levels of monoamines. Cocaine has shorter lasting effects compared with amphetamines
Modafinil
Modafinil is thought to affect the dopamine transporter. When a PET scan was taken with labelled cocaine, it bound very strongly however with modafinil, cocaine did not bind as strongly.
The main effects are:
increased wakefulness and vigilance
suggested to improve cognitive performance
Modafinil binds with low affinity to DAT and to NET and has additional actions at a variety of NT systems as well as a low abuse potential
Cognitive enhancers are hoped to:
reduce mental fatigue
maintain attention and concentration
increase motivation
normalise behaviour
schizophrenia
autism disorders
addiction
ampakines
ampakines enhance the activation of glutamate AMPA receptors. They promote the release of brain derived neurotrophic factor and show evidence of enhancing cognition in a range of tests (the rat one)
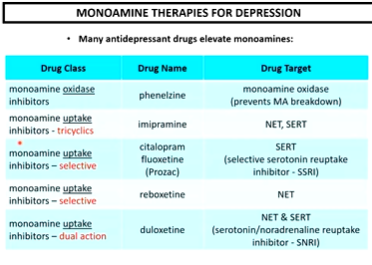
The monoamine theory for depression was first proposed by Jow Schildkraut in 1965 and it is based on the theory that drugs that enhance monoamine levels improve mood and symptoms of depression
There are various signs of depression that clinicians use in the diagnosis of depression which could be caused by messed up monoamine levels. Antidepressants essentially normalise the levels of the neurotransmitters which can be used to alleviate some of the symptoms
 Dopamine and schizophrenia
Dopamine and schizophrenia
Schizophrenia is a condition that displays positive, negative and cognitive symptoms.
Positive symptoms relate to over activity in the mesolimbic dopaminergic pathway activating dopamine D2 receptors
Negative symptoms relate to decreased activity in the mesocortical dopaminergic pathway in D1 receptors
Cognitive receptors relate to attention and memory - mesocortical pathway
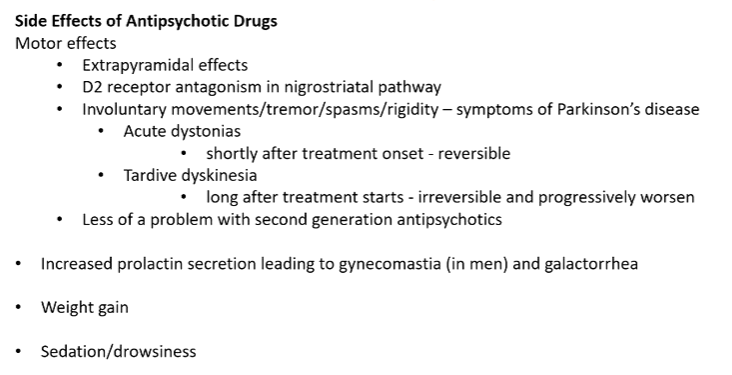
Therapies
There are two generations of antipsychotics
The first generation target D1 and D2 receptors while the second generation has some activity in D1 but more in D2
 Dopamine and Parkinson’s disease
Dopamine and Parkinson’s disease
Parkinson’s disease is a neurodegenerative disorder in which patients display a profound motor impairment
It has a suppression of voluntary movements with a tremor at rest and increased resistance in passive limb movement with a variable degree of cognitive impairment