Week 8: Disruptive Behavior Disorder & ADHD
Introduction to Disruptive Behavior Disorders
Disruptive behavior disorders involve difficulty regulating emotions or behaviors, typified by persistent patterns of anger, hostility, and aggression.
Targeted behaviors can be directed towards people and property.
Primary disorders:
Oppositional Defiant Disorder (ODD)
Conduct Disorder
Intermittent Explosive Disorder (IED)
Continuum Concept:
ODD and Conduct Disorder are viewed on a continuum with Antisocial Personality Disorder.
Some view ODD as a milder variant of Conduct Disorder.
IED is characterized as an impulse control disorder involving aggression toward people and property and is typically diagnosed from adolescence to young adulthood.
Related Disorders
Kleptomania vs. Pyromania (Behavior conditions that can start during childhood)
Kleptomania:
Characteristics: Impulsive, repetitive theft of unnecessary items, high tension before theft, relief during theft, stolen items often discarded.
Demographics: More common in females, negative legal, career, family, and social consequences.
Pyromania:
Characteristics: Repeated intentional fire setting, fascination with fire, pleasure during fire setting, absence of external motivations, no monetary gain or revenge.
Legal implications: Rare as a primary disorder, it often leads to legal system involvement rather than mental health treatment.
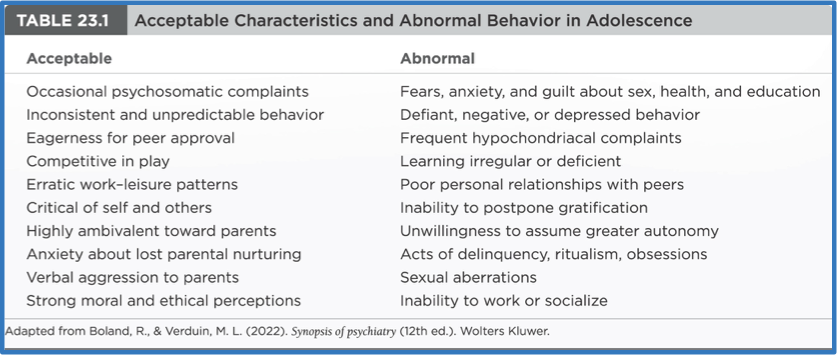
Normative Adolescent Behaviors
Discussion on behaviors considered "normal," "typical," or "expected" during adolescence versus those that are not tolerated.
Oppositional Defiant Disorder (ODD)
Common in children and adolescents.
Expected behaviors at certain phases (e.g., ages 2-3 and early adolescence).
Diagnosis Criteria:
More frequent and intense behaviors than peers, and intense behavior towards authority (parents, teachers, etc.).
Causes dysfunction in social, academic, or work situations.
Initial Settings:
Begins at home with parents or parental figures, often more intense at home.
Prevalence Rates:
2% to 15% of the adolescent population, with an average of 3% to 5% in the United States.
More common in males, although recent years show an increase in female adolescents.
Contributing Factors:
Genetics, temperament, adverse social conditions, lower self-concept, and lack of competence in social situations.
Common Behaviors in ODD
Enduring patterns of uncooperative, defiant, disobedient, and hostile behavior toward authority figures.
Common Behaviors:
Frequent temper tantrums.
Argumentative with authority figures.
Refusal to comply with rules.
Deliberately annoying others.
Risk Factors:
Family history of mental health disorders.
Inconsistent disciplinary practices.
Ex. Going to different parents’ houses during divorce with different house rules.
Exposure to violence or trauma.
Treatment Approaches:
Parent management training.
You have to treat the family system, not solely the child.
Cognitive-behavioral therapy.
Changing your mindset/thinking, cognitive restructuring. Creating a more flexible mindset by analyzing thoughts and emotions.
Social skills training.
Prognosis Factors for ODD
Behavioral characteristics include:
Limited ability to associate behavior with consequences.
Impaired problem-solving abilities.
Deficiencies in attention, flexibility of thinking, and decision-making.
Prognosis Factors:
Age of onset, symptom severity, and presence of comorbid psychiatric disorders.
Early onset is linked to poorer long-term outcomes and increased risk for Conduct Disorder and Antisocial Personality Disorder.
Comorbid Disorders and Treatment of ODD
Common comorbid psychiatric disorders include ADHD, anxiety, and mood disorders.
Treatment must address comorbid conditions with specific approaches:
Parent management training targeting behavioral interventions.
Ignoring maladaptive behaviors while rewarding positive behaviors.
Interventions that enhance personal strengths (e.g., the Coping Power Program).
Intermittent Explosive Disorder (IED)
Definition and Characteristics
IED is characterized by repeated episodes of impulsive, aggressive, violent behavior disproportionate to the situation, with angry verbal outbursts lasting less than 30 minutes.
Typically longer in clients with autism, uncontrollable.
Diagnosed typically from adolescence to young adulthood, and can follow stressful situations, frustrations, or perceived threats.
Emotional Outburst Characteristics:
Intensity disproportionate to the stressor.
Minor issues may trigger significant rage or aggression.
Feelings of embarrassment, guilt, or remorse post-episode, but a lack of prevention for future outbursts.
Demographics of IED
Common onset during adolescence to young adulthood.
Can occur after 6 years of age; often diagnosed from adolescence to young adulthood.
Gender Prevalence: More common in males.
Common Comorbid Psychiatric Disorders:
Substance use disorder.
ADHD.
ODD and Conduct Disorder.
Anxiety disorders and depression.
Etiology of IED
Childhood factors linked to IED:
Exposure to trauma, neglect, and maltreatment.
Neurotransmitter imbalances:
Serotonin deficiencies.
Plasma tryptophan depletion.
Frontal lobe dysfunction leads to correlation with physical outcomes like coronary heart disease, hypertension, stroke, diabetes, arthritis, and chronic pain.
Dysfunction could also be caused by continuous injuries.
Treatment for IED
Psychopharmacology Treatments:
SSRIs like Fluoxetine (Prozac).
Lithium as a mood stabilizer for labile mood/behaviors.
Cannot be given if pregnant.
Anticonvulsant mood stabilizers (e.g., valproic acid [Depakote], phenytoin [Dilantin], topiramate [Topamax], oxcarbazepine [Trileptal]).
Medication Effects:
Reduce aggressive impulses and irritability, but do not eliminate outbursts.
Cognitive Behavioral Therapy (CBT):
Goals include identifying triggers for aggressive outbursts, developing coping strategies, and improving emotional regulation.
Techniques include cognitive restructuring, behavioral modification, and problem-solving skills, aiming for reduced frequency of outbursts and improved interpersonal relations.
Anger Management Strategies for IED
Techniques for managing anger include:
Deep breathing exercises.
Progressive muscle relaxation.
Visualization techniques.
Regular practice for sustained benefits, setting aside time for relaxation.
Importance of avoiding triggers by recognizing and avoiding situations that provoke anger and developing alternative responses to stressors.
Role of support systems such as family and friends, professional counseling, and support groups.
Conduct Disorder
Expected Findings
Conduct Disorder characterized by:
Persistent behavior violating societal norms, including aggression towards people and animals, destruction of property, deceitfulness, theft, and serious rule violations.
Involves callous and unemotional traits, indicating a lack of empathy, guilt, or remorse, and shallow emotions.
Harm/kill animals, family pets, or seek easy human targets.
Associated behaviors include early sexual behavior, substance use, and risky behaviors with potential progression to Antisocial Personality Disorder in up to 40% who are diagnosed as adults.
Onset and Clinical Course
Subtypes Based on Age at Onset:
Childhood-onset: symptoms before age 10, primarily in boys, with physical aggression and disturbed peer relationships, higher risk of persistent Conduct Disorder and Antisocial Personality Disorder.
Adolescent-onset: symptoms after age 10, observed in both genders, typically showing less aggression and more normal peer relationships, presenting a lower risk of persistent disorders.
Etiology and Contributing Factors of Conduct Disorder
Risk Factors:
Family history of Conduct Disorder, Antisocial Personality Disorder, and substance use disorder.
Prenatal exposure to alcohol, child abuse, inadequate housing, unstable environments, poverty, poor parenting, and low academic achievement.
Protective Factors:
Positive role models, healthy peer relationships, participation in extracurricular activities, and strong academic performance.
Neurobiological Research: Shows how autonomic nervous system unresponsiveness correlates with increased aggression.
Similar to adults with antisocial personality disorder.
Treatment of Conduct Disorder
Emphasis on early intervention and prevention is more effective than treatment.
Targeted Treatment Approaches:
Preschool programs focusing on parental education and child stimulation.
School-aged programs involve parenting education, social skills training, and family therapy.
Adolescent-focused interventions incorporate individual therapy, conflict resolution, anger management, and social skills training.
Focus on supporting the development of emotional regulation and coping strategies to help children manage their behavior effectively.
Pharmacological Approach:
Limited efficacy in managing symptoms; antipsychotics and mood stabilizers may address specific symptoms like aggression.
Antipsychotics (2nd and 3rd generation) for aggression, mood stabilizers for labile moods.
Community-Based Care
Acute care for severe behavior on a short-term stabilization basis, leading to long-term care in community settings such as school and home.
Various community residential placements for children outside the home, including group homes, halfway houses, and residential treatment settings.
Legal Issues: Involvement in detention facilities and safe environments provides structured supervision and support.
Nursing Process Applications for Conduct Disorder
Recognizing and Analyzing Cues
Assessment includes a history of aggression, disturbed relationships, deceitfulness, truancy, and risky behavior.
Psychological Profile:
Mood and affect can range from sullen to openly hostile, with a lack of insight into their consequences.
Self-Concept shows low self-esteem despite a tough appearance.
Prioritization and Planning
Identifying key interventions focusing on no injury, participation in treatment, and promoting age-appropriate behaviors and positive self-statements.
Interventions
Aiming to decrease violence and increase compliance with treatment through structured limit-setting, behavioral contracts, and skill-building exercises.
Mental Health Promotion
Parenting classes designed to alter risky behaviors that are modeled to children, and group-based parenting programs are effective in early intervention.
Importance of early detection and assessment through screening tools like SNAP-IV, DBDRS, and Conners Scale for ADHD.
Ethical Concerns and Self-Awareness
Importance of recognizing personal beliefs and values regarding child behavior and the need for a supportive approach that avoids placing blame.
Attention-Deficit/Hyperactivity Disorder (ADHD)
Overview of ADHD
Characterized by inattentiveness and impulsiveness, most common in males.
Essential features include persistent patterns of inattention and/or hyperactivity and impulsivity.
Affects approximately 9% of school-age children, with 60% experiencing persistent symptoms into adulthood.
Key Characteristics
Inattention.
Hyperactivity.
Impulsivity.
Treatment Approaches
Behavioral interventions.
Medication management.
Onset and Clinical Course of ADHD
Typically diagnosed when a child enters preschool or school, symptoms may be reported earlier by parents.
Infants may be described as fussy and temperamental; distinguishing normal active behavior from hyperactivity can be difficult for parents.
Etiology of ADHD
Understanding Causes
The definitive cause is unknown; a combination of genetic and environmental factors contributes to the risk.
Risk Factors
Family history of ADHD (first- and second-degree relatives are 2 to 8 times more likely to develop ADHD).
Environmental toxins (e.g., lead exposure).
Prenatal influences (e.g., alcohol, tobacco).
Severe malnutrition during early childhood.
Marital or family discord (e.g., divorce, neglect).
Low birth weight and maltreatment or physical abuse.
Treatment Approaches for ADHD
No single treatment option exists; the focus is on managing symptoms and improving functionality.
Goals of Treatment:
Reduce hyperactivity and impulsivity, and increase attention.
Components of ADHD Treatment
Medications (stimulants and non-stimulants).
Behavioral interventions focused on improving attention and reducing hyperactivity.
Educational assistance for academic achievement.
Psychopharmacology for ADHD
Medications Used
Stimulant medications: Methylphenidate (Ritalin) and amphetamine compounds (Adderall).
Ritalin is effective in 70%–80% of children for reducing hyperactivity and improving attention.
Atomoxetine (Strattera) is the first FDA-approved non-stimulant medication for ADHD.
Mechanism of Action
Medications stimulate the release of norepinephrine, dopamine, and serotonin pre-synaptically while blocking their reuptake.
Common Side Effects
Anorexia, weight loss, nausea, irritability, and potential growth suppression.
Patient Teaching
Take doses after meals,
Avoidance of caffeine, sugar, and chocolate,
Ensure proper storage of medications out of children's reach.
Effective Noticing in ADHD Assessment
Utilize assessment strategies including history-taking from parents regarding behavior as an infant and identifying difficulties across multiple life domains, general assessment of motor behavior, mood and affect observation, as well as self-concept and familial relationships.