NMB Reversal
Neuromuscular Blocker Reversal
Definition and Importance
Neuromuscular blocker reversal involves the use of acetylcholinesterase inhibitors to counteract the effects of neuromuscular blockers used in anesthesia.
Acetylcholinesterase Inhibitors
Mechanism of Action
Acetylcholinesterase hydrolyzes acetylcholine into choline and acetate, primarily at the nicotinic receptors at the neuromuscular junction.
Inhibitors include:
Pyridostigmine
Edrophonium
Neostigmine
These inhibitors reversibly block acetylcholinesterase, leading to an increased concentration of acetylcholine at the neuromuscular junction, enhancing competition for alpha binding sites on nicotinic receptors and helping to antagonize the block.
Key Points on Acetylcholinesterase Inhibitors
Higher acetylcholine concentration does not eliminate neuromuscular blockers; they still need to be eliminated despite the increased acetylcholine levels.
To recognize which acetylcholinesterase inhibitors cross the blood-brain barrier, use this mnemonic: "four big pen"
4 = Quaternary amine (e.g., pyridostigmine, Edrophonium, neostigmine) - these cannot cross the blood-brain barrier due to size.
Mechanism of Acetylcholine Concentration Increase
Two main ways acetylcholinesterase inhibitors increase acetylcholine concentration at the nicotinic receptor:
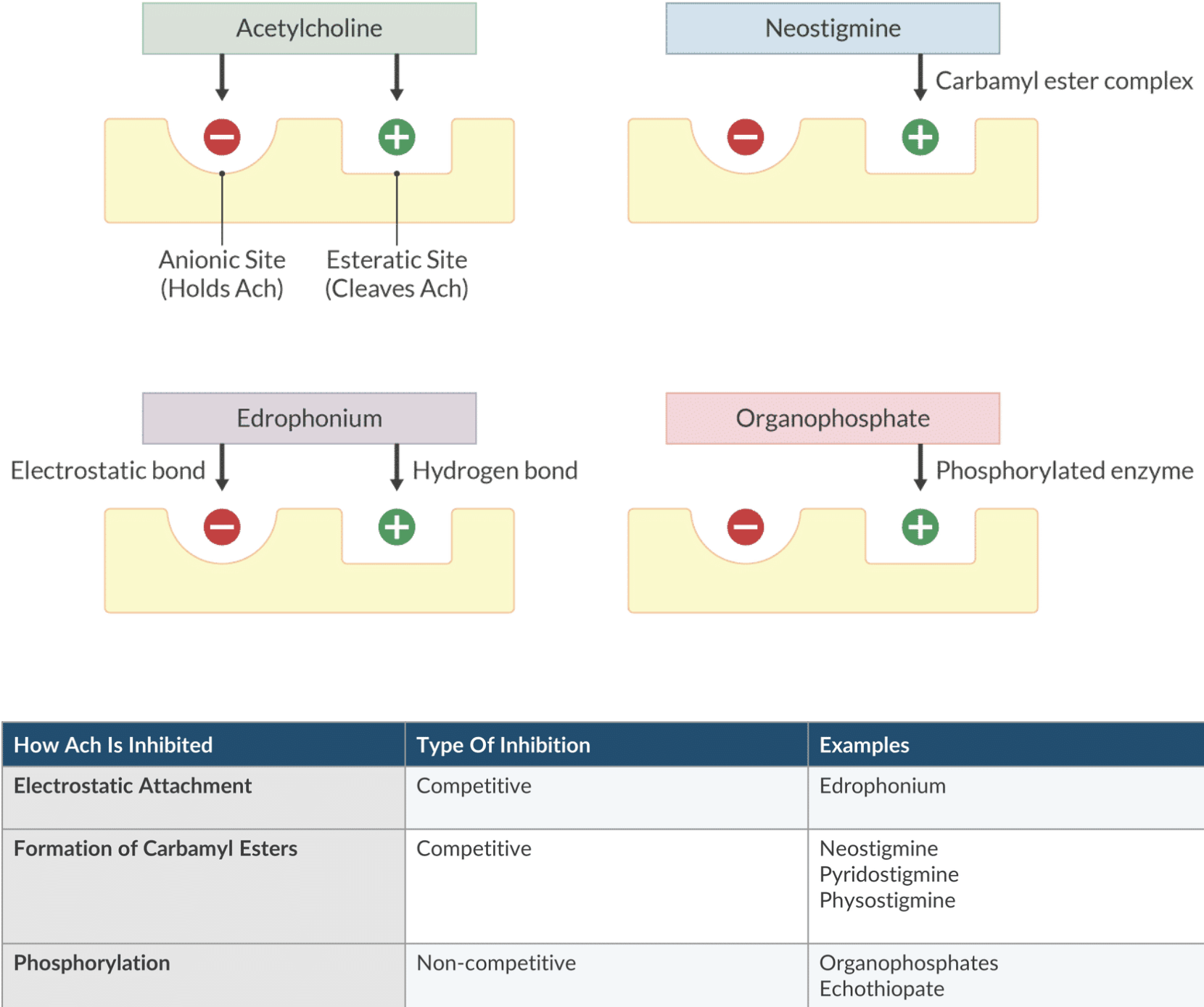
Enzyme Inhibition
Acetylcholinesterase has two binding sites for acetylcholine.
Anionic site (holds Ach) and Esteratic site (cleaves Ach)
Edrophonium competitively inhibits the electrostatic attachments.
Pyridostigmine, Physiostigmine, and neostigmine, they form carbamyl esters, contributing to another competitive inhibition.
Organophosphate and Echothiophate non-competitively inhibits Ach by phosphorylation.
Presynaptic Effects
Acetylcholinesterase inhibitors stimulate presynaptic receptors, causing an increase in released acetylcholine due to a positive feedback loop created from inhibition.
Pharmacokinetics and Pharmacodynamics of Acetylcholinesterase Inhibitors
Combining an anticholinergic drug with acetylcholinesterase inhibitors helps mitigate cholinergic side effects.
Renal failure increases the duration of action for both acetylcholinesterase inhibitors and neuromuscular blockers, but this has a net zero effect; thus, no dose adjustment is needed.
Acetylcholinesterase inhibitors exhibit a ceiling effect; increasing doses does not yield better recovery and can worsen side effects.
Train of four less than 90%:
Increase risk of airway obstruction, hypoxemia, and postoperative pulmonary complications
Caution with inadequate reversal and giving Acetylcholinesterase inhibitors at full recovery because it can cause paradoxical muscle weakness
Due to Too much Ach desensitizes the receptor
Dosing Information
With deeper neuromuscular blockers, there is a longer onset of action for acetylcholinesterase inhibitors.
E.g., neostigmine takes longer for effect with 90% twitch suppression than 50% twitch suppression.
Mixing Acetylcholinesterase inhibitors causes an additive effect, not a synergistic effect.
Neostigmine:
Onset: 5 to 15 minutes
Duration: 45 to 90 minutes
Dosing: 0.02 to 0.07 mg/kg
Best anticholinergic pairing: Glycopyrrolate
Metabolism: 50% renal, 50% liver
Edrophonium:
Dosing: 0.5 to 1 mg/kg
Onset: 1 - 2 min
Duration: 30 to 60 minutes
Best anticholinergic pairing: Atropine
Metabolism: 75% renal, 25% liver
Pyridostigmine:
Dosing: 0.1 to 0.3 mg/kg
Onset: 10 - 20 min
Duration: 60 to 120 minutes
Best anticholinergic pairing: Glycopyrrolate
Metabolism: 75% renal, 25% liver
Clinical Implications in the Operating Room
Intrathecal Neostigmine:
Dosing: 50 to 100 mcg
Effects: Provides analgesia, can cause nausea/vomiting, pruritus, and prolonged sensory/motor block.
Physostigmine:
Dosing: 40 mcg/kg
Uses: Decreases postoperative shivering, comparable in efficacy to meperidine and clonidine.
Cholinergic Side Effects
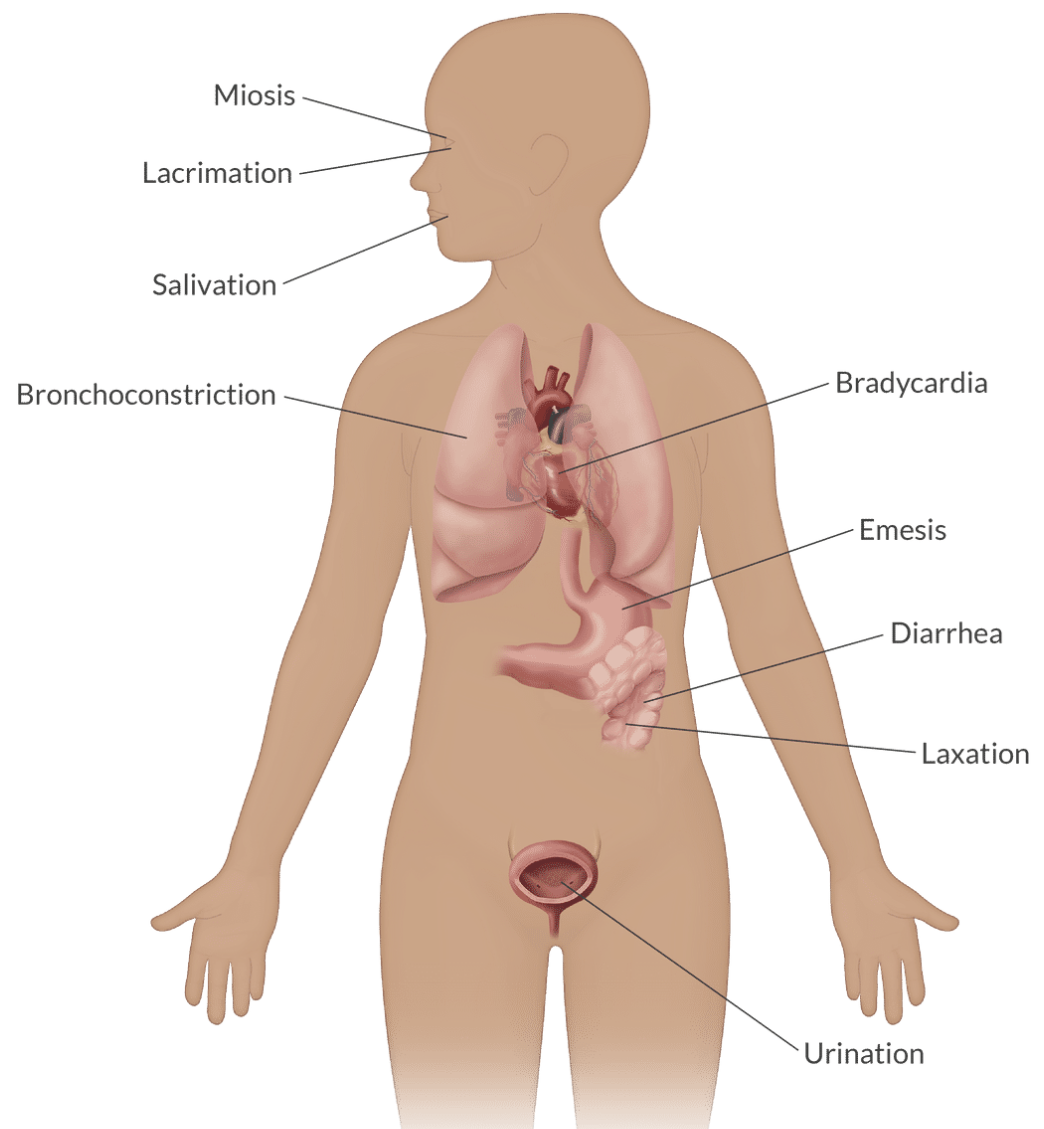
Increased acetylcholine concentration at muscarinic receptors leads to parasympathetic side effects:
Mnemonic: DUMBELLS
Diarrhea
Urination
Myosis (constricted pupils)
Bradycardia
Bronchoconstriction
Emesis
Lacrimation
Laxation
Salivation
Alternative mnemonic: SLUDGE
Salivation
Lacrimation
Urination
Defecation
GI upset
Emesis
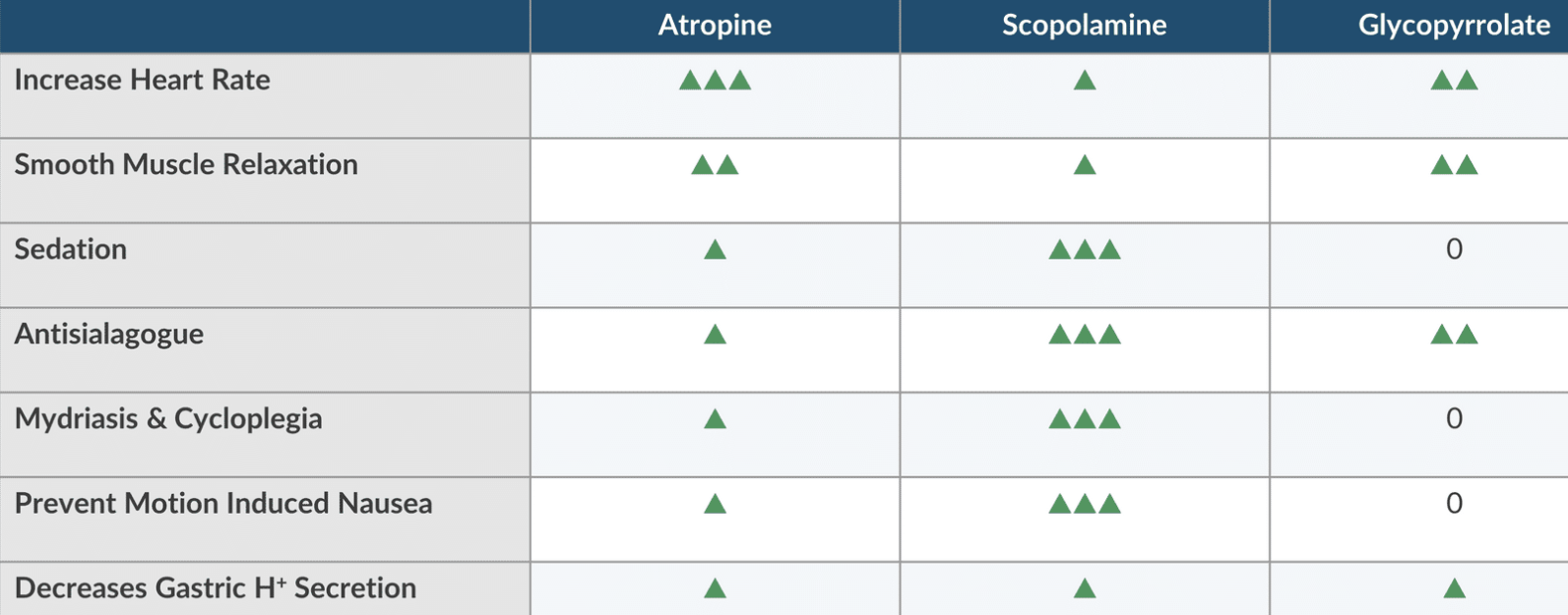
Muscarinic Antagonist Side Effects
Atropine and Scopolamine:
A tertiary amine that is lipophilic and can cross blood-brain barrier causing CNS side effects.
Side effects of atropine: Paradoxical bradycardia from low doses due to inhibition of presynaptic m1 receptors on vagal nerve endings, disrupting negative feedback loops.
Glycopyrrolate:
A quaternary ammonium that does not cross blood-brain barrier, avoiding CNS side effects like sedation.
Cautions
Muscarinic antagonists have no effect on heart rate in heart transplant patients due to denervated hearts—they still experience other cholinergic effects.
They should receive a muscarinic antagonist anyway
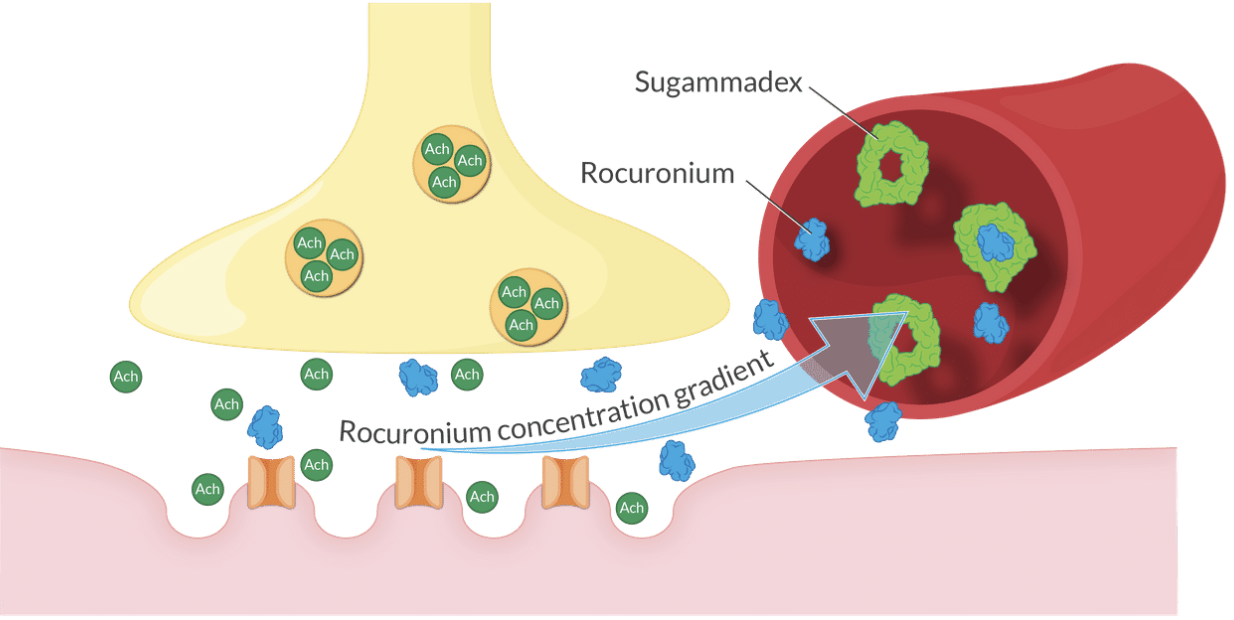
Sugammadex
A selective agent that binds aminosteriodal nondepolarizing neuromuscular blockers (for example: rocuronium > vecuronium > pancuronium).
Mechanism of Action:
A gamma-cyclodextrin composed of eight sugars encircling neuromuscular blockers like a capsule, decreasing the free concentration of the blocker in plasma and fostering transfer from the neuromuscular junction.
The sugammadex-rocuronium complex is excreted unchanged by the kidneys.
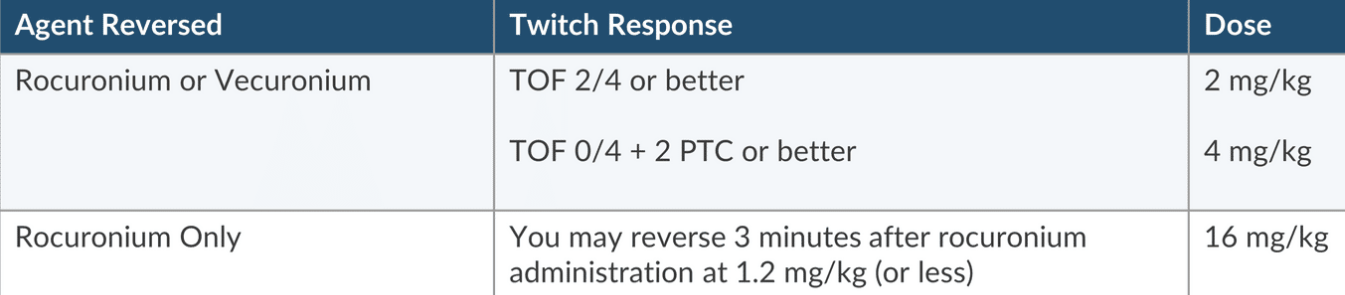
Dosing of Sugammadex
Use actual body weight for dosing to avoid excess residual neuromuscular blockade risk.
Ideal body will increase residual neuromuscular blockers and underside obese patients
Required ratio: 1:1 between sugammadex and neuromuscular blockers.
For a train of four with 2 or more twitches: Dosing: 2 mg/kg
For a train of four with 0 twitches and a posttetenic of 2 or more: Dosing: 4 mg/kg
Rockuronium and vecuronium are appropriate uses for these doses.
16mg/kg of Sugammadex if you need to reverse rocuronium after giving it 3 minutes ago.
Special Considerations
After administering 16 mg/kg of sugammadex, a non-amino steroid blocker such as succinylcholine, atracurium, cisatracurium, or mivacurium must be used if paralysis is needed again.
Less than 4 mg/kg of sugammadex permits repurposing of rocuronium and vecuronium.
Sugammadex can be given from 5 minutes up to 4 hours after the neuromuscular blocker.
For administration beyond 4 hours, rocuronium (0.6 mg/kg) or vecuronium (0.1 mg/kg) can be given.
Adverse Reactions
Anaphylaxis incidence is low (0.3%).
Reported side effects include bradycardia and cardiac arrest where an anticholinergic may be beneficial.
Sugammadex decreases the effectiveness of hormonal contraceptives for 7 days; thus, females should use a backup method during this period.
Benefits of Sugammadex
Improves safety by:
Allowing the use of rocuronium for difficult intubations without the risks associated with succinylcholine.
Enabling reversal of dense neuromuscular block at any point post-administration of the blocker without timing concerns.