Abnormal Colour Vision
Abnormal Colour Vision: Comprehensive Notes
Colour Vision (CV) and Abnormal Colour Vision (Abnormal CV)
Abnormal CV characterized by:
Abnormal colour matching
Colour confusions
Reduced number of colours that can be distinguished compared to those with normal CV
Causes and Types of Abnormal Colour Vision
Abnormal CV can be due to:
Congenital conditions: inherited genetic defects affecting photoreceptor pigments
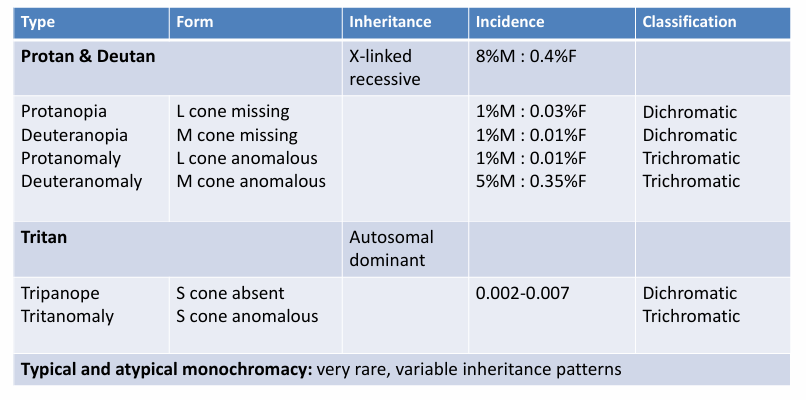
Red/Green (R/G) defects: X-linked recessive
Blue/Yellow (B/Y) defects: Autosomal dominant
Monochromats: X-linked or autosomal recessive
Acquired conditions: altered CV perception secondary to eye disease
Retinal, optic nerve, or visual pathway conditions
Often with other visual function changes
Less predictable pattern of loss
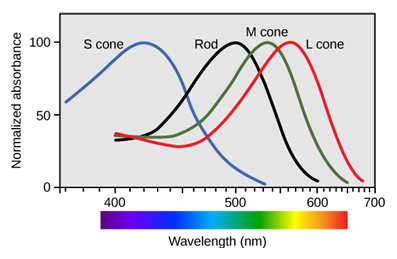
Cone Photo-pigments and Colour Differentiation
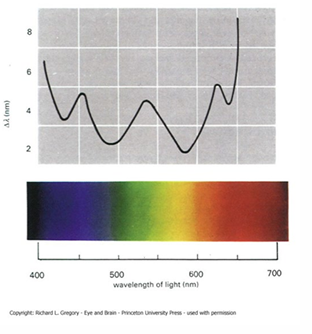
3 cone photo-pigments enable differentiation of all wavelengths in the visible spectrum
If normal function, can discriminate around variation in wavelength
2 cone photo-pigments differentiate some but not all wavelengths
Results in limited colour vision; some colours perceived as identical
1 cone photo-pigment leads to no colour differentiation; brightness differences used for discrimination; effectively colour blind
Terminology: Cone Function and Colour Vision Defects
Status of cone functioning:
Normal trichromat: three cones function normally
Anomalous trichromacy / anomalous trichromat: abnormal sensitivity in one cone
Dichromacy / dichromat: absence of one cone, leaving two functioning cones
Typically avoid the term “colour blind”
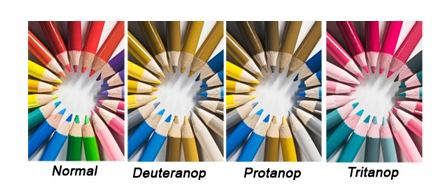
Affected cone pigments:
Protan: L-cone affected
Deutan: M-cone affected
Tritan: S-cone affected
Congenital Colour Vision Defects (R/G and B/Y)
Congenital red/green defects:
Deutan (M cone affected)
Deuteranomaly
Deuteranopia
Protan (L cone affected)
Protanomaly
Protanopia
Congenital blue/yellow defects:
Tritan (S cone affected)
Tritanomaly (rare)
Tritanopia
Colour Matching and Judgement
Normal trichromats (CV normal): can match any reference wavelength with 3 appropriate spectral wavelengths
Anomalous trichromats: can match any reference wavelength with 3 spectral wavelengths but in different proportions from normals
Dichromats: can match any reference wavelength using two other appropriately chosen wavelengths
Monochromats: can match any reference wavelength using any one other selected wavelength; matched on brightness
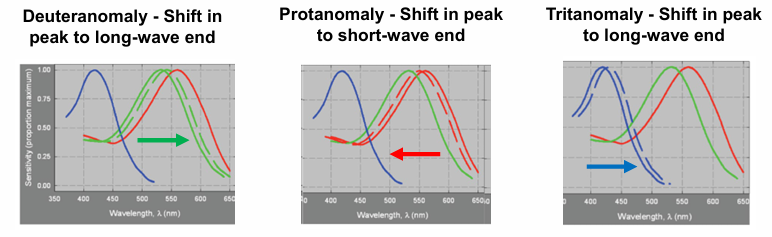
Anomalous Trichromacy: Abnormal Absorption and Shifts
Abnormal absorption spectrum for the affected cone photopigment
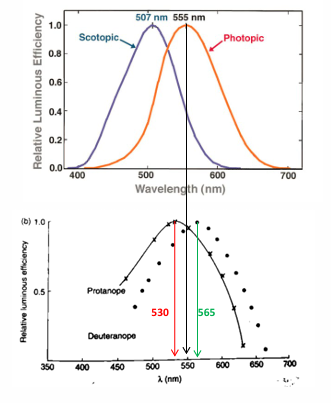
Shifting of the relative luminous efficiency curves
Specific shifts:
Deuteranomaly: peak shift toward the long-wave end
Tritanomaly: peak shift toward the long-wave end
Protanomaly: peak shift toward the short-wave end
Anomalous Trichromacy: Range and Performance
Three primaries can match many colours; but the proportions differ from normal trichromats
Range of severity:
Mild: close to normal functioning
Moderate: intermediate functioning but may be colour unsafe for various tasks
Severe: close to dichromatic functioning
Performance tends to be worse with:
Desaturated colours
Low luminance
Small targets
Fatigue
Dichromacy (Absence of One Cone Type)
Types:
Deuteranopia: M-cone absent
Protanopia: L-cone absent
Tritanopia (rare): S-cone absent
Can match all colours with 2 primaries
Severity terminology is not appropriate; all types perform similarly to each other
Characteristics of Red/Green Defects
Relative luminous efficiency: normal peak around ~555nm
Protan: peak shifts to shorter wavelengths ~530nm, reduced long-wavelength sensitivity
Deutan: peak shifts to longer wavelengths~565 nm
Anomalous trichromats have peaks between normal and dichromatic values.
Protan – peak shifts towards short wavelengths
Deutan – peak shifts towards long wavelengths
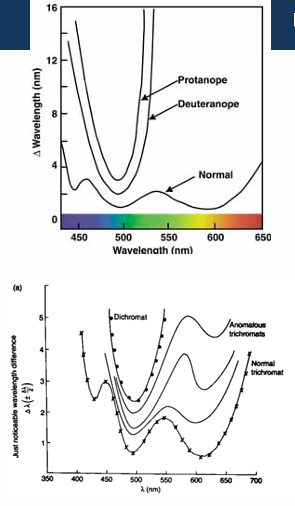
Hue discrimination: optimum around ~495 nm; similar for protanopes and deuteranopes
above 540nm, colour distinction reduces
anomalous trichromats vary
Saturation discrimination: dichromats have a neutral point where a spectrum is indistinguishable from white
Protanopes ~490nm
Deuteranopes ~500nm
poorest saturation in the blue-green end of the spectrum– Need to add much more colour to white before it looks different from white
Anomalous trichromats have similar saturation discrimination to dichromats but no neutral point

Neutral points appear grey/achromatic at specific wavelengths (spectrum points)
Confusion lines on a chromaticity diagram: colours along a confusion line appear the same
A line through white intersecting the spectral locus defines a point that appears achromatic
Neutral points:
~490nm Protanopes
~ 500 nm Deuteranope

Anomalous Trichromats: Confusion Zones
Confusion zones vary in length depending on how far the abnormal pigment shifts the spectral sensitivity
Confusion zones may be almost as long as dichromats (severe anomalous trichromats) or not far off normal colour vision (mild anomalous trichromat)
Specific Defects: Deuteranomaly and Deuteranopia
Deuteranomaly:
Production of abnormal opsin pigments for the M-cone; genetic abnormality on the X chromosome
Prevalence: males, females
Practical implications depend on degree affected:
M-cone absorption curve shifted; diminished discrimination above
Best discrimination around (blue/green)
May confuse reds, yellows, and greens; blue/green with grey and red/purple
Mild: may be colour safe and pass some vocational tests
Moderate/severe: likely colour unsafe (closer to deuteranopia levels)
Deuteranopia:
Absence of M-cones; genetic abnormality on X chromosome
Prevalence: males, females
Practical implications invariant: M-cone absent; no long-wavelength discrimination above ; best around
Will confuse reds, yellows, greens; blue/green with grey and red/purple; brightness cues also matter
Protanomaly and Protanopia
Protanomaly:
Abnormal opsin pigments for the L-cone; X-linked
Prevalence: males, females
L-cone absorption curve shifted; variable loss above ; best discrimination around
May confuse reds, yellows, greens; red & blue/green with grey; blue with purple
May have reduced sensitivity to red light
Mild: less likely to pass vocational tests than mild DA
Moderate/severe: colour unsafe; may be close to protanopic function
Protanopia:
Absence of L-cones; X-linked
Prevalence: males, females
Invariant practical implications: no L-cone function; no long-wavelength discrimination above ; best around
Will confuse reds, yellows, greens; red & blue/green with grey; blue with purple; reduced sensitivity to red light
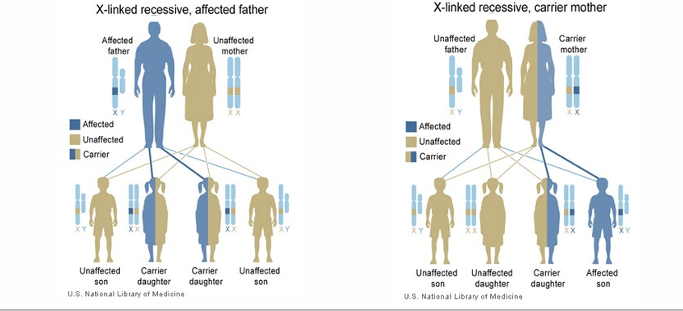
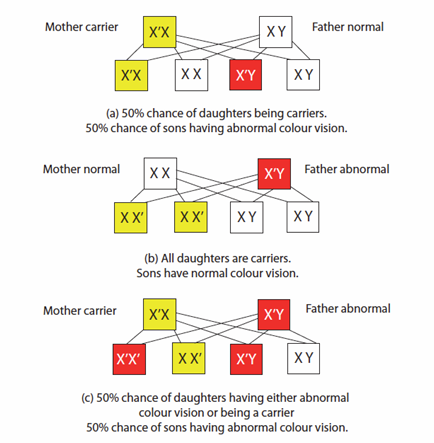
Inheritance of Red/Green Defects
L and M cones are encoded on the X-chromosome; defects are recessive
Expression tends to be in males with a single defective X chromosome; females may be carriers if only one defective X is present
Carrier concepts and cross outcomes (simplified representations):
(a) Mother carrier (X'X), Father normal (X Y): 50% daughters carriers; 50% sons abnormal
(b) Mother normal (XX), Father abnormal (X'Y): all daughters carriers; sons normal
(c) Mother carrier, Father abnormal: 50% daughters abnormal or carriers; 50% sons abnormal
Tritan Defects: Blue/Yellow Defects
Tritanopia (S-cone absent): Prevalence ~1 in 10,000; Autosomal dominant
Reduced ability to see colours; confuses blue with green and purple; yellow with grey
Not colour safe; may fail some occupational tests
Tritanomaly (incomplete Tritan): Prevalence unclear (~1 in 500?); S-cone shifted or partially absent
May be colour safe; may pass more occupational tests; R/G connotative codes more common than B/Y
Characteristics:
Relative luminous efficiency: no peak shift, but reduced sensitivity at short wavelength end
Hue discrimination: Tritanopes cannot detect wavelength differences between
Tritanomalous: reduced colour discrimination in this range

Confusion lines and neutral points:
Confusion lines on a chromaticity diagram: colours on a line appear the same (perceived as grey / achromatic)
Neutral point occurs at approximately for Tritanopes

Inheritance: Autosomal dominant; one defective gene expresses deficiency
a parent with the defect passes the gene to 50% of offspring regardless of gender
Monochromatism (Inherited Achromatopsia)
Monochromats cannot distinguish wavelength differences in photopic illumination
They can match all spectral hues using a single spectral wavelength
Rod monochromatism (typical, complete):
Normal rod function only; absence of cone photoreceptors
Scotopic function only
Autosomal recessive inheritance
Both parents with same genetic abnormality, 25% of children are affected
Predisposing factor: consanguinity (inter-related marriage)
Prevalence ~ 1 in 35,0000006/606/18$$); moderate photophobia; low-grade nystagmus
ERG may be abnormal
Some colour perception possible in mesopic conditions
Both S-cones and rods active, but no colour perception in photopic or scotopic conditions
Summary of Inheritance and Incidence
Treating Congenital Colour Vision Defects
short answer is “no” - alex black
Selective wavelength transmission filters may help some individuals
May assist passing a CV test but likely shifts rather than removes colour confusions
May reduce luminance; avoid for critical tasks (e.g., night driving)
X-chrom, Chromagen and ColourMax lenses: marketed for selective wavelength filtering
Evidence does NOT support their efficacy
Beware of stereo disadvantage and Pulfrich effect during use
Ensure coloured contact lenses or other wavelength filters are NOT used during a CV assessment
Potential gene therapy may exist in the future
Acquired Colour Vision Deficiencies
Abnormal CV can be secondary to disease or injury along the visual pathway from retina to cortex
May be associated with systemic or CNS diseases or medication use
Variable severity and progression; may outlast the underlying condition after treatment
Presentation is less specific; classification not straightforward
May present with monocular differences (asymmetric CV defect)
Clinical Associations and Rules
May be accompanied by reduced visual acuity (VA), visual field (VF) defects, and/or relative afferent pupillary defect (RAPD)
Impaired dark adaptation, abnormal ERG responses, flicker sensitivity changes
Kollner’s rule (general associations):
Blue/Yellow (B/Y) defects: outer retinal and media changes
Red/Green (R/G) defects: inner retina, optic nerve, visual pathway and cortex involvement
Exceptions exist (e.g., glaucoma—early B/Y defects possible)
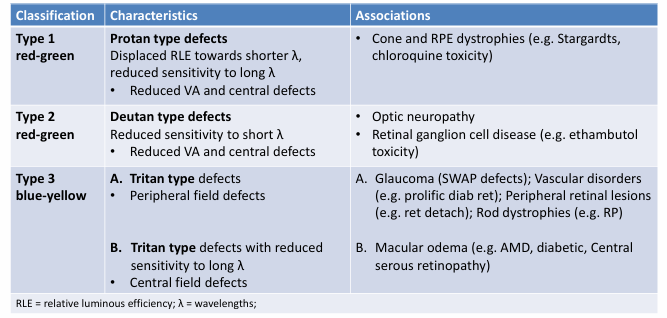
Classification of Acquired CV Deficiencies
Type 1: Red-green Protan type defects
Symptoms: displaced relative luminous efficiency toward shorter wavelengths; reduced long-wavelength sensitivity
Associated with cone and RPE dystrophies (e.g., Stargardt disease, chloroquine toxicity)
Type 2: Red-green Deutan type defects
Symptoms: reduced sensitivity to short wavelengths
Associated with optic neuropathy and retinal ganglion cell disease (e.g., ethambutol toxicity)
Type 3: Blue-yellow defects
A. Tritan type defects: peripheral field defects
B. Tritan type defects with reduced sensitivity to long wavelengths: central field defects
Associations: glaucoma (SWAP defects); vascular disorders (e.g., proliferative diabetic retinopathy); peripheral retinal lesions (retinal detachment); rod dystrophies (RP); macular edema (AMD, diabetic macular edema, central serous retinopathy)
RLE = relative luminous efficiency; λ = wavelengths
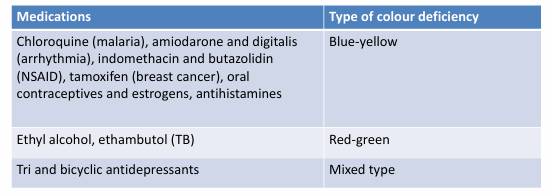
Medications Known to Affect Colour Vision
Not exhaustive list; examples include:
Chloroquine, amiodarone, digitalis: Blue-yellow defects
Ethambutol (TB) and others: Red-green defects
Indomethacin, butazolidin (NSAIDs); tamoxifen; oral contraceptives and estrogens; antihistamines: various effects
Tri- and bicyclic antidepressants: mixed defect types
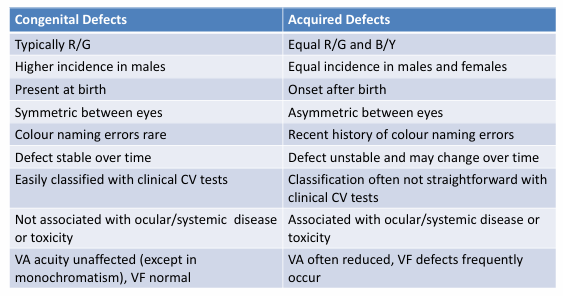
Summary: Congenital vs Acquired Colour Vision Defects
Congenital defects:
Typically R/G defects
Higher incidence in males
Present at birth
Symmetric between eyes
Colour naming errors are rare
Defect generally stable over time
Acquired defects:
Equal incidence in males and females
Onset after birth
Often asymmetric between eyes
Colour naming errors may be present
Defect may be unstable and change over time