Week 6: Mood Disorders and Depression
Chapter 17: Mood Disorders: Depression
Introduction
Overview of Mood Disorders:
Everyone experiences occasional sadness and low energy.
Symptoms include:
Anergia: a state of profound lethargy or lack of energy, often seen in individuals with depressive disorders.
Exhaustion
Agitation
Noise intolerance
Slow thinking
Mood fluctuations are normal, typically temporary.
Sadness can be a response to misfortune or loss; elated moods occur but are short-lived.
Mood Disorders:
Involves pervasive alterations in emotions.
Manifested by:
Depression
Mania
Both can interfere with life activities, self-esteem, occupation, and relationships.
Historical context:
Ancient treatments and beliefs about mood disturbances.
Modern understanding and treatment: Effective treatments for depression and mania are available.
Medications weren’t developed until the 1950s.
Mood disorders are the most common psychiatric diagnoses associated with suicide.
General Concepts
Mood: Pervasive, sustained emotion that impacts a person's perception of the world (internal).
Affect: Emotional reaction associated with an experience (external).
Depression: Alteration in mood expressed as feelings of sadness, despair, and pessimism.
Loss of interest in usual activities, somatic symptoms.
Changes in appetite and sleep patterns (sleep more or less).
Pessimism: glass half empty.
Despair: hopelessness and helplessness.
Mood Disorders:
The most common psychiatric diagnosis associated with suicide.
Depression is a significant risk factor.
Anergia
Anergia:
Lack of energy affects daily routines.
Impacts how someone functions.
Work, family, and social responsibilities continue despite low mood.
Low periods usually pass within days.
Everyday use of "depressed" vs clinical depression:
Common to state “I'm depressed” during bad days.
Clinical depression involves more severe and persistent symptoms.
Mood responses to life events:
Grief from loss or misfortune is normal.
Elated moods can occur, but typically return to average.
Comparison:
Mood disorders cause drastic, long-term emotional changes accompanied by self-doubt, guilt, and anger.
Historical Context and Notable Figures
Historical Treatments:
Ancient practices: drilling holes in skulls to relieve "evil humors"; beliefs in divine causes of extreme behavior.
Notable Historical Figures:
Mood disorders in:
King Saul, King Nebuchadnezzar, Moses.
Abraham Lincoln, Queen Victoria.
Famous artists/writers: Virginia Woolf, Sylvia Plath, Eugene O’Neill, George Frideric Handel, Vincent van Gogh.
Contemporary Celebrities with Mood Disorders:
Dwayne Johnson, Lady Gaga, Demi Lovato, Michael Phelps, Bebe Rexha.
Evolution of Treatment:
No effective treatments existed until mid-1950s.
Modern treatments for depression and mania now available.
Modern Understanding and Treatment
Impact of Mood Disorders:
Mood disorders interfere with self-esteem, occupation, and relationships.
Causes long-term sadness, agitation, or elation.
Suicide Risk:
Mood disorders are the most common psychiatric diagnoses associated with suicide; depression is a significant risk factor.
Focus Areas:
Major depression, bipolar disorder, suicide, and increased suicide risk in other disorders (e.g., schizophrenia, substance use).
Importance of Understanding:
Effective treatments improve quality of life.
Awareness and intervention can reduce suicide risk.
Categories of Mood Disorders
Major Depressive Disorder (MDD):
Lasts at least 2 weeks or more.
Symptoms include:
Depressed mood
Loss of pleasure in activities: surrounding people may notice this and point it out to you.
Changes in eating habits
Hypersomnia or insomnia
Impaired concentration
Feelings of worthlessness
Thoughts of death or suicide
Fatigue
Rumination: the process of continuously thinking about the same thoughts, often negative.
Which can exacerbate feelings of hopelessness and contribute to the severity of depressive symptoms.
And contribute to a lack of sleep.
Significant distress or impairment in functioning.
10% to 20% experience psychotic features.
Bipolar Disorder:
Divided into bipolar I and bipolar II.
Dysthymic Disorder (Persistent Depressive Disorder):
Chronic, long-term form of depression.
Disruptive Mood Dysregulation Disorder:
Severe temper outbursts and temper issues.
Cyclothymic Disorder:
Mild mood swings between hypomania and depression; no loss of social or occupational functioning.
Related Disorders
Substance-Induced Depressive or Bipolar Disorder:
Mood disturbance due to ingested substances (e.g., alcohol, drugs, toxins).
Mood altering subtance that can cause permanent brain damage or short-term alterations.
Seasonal Affective Disorder (SAD):
Two subtypes:
Winter depression (fall-onset):
Symptoms: increased sleep, appetite, carbohydrate cravings, weight gain, irritability.
Spring/summer-onset:
Symptoms: insomnia, weight loss, poor appetite.
This may trigger more suicidal ideation due to life not getting better with the better weather.
Treatment: Light therapy.
Nonsuicidal Self-Injury:
Deliberate, intentional self-harm (e.g., cutting, burning).
Reasons may include: alleviation of negative emotions, self-punishment, and seeking attention.
Related Disorders (Hormonal)
Postpartum or Maternity Blues:
Mild, predictable mood disturbance; symptoms subside without treatment.
Big hormonal disturbances.
Postpartum Depression:
The most common complication of pregnancy is symptoms consistent with depression.
Huge drop in hormones.
Onset within 4 weeks of delivery; treated with Brexanolone (Zulresso).
Postpartum Psychosis:
Severe psychiatric illness requiring immediate treatment; symptoms include fatigue, emotional lability, delusions, and hallucinations.
This is an emergency!
Homicidal tendencies.
Premenstrual Dysphoric Disorder:
Affects 5% to 8% of premenopausal individuals; severe premenstrual syndrome symptoms leading to significant dysfunction in daily activities.
Symptoms: labile mood, irritability, increased interpersonal conflict, difficulty concentrating, feeling overwhelmed, anxiety, and tension.
Etiology of Mood Disorders
Overview:
Various theories exist for the etiology of mood disorders.
Genetics and biological imbalances are influenced by psychosocial stressors.
May be a generic factor in families.
Interpersonal events can trigger physiological changes in the brain.
Effective treatment should address both biological and psychosocial components.
Biological Theories: Genetic Theories
Genetic studies indicate transmission of major depression:
Increased risk (two to three times) if a parent or sibling has major depression.
Twin studies show the heritability of depression is 40% to 50%.
Concordance rate for monozygotic twins is not 100%, indicating the role of environmental factors and not solely genetics.
How genes interact with environmental factors remains a key area of research, as it may reveal why some individuals with a genetic predisposition do not develop depression.
Genetic overlap with bipolar disorder and alcohol use disorder is noted.
Neurochemical Theories
Focus on serotonin and norepinephrine neurotransmitters:
Serotonin Functions: Regulates mood, aggressiveness, cognition, and pain.
Also affects appetite, sexual behavior, and sleep patterns.
Norepinephrine: Deficiency linked to depression.
The interaction of genetic and environmental factors can disrupt neurochemical functions.
Neuroendocrine Influences
Examines hormonal fluctuations related to depression:
Elevated glucocorticoid activity associated with the stress response from increased cortisol levels and inflammation is noted in depressed individuals.
Hypothyroidism is noted as a risk factor for depression, often treatment-resistant.
Ensure that the cause of depression isn’t biological, relating to hypothyroidism or a tumor in the brain.
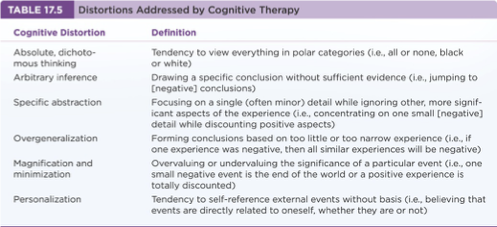
Psychodynamic Theories
Many theories have focused on the individual’s family and self-depreciation as it relates to depression:
Depression is a reaction to distressing life experiences, leading to learned helplessness and specific cognitive distortions as per Beck's cognitive model.
Example: A person who has dealt with behaviors as a child and thus, that person may be used to that behavior as they grow older and not recognize its negative impact on their mental health, often internalizing feelings of worthlessness and inadequacy in adulthood.
Cultural Considerations
Hamilton Rating Scale for Depression (HRSD):
Considered a gold standard measure of depression.
Symptoms assessed include mood, guilt, loss of interest, retardation, and suicidal thoughts.
Somatic symptoms can vary among cultures; physical ailments may accompany depression.
Major Depressive Disorder (MDD)
Characterized by a sad mood or loss of interest lasting 2 weeks plus at least four symptoms from the following:
Anhedonia (lack of pleasure)
Changes in sleep, weight, and energy
Impaired concentration and decision-making
Feelings of worthlessness; thoughts of death or suicide
Fatigue and rumination
Prevalence: twice as common in females.
History includes a higher incidence among first-degree relatives (1.5-3 times) with a mean onset age of 40 years.
Episodes can last weeks to months and are usually untreated.
Nursing Process in Mood Disorders
Assessment: Recognizing cues related to the patient's depression.
Analysis: Prioritizing relevant data for outcome identification.
Planning: Generating solutions and monitoring outcomes.
Implementation: Taking actions, such as safety precautions and promoting therapeutic relationships.
Evaluation: Checking the effectiveness of interventions, including medication compliance and self-reported outcomes.
Treatment and Psychopharmacy Overview
Types of antidepressants:
Cyclic antidepressants, MAOIs, SSRIs, Atypical antidepressants.
Medication therapy is recommended to continue longer than 6 months after depressive symptoms improve.
Beware of off-label uses and black box warnings (risk of serious side effects).
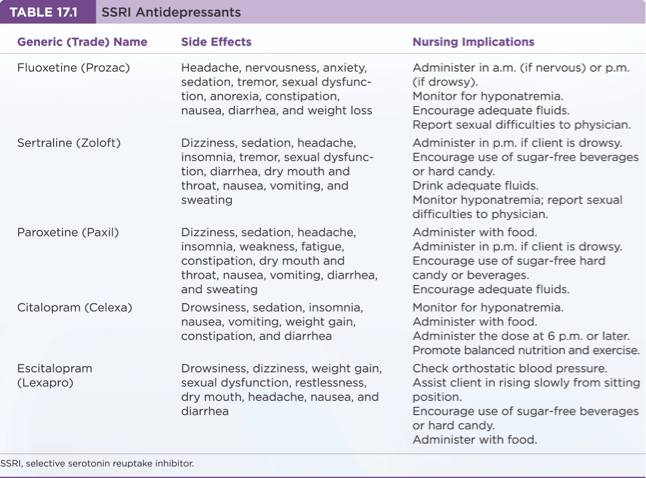
Treatment and Psychopharmacy: SSRIs
SSRIs: First-line treatment; usually administered in the morning.
Known side effects: anxiety, agitation, insomnia, and sexual dysfunction.
Risk of serotonin syndrome when combined with other medications.
Head (hyperthermia) Master (myoclones) (autonomic instability/not being able to manage BP or HR) (shock) (tremors) (encepalopothy) (rigidity/hyperreflexia).
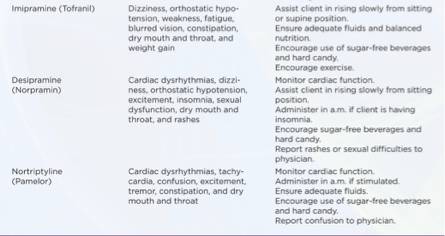
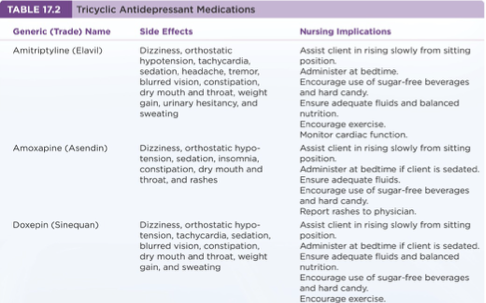
Treatment and Psychopharmacy: Cyclic Antidepressants
Administer cyclically within a few hours of missed doses.
Cyclic within 3 hours of missed dose or omit the day’s dose.
Known for anticholinergic effects, orthostatic hypotension, sedation, and other side effects.
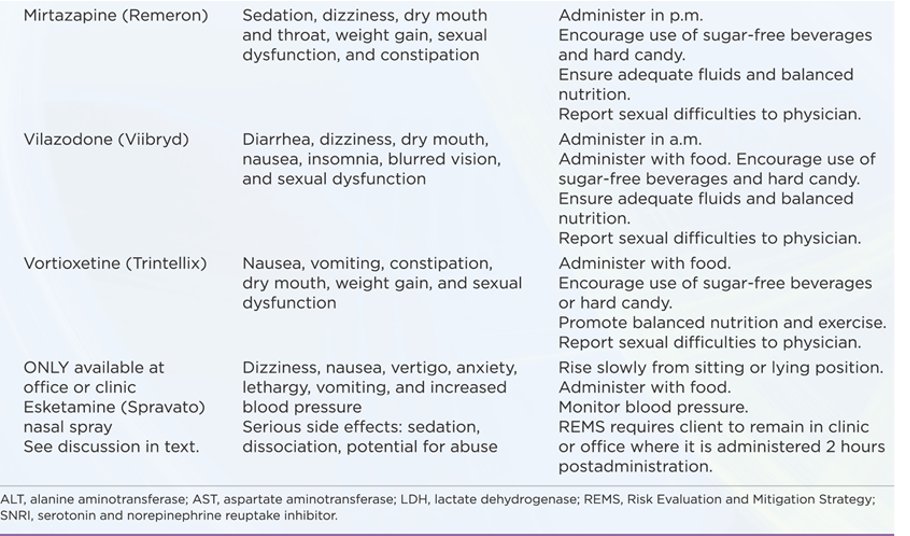
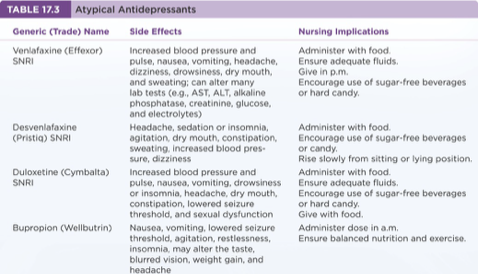
Treatment and Psychopharmacy: Atypicals
Generic (Trade) Name | Classification | Side Effects | Nursing Implications |
|---|---|---|---|
Venlafaxine (Effexor) | SNRI | Increased blood pressure, nausea, and dizziness | Administer with food. |
Duloxetine (Cymbalta) | SNRI | Weight gain; headache | Administer with food. |
Bupropion (Wellbutrin) | NDRI | Lowered seizure threshold; agitation | Administer in the morning with food. |
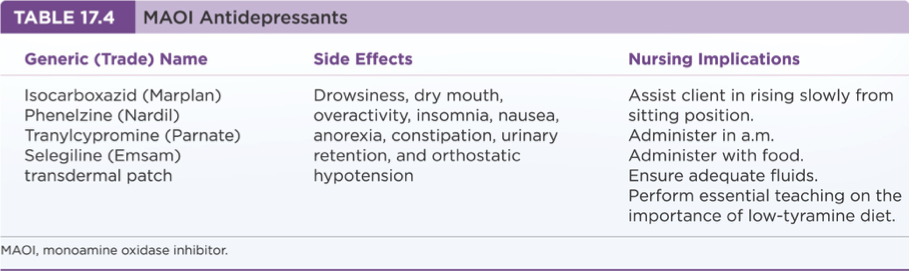
Treatment and Psychopharmacy: MAOIs
Known side effects include daytime sedation, weight gain, and risk of hypertensive crisis with certain foods (tyramine).
Additional Therapy Options
Electroconvulsive Therapy (ECT): For non-responsive cases or active suicidality, typically 6 to 15 sessions are required.
Psychotherapies: Interpersonal, behavioral, cognitive therapies, and brain stimulation methods such as TMS or VNS.
Community-Based Care
Nurses often first recognize symptomatic behaviors of mood disorders.
Treatment should be multidisciplinary and tailored to meet social determinants of health.
Mental Health Promotion
Prevention programs focus on increasing self-esteem and reducing hopelessness.
Collaboration between care providers enhances effectiveness, improving outcomes.