3. Paralytic/Incomitant Strabismus: Common Causes
Third Nerve (Oculomotor) Paresis
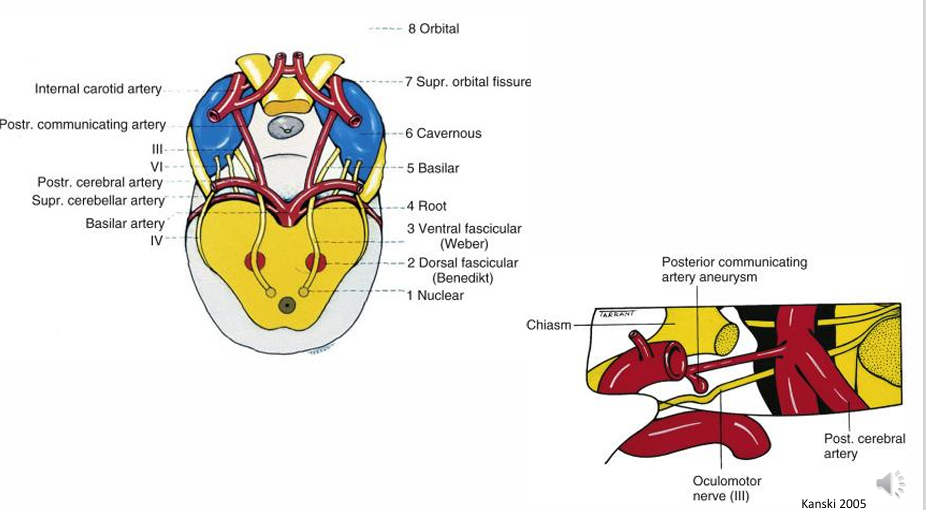
Potential Causes
Vascular disease:
Aneurysm, especially affecting the posterior communicating artery
Ischemia (e.g., due to atherosclerosis, diabetes).
Mass:
Pituitary tumour.
Sphenoid wing meningiomas.
Trauma: Severe head injuries.
Ophthalmoplegic migraine.
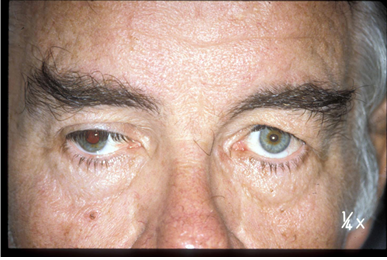
Clinical Signs and Symptoms
Pupil: Dilated and fixed (due to involvement of the iris sphincter muscle, innervated by the IIIrd nerve).
Ptosis: Drooping of the eyelid (due to paresis of the levator palpebrae superioris muscle).
Eye Deviation: Depressed and diverged (outward and downward) due to unopposed action of the Lateral Rectus (LR) and Superior Oblique (SO) muscles, which are not innervated by the IIIrd nerve.
Diplopia:
If partial IIIrd nerve involvement, diplopia may be horizontal, vertical, or oblique.
typically oblique
Partial IIIrd nerve paresis can affect any of the muscles innervated by it, to varying degrees and in any combination.
Could result in any deviation except esotropia.
Blurred Vision: Possible due to ciliary muscle paresis and mydriasis (pupil dilation).
Critical Clinical Considerations
ACUTE PAINFUL ONSET = ANEURYSM:
This is a severe warning sign. An expanding aneurysm can be fatal within hours of the onset of diplopia. Any acute onset IIIrd nerve palsy is an urgent ophthalmic emergency and requires rapid referral.
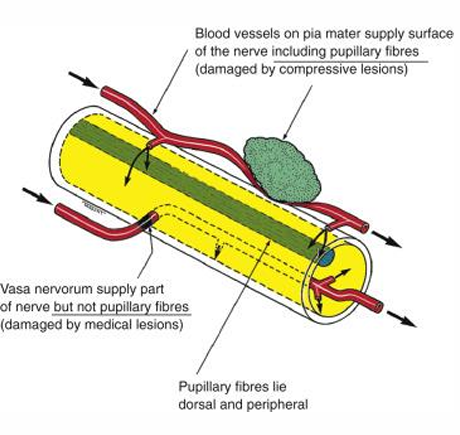
Pupil Involvement and Aetiology:
Aneurysms and compressive lesions generally tend to cause pupil involvement in IIIrd nerve paresis.
Medical conditions (e.g., ischemia due to atherosclerosis, diabetes) typically lead to a pupil-sparing IIIrd nerve palsy.
However, aneurysms may be pupil-sparing early in their evolution, making initial differentiation challenging.
Actionable Advice: ALL patients with acute IIIrd nerve palsies (whether partial or complete) require URGENT REFERRAL FOR NEURO-IMAGING.
Case Example: Partial IIIrd Nerve Paresis Affecting the Superior Division
Patient Profile: A -year-old Chinese female.
Onset: Noticed vertical diplopia and right eyelid droop on waking Christmas morning.
Initial Presentation: Attended PAH on Boxing Day; CT scan showed no abnormalities, discharged the next day.

Follow-up (one month later):
Diplopia had not improved; worse when looking up, especially up and right.
Visual Acuity (VA): Right , Left .
Significant right ptosis.
Adduction and abduction of the right eye were normal.
A right hypotropia was observed.
Elevation of the right eye was deficient, particularly in up and right gaze (impairment of Right Superior Rectus - RSR).
partial paresis
Pupils were equal, round, and normally reacting; no Relative Afferent Pupillary Defect (RAPD).
Amplitudes of accommodation normal and equal
ciliary and sphincter muscle working normally.
no internal ophthalmoplegia.
Corneal sensitivity normal.
Conclusion: This presentation is consistent with a partial IIIrd nerve palsy, specifically affecting the superior division of the oculomotor nerve, which innervates the superior rectus and levator palpebrae superioris.
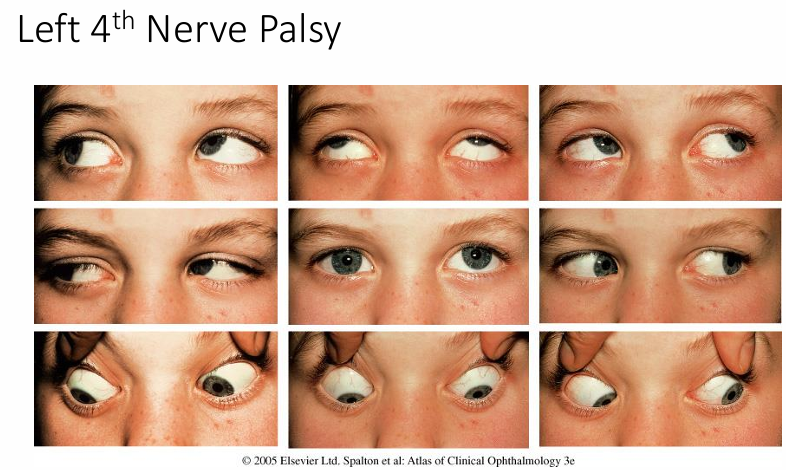
Fourth Nerve (Trochlear) Paresis
Likely the most common nerve palsy to present to optometrists.
Causes
Congenital: Relatively common.
Acquired:
Trauma: Most common acquired cause, especially severe head trauma (can be unilateral or bilateral).
Ischemic: Due to atherosclerosis, diabetes, hypertension (usually unilateral).
Compressive and Inflammatory causes: More rare.
Clinical Signs and Symptoms
Diplopia: Vertical or oblique.
Bilateral IVth nerve paresis often leads to torsional diplopia.
Worse at near (e.g., reading). - down and in (SO muscle)
Worse on ipsilateral head tilt.
Hypertropia: Of the affected side. Looks higher as IO over acts.
Secondary Overaction: Ipsilateral inferior oblique muscle (leading to an "upshoot" of the eye in adduction).
Extorsion: Of the fundus on the affected side may be observed.
Head Tilt: To the sound (unaffected) side.
Bielchowsky Head Tilt Test: Tilting the head to the affected side may cause the involved eye to elevate (increased hypertropia). This is a key diagnostic sign

Features of Fourth Nerve Palsies (Table 18.7, Spalton et al. 2005)
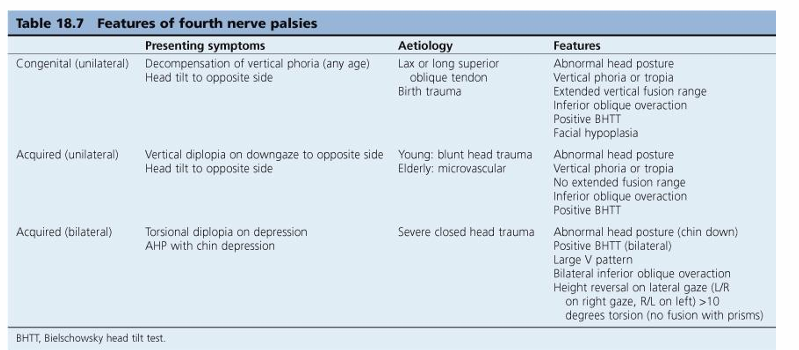
Congenital (Unilateral):
Presenting Symptoms: Decompensation of a vertical phoria (at any age), head tilt to the opposite side.
Aetiology: Lax or long superior oblique tendon, birth trauma.
Features: Abnormal head posture, vertical phoria or tropia, extended vertical fusion range, inferior oblique overaction, positive BHTT, facial hypoplasia.
Acquired (Unilateral):
Presenting Symptoms: Vertical diplopia on downgaze to the opposite side, head tilt to the opposite side.
Aetiology: Young patients: blunt head trauma. Elderly patients: microvascular disease.
Features: Abnormal head posture, vertical phoria or tropia, no extended vertical fusion range, inferior oblique overaction, positive BHTT.
Acquired (Bilateral):
Presenting Symptoms: Torsional diplopia on depression, abnormal head posture (AHP) with chin depression.
Aetiology: Severe closed head trauma.
Features: Abnormal head posture (chin down), positive BHTT (bilateral), large V pattern, bilateral inferior oblique overaction, height reversal on lateral gaze (Left/Right on right gaze, Right/Left on left gaze), more than torsion (no fusion with prisms).

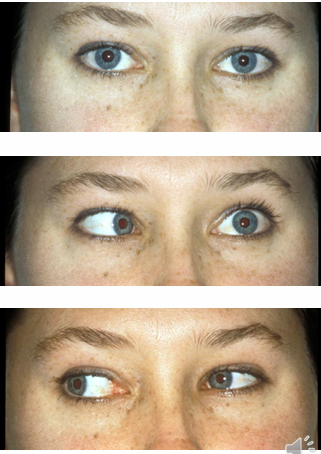
Sixth Nerve (Abducens) Paresis
Lateral rectus problems.
relatively vulnerable to damage
A common cause of paretic squint.
Causes
Vascular disease: Ischemia.
Mass: Tumour, aneurysm (e.g., sphenoid wing meningioma, cavernous internal carotid aneurysm).
Raised Intracranial Pressure.
Trauma: Severe blunt trauma, fracture of the base of the skull.
Clinical Signs and Symptoms
Failure of Abduction: Inability to properly abduct the affected eye.
Diplopia: Horizontal diplopia, worse on gaze to the affected side (abduction) and in the distance.
Head Turn: To the ipsilateral (affected) side to maintain binocular vision.
Differential Diagnosis: Possible confusion with Duane's syndrome.

Duane's Syndrome
A congenital condition.
Thought to be due to a failure of innervation of the lateral rectus by the VIth nerve, with anomalous innervation of the lateral rectus by the IIIrd nerve.
Clinical Features
Limitation of Abduction: Complete or partial.
Limitation of Adduction: Usually partial and minor.
Globe Retraction: The eye pulls back into the orbit on adduction.
Palpebral Fissure Narrowing: The eyelid aperture narrows on adduction.
Co-contraction: These phenomena are due to co-contraction of the medial and lateral rectus muscles.
Head Turn: May have a head turn to the affected side.
Observation: "WATCH MOTILITY IN PROFILE" to best observe the retraction.
Demographics: Most commonly affects females and the left eye, but can also be bilateral.
Brown's Syndrome
Characterized by mechanical disruption of eye movement.
Usually congenital, but can be acquired.
Involves the Superior Oblique (SO) tendon/trochlear pulley complex, leading to impaired movement of the tendon through the pulley.
sometimes hear a clicking noise
Clinical Features
Restriction of Elevation in Adduction: The primary characteristic.
Downshoot: Of the affected eye in adduction.
Hypotropia: Of the affected eye in primary gaze.
Head Posture: Possible chin elevation and head tilt to the affected side.
Differential Diagnosis: Simulates paresis of the Inferior Oblique (IO) muscle.
Movement Improvement: Elevation improves in other directions of gaze (away from adduction).


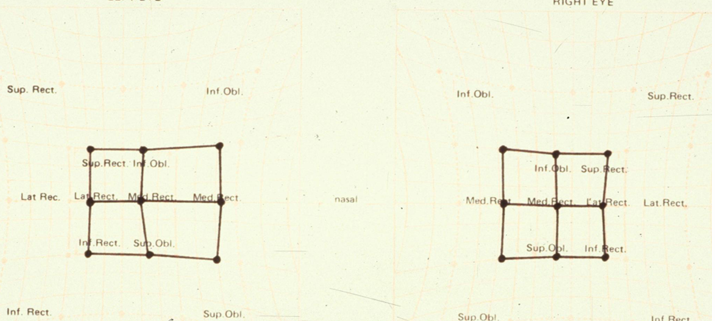
Paretic Sequelae (Spread of Comitance)
Over time following the onset of paresis, the oculomotor system attempts to minimize the effects of eye misalignment on vision. This adaptive process is known as the "spread of comitance."
Stages of Paretic Sequelae
Overaction of ipsilateral antagonist: The muscle in the affected eye that performs the opposite action of the paretic muscle overacts.
Overaction of contralateral synergist: The muscle in the other eye that works with the paretic muscle in its primary action overacts.
Underaction of antagonist of contralateral synergist: The muscle in the other eye that performs the opposite action of the overacting contralateral synergist shows underaction.
Overaction of ipsilateral synergist: The muscle in the affected eye that works synergistically with the paretic muscle in some positions of gaze overacts.
the greater the spread, the more difficult to detect incomitance.
Example: Right Superior Rectus (RSR) Paresis
If the RSR is paretic:
Overaction of ipsilateral antagonist: The Right Inferior Rectus (RIR) overacts.
Overaction of contralateral synergist: The Left Inferior Oblique (LIO) overacts.
Underaction of antagonist of contralateral synergist: The Left Superior Oblique (LSO) underacts.
Overaction of ipsilateral synergist: The Right Inferior Oblique (RIO) overacts.
Treatment
Optometric Management
Often difficult and unrewarding for the underlying paralytic condition.
Lenses: Ensure the patient has the best possible refractive correction.
Prisms:
Fresnels prisms can be used for trials.
Trial prism should address the problem causing the greatest hindrance to the patient (e.g., for a Superior Oblique weakness, prism may be needed for reading).
Occlusion: Used when diplopia is distressing to the patient to eliminate double vision.
Medical/Surgical Management
Referral for surgery: Often necessary for definitive correction of strabismus caused by paresis.
Primary Optometric Responsibility
Recognize cases of recent onset paralytic strabismus that are urgent and require rapid referral to an ophthalmologist or neuro-ophthalmologist, especially in cases like acute IIIrd nerve palsy suspected of aneurysm.