Positioning notes: C-spine & Soft tissue neck
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
98 Terms
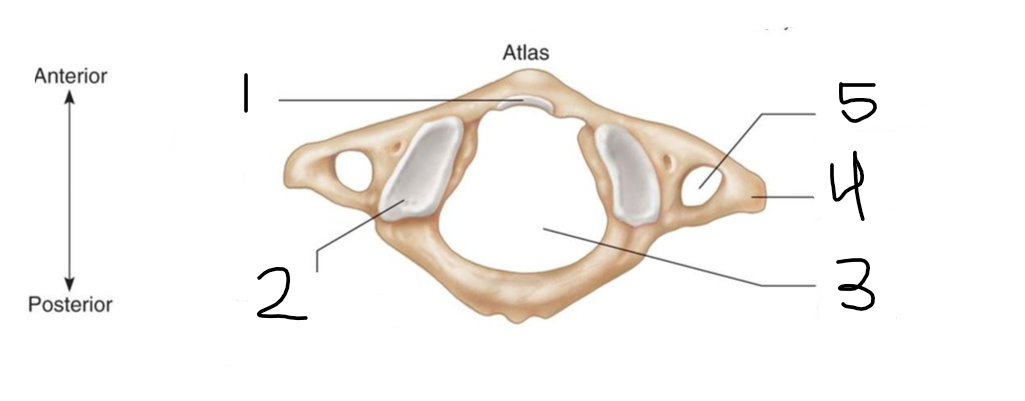
what is number 3 of the atlas?
vertebral foramen
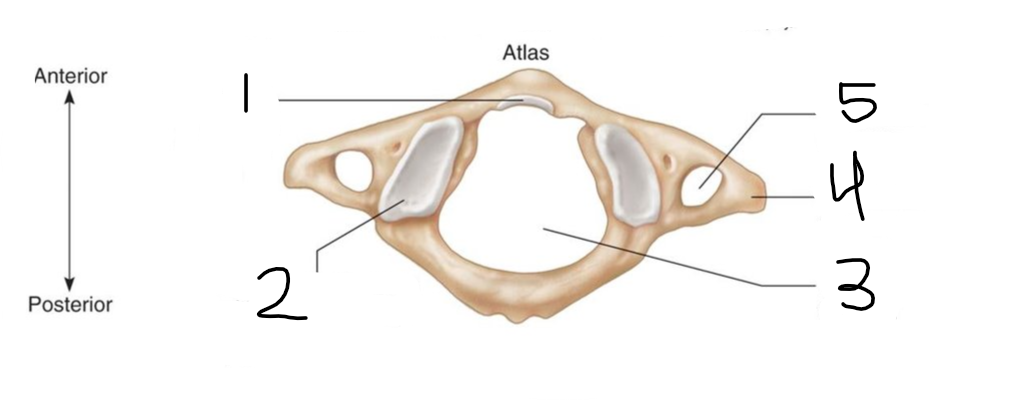
what is number 4 of the atlas?
transverse process
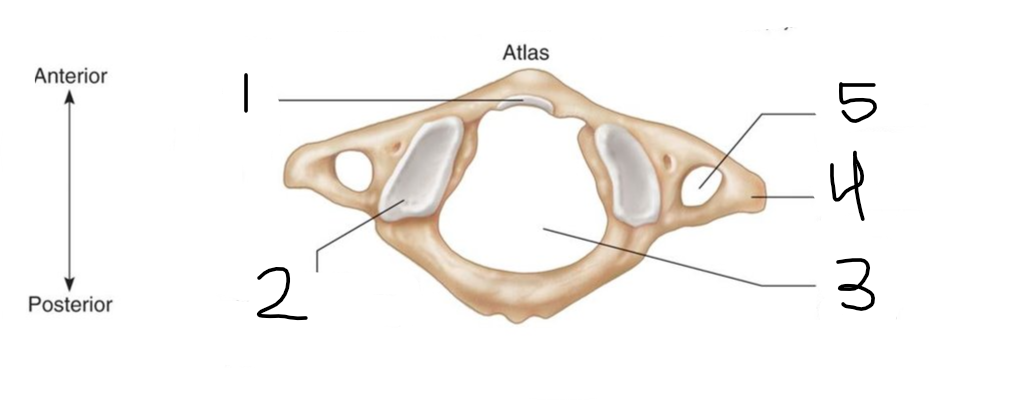
what is number 5 of the atlas?
transverse foramen
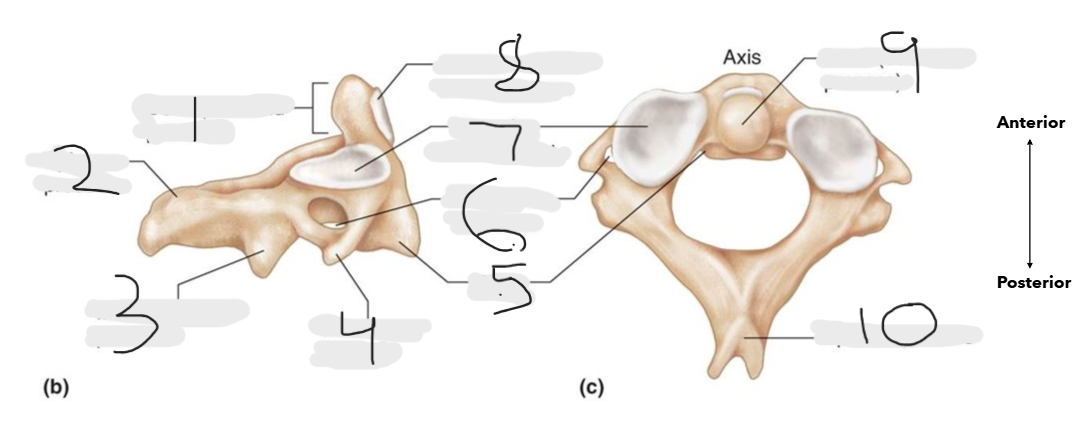
what is number 1 on the axis?
dens (odontoid process)
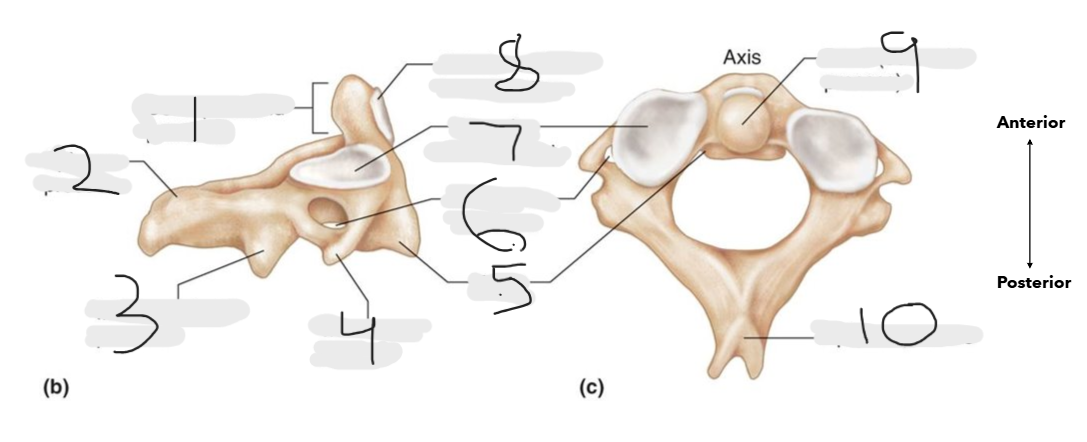
what is number 2 on the axis?
spinous process
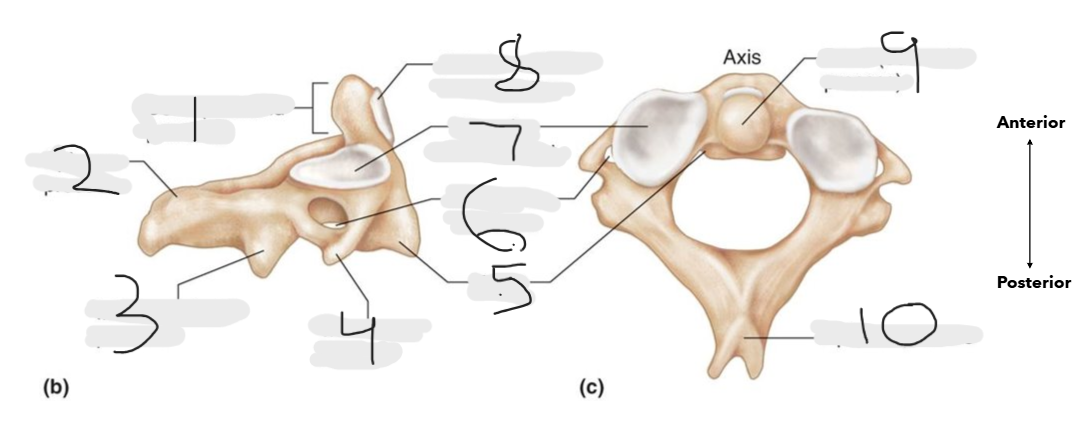
what is number 3 on the axis?
inferior articular process
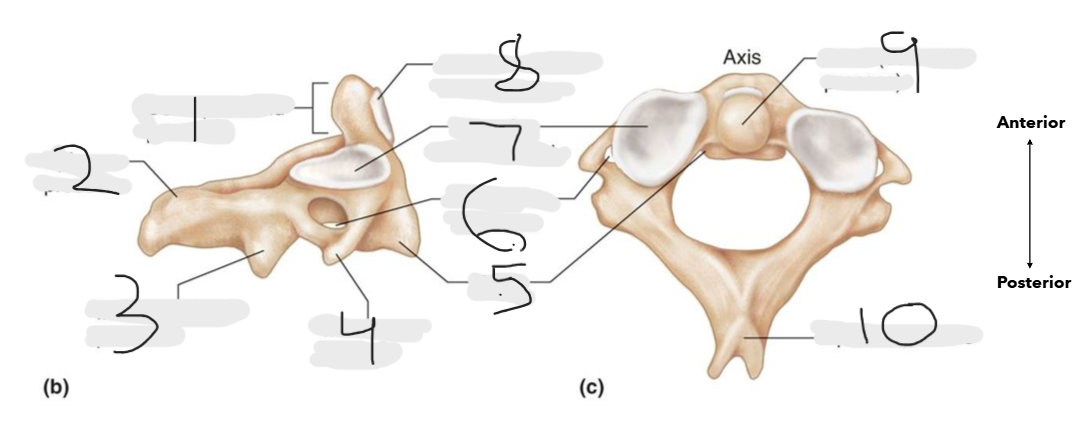
what is number 4 on the axis?
transverse process
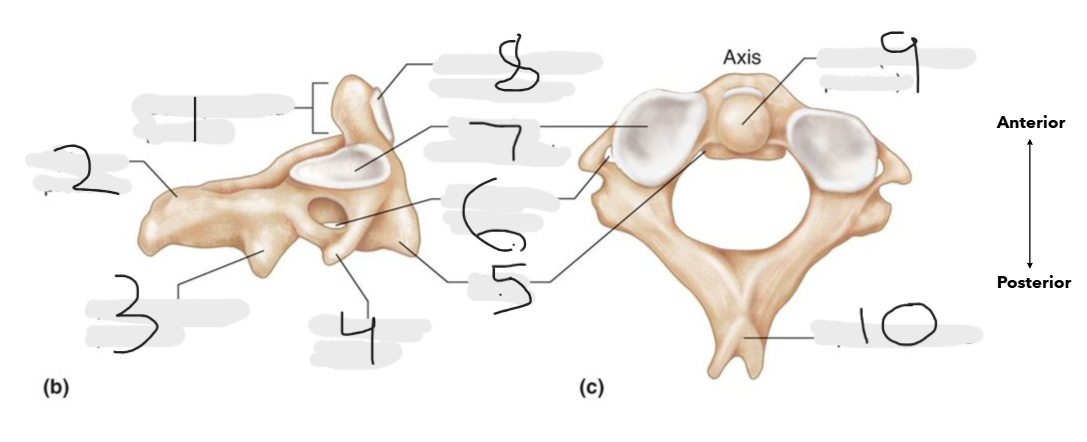
what is number 5 on the axis?
body
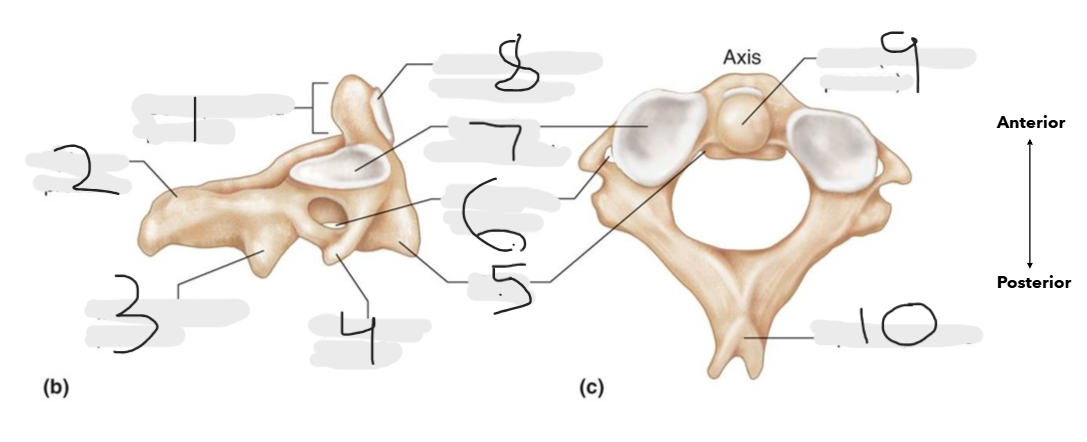
what is number 6 on the axis?
transverse foramen
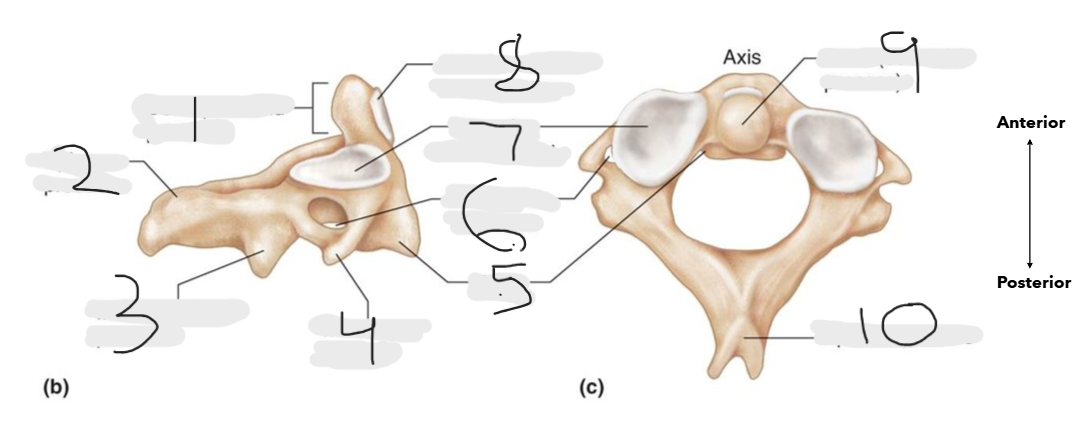
what is number 7 on the axis?
superior articular facet
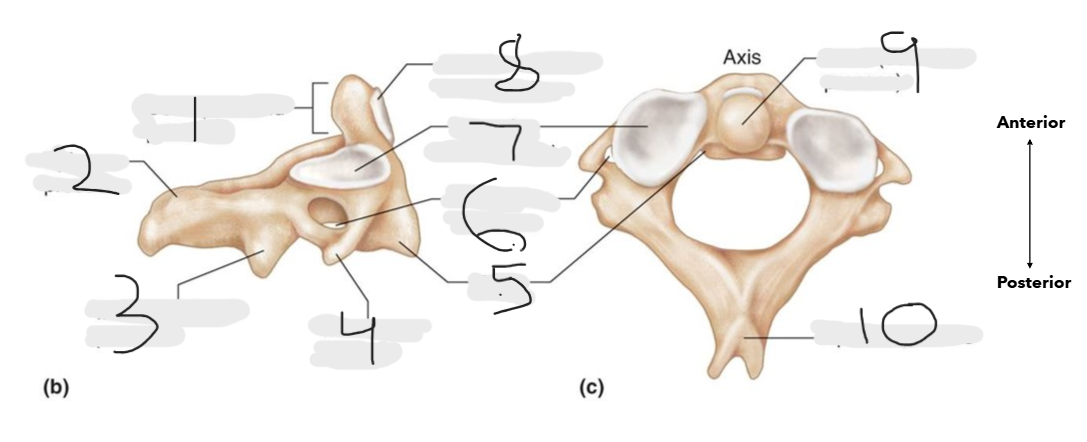
what is number 8 on the axis?
anterior articular facet for atlas
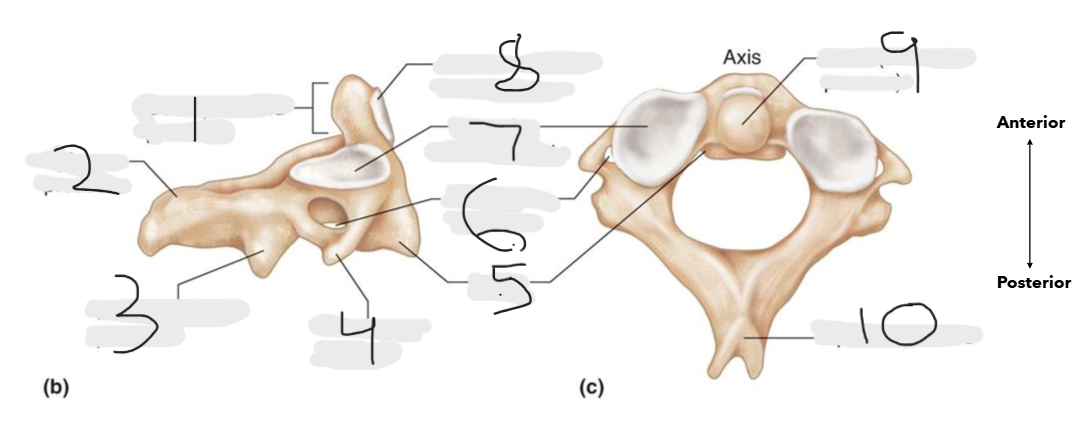
what is number 9 on the axis?
dens [odontoid process]
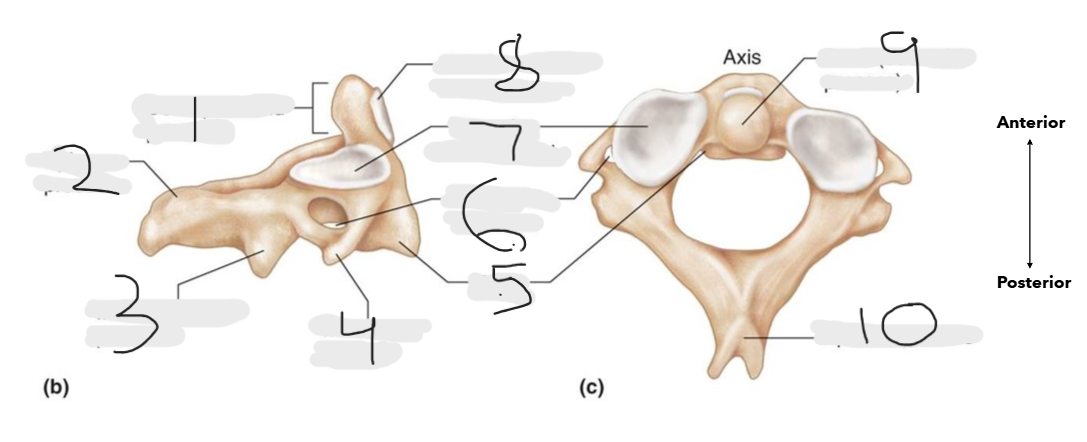
what is number 10 on the axis?
spinous process
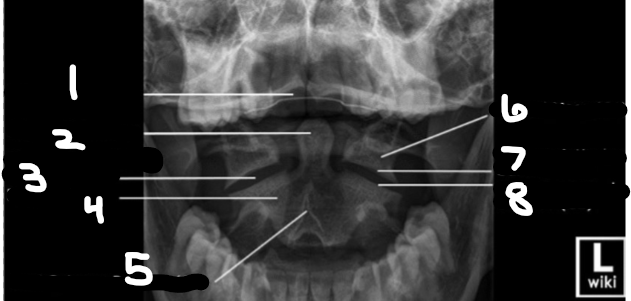
what is number 1 on this odontoid x-ray?
upper incisors
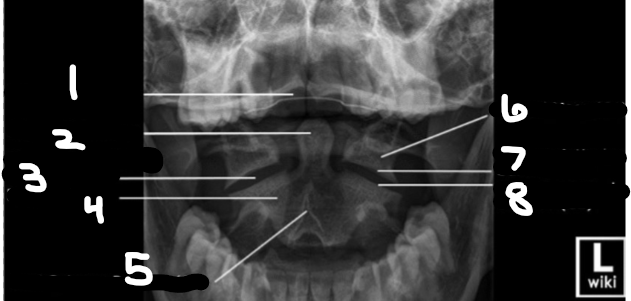
what is number 2 on this odontoid x-ray?
odontoid process
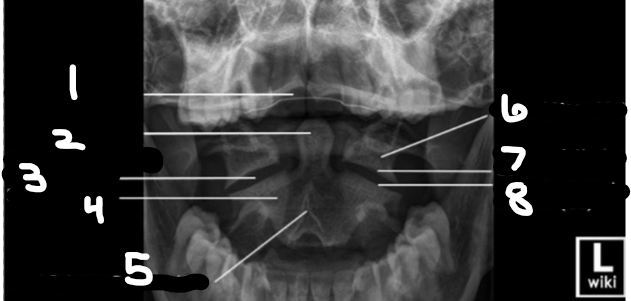
what is number 3 on this odontoid x-ray?
zygapophyseal joint space (C1-C2)
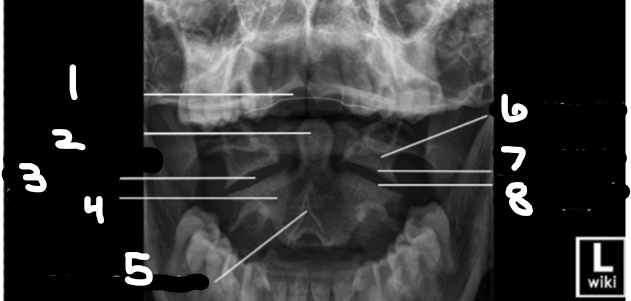
what is number 4 on this odontoid x-ray?
body (C2)
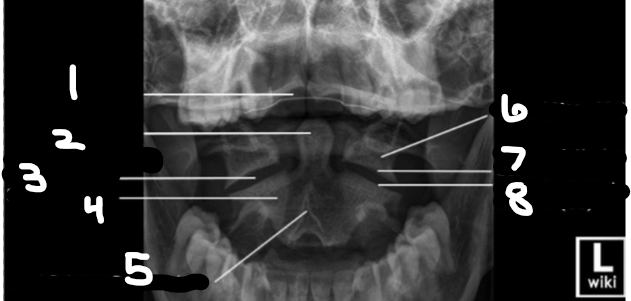
what is number 5 on this odontoid x-ray?
bifid spinous process (C2)
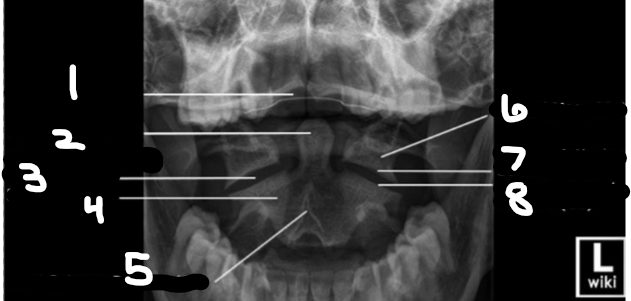
what is number 6 on this odontoid x-ray?
lateral mass (C1)
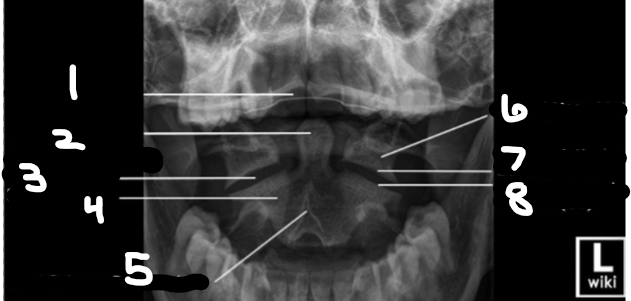
what is number 7 on this odontoid x-ray?
inferior articular surface (C1)
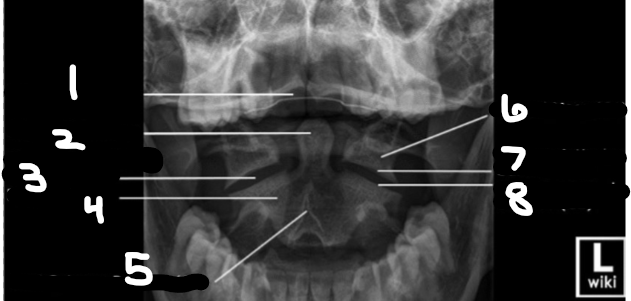
what is number 8 on this odontoid x-ray?
superior articular surface (C2)
C-spine protocol for Adult
AP, Odontoid, RAO, LAO, lateral
C-spine protocol for pediatric (2-18)
AP, Lateral, odontoid
C-spine protocol for pediatric (under 2)
AP & lateral
pediatric patients with trauma surgeon present get what view?
lateral only (unless trauma surgeon says otherwise)
left lateral c-spine technique
85 kVp, 8 mAs
left lateral c-spine
10×12 LW
72” SID
center @ C4
suspended expiration
C1-C7 & 1/3 of T1 is needed
cone down lateral purpose
if did not get C7-T1 on routine lateral
cone-down lateral technique
96 kVp, 28 mAs
cone down lateral c-spine
72” SID
4×17 LW collimation
center @ thickest part of shoulder
suspended expiration
C2-T1 needed
swimmer’s lateral purpose
only perform if unable to visualize C7-T1 on cone down
swimmer’s lateral technique
96 kVp, 28 mAs
swimmer’s lateral c-spine
40” SID
10×12 LW collimation
Center @ C7-T1 (2” above jugular notch)
suspended expiration
C5- T4 visualized through separation of humeral heads
AP axial c-spine technique
85 kVp, 3.2 mAs
AP axial c-spine
40” SID
10×12 LW collimation
angle 15-20 degrees CEPHALAD to C4 (thyroid)
suspended respiration
C3 to T2 visualized
Odontoid technique
85 kVp, 3.6 mAs
Odontoid c-spine
40” SID
5×5 collimation
Center to open mouth
suspended respiration
merrill’s recommendation for odontoid SID
30” (to increase FOV)
AP fuchs purpose
only done when upper dens not visible on good odontoid
(should NOT be done when fx is present)
AP fuchs technique
85 kVp, 7.1 mAs
AP fuchs c-spine
40” SID
5×5 collimation
center just inferior to top of chin
suspended respiration
PA axial obliques (RAO & LAO) technique
85 kVp, 10 mAs
PA axial obliques (RAO & LAO) c-spine
40” SID
10×12 LW collimation
45 degree obliquity
Center 15-20 degrees caudad at level of C5
suspended respiration
open foramina from C2-C3 to C7-T1
need C1-T1
additional oblique notes: SUPINE
Angle the tube 15 degrees cephalad and mark the side against the IR anterior to the neck
Special view: C-spine: Cross table lateral (trauma)
attending physician or radiologist must review this image to r/o fx or dislocation before removing collar or performing other projections
Lateral Flexion & extension: notes
**should not be attempted unless a cervical spine pathology or fracture has been RULED OUT
72” SID
8×10 or 10×12 LW
center at C4
marker placed posteriorly (annotate flexion & extension)
suspended EXPIRATION
Flexion & extension: C-spine merrills SID
60-72” (to compensate for increase in OID)
flexion & extension : C-spine- purpose
Demonstrate the normal anteroposterior movement or absence of movement resulting from trauma or disease (motility of cervical spine, discs and zygapophyseal joints). Frequently performed to rule out “whiplash” type or injury or to follow up after spinal fusion surgery.
evaluation criteria: flexion & extension c-spine
all 7 vertebrae in true lateral
no rotation or tilt of cervical spine
superimposed z- joints & open intervertebral disk spaces
superimposed or nearly superimposed rami of the mandible
spinous processes shown in profile
Flexion- body of mandible almost vertical & all 7 spinous processes in profile, elevated, & widely separated
extension- body of mandible almost horizontal & all 7 spinous processes in profile, depressed, & closely spaced
AP axial obliques (RPO & LPO): purpose
foramina farthest (OPPOSITE) from IR are demonstrated, opened, from C2-C7, T1. opened disk spaces
AP axial obliques (RPO & LPO)- angle
15-20 degree cephalad,
trauma axial oblique c-spine notes
do not use grid (double angle will cause grid cut off)
mark side opposite from tube
when CR enters right side, left foramina and disk spaces are demonstrated
when CR enters the left side, right disk spaces & foramina are demonstrated
Soft tissue neck (upper airway) routine views
lateral only
Soft tissue neck (upper airway) if ordered for foreign body
AP as well as lateral
left lateral: soft tissue neck technique
65-70 kVp, 3.2 mAs
left lateral soft tissue neck
40” SID
10×12 LW collimation
Center @ C4 (slightly anterior to EAM)
slow inspiration through the MOUTH
air filled trachea down to level of T1
additional note for pediatric patients for lateral soft tissue neck
Image is then taken on inspiration.
additional note: lateral soft tissue neck: merrills
patient should clasp hands behind the body & rotate the shoulders posteriorly to keep the arms from obscuring
jugular notch is at the level of
T2/T3
c2 appears taller than other cervical vertebra because ….
the dens
mastoid tip lies at __
C1
gonion lies at
C2-C3
pedicle
above & below foramina
intervertebral foramina
openings between pedicles
angle that intervertebral foramina lie in
45 degree from sternal plane & 15 degree from horizontal plane
what is the true lateral position
z joints (zygapophyseal joints)
secondary curve occurs
after birth
C1=
atlas
c2=
axis
c7=
vertebral prominence
z-joints lies around
C1
body on odontoid image lies around
c2
lateral mass lies around
c1
RAO=
right side being viewed (facing the board)
observes CLOSEST to board
RPO=
oPPosite is being viewed
jefferson fx is at the level of
c1
hangman fx is at the level of
c2
unique characteristics of c3-c6 vertebrae
bifid spinous process
pillars
foramina
what is part of 2 organ systems
pharynx
swimmers centering is
c7-t1
body of mandible on flexion should be
vertical
body of mandible in extension should be
horizontal
if the shoulder is not properly depressed for a swimmers lateral what angle should you put on?
3-5 degree caudad
vertebrae needed on lateral cspine
all 7 & at least 1/3 of T1
if the upper incisors are projected over the dens this means what?
chin is down
if the base of the skull is projected over the dens this means what?
chin is raised too high
on a fuchs, if the chin is over the dens & there is a “gap” above the dens=
chin is down, not enough angle
on a fuchs, if the tip of the dens is not in the foramen magnum & there is a “gap” beneath it=
chin is up, too much angle
what forms the z joints
superior & inferior articular processes
what are the openings between the pedicles?
intervertebral foramina
little or no angle on AP=
closed spaces; spinous process & chin superimposed over C3
tilt vs rotation on lateral
Tilt= z-joints are above/ below each other
Rotation= z-joints are next to each other
rotation on swimmers view
rami are off side to side & intervertebral foramina are seen
on odontoid if upper incisors overlap dens this means
chin not raised enough
on odontoid if base of skull is overlapping the dens & the dens is touching the foramen magnum=
chin raised too high
on a LAO/RAO, if the pedicles are off the border of the vertebral body & you can see the spinous process off the back (looks lateral), this means it is
over rotated
on a LAO/RAO, if there are “hills” on the front w/ intervertebral foramina closed off (looks AP), it is
under rotated
when to repeat for chin on soft tissue neck
if chin is in trachea