Core stability
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
2 muscle types
movement
consist of big muscles, fast twitch fibres → dynamic → move joints
stability
consist of smaller, deeper muscles + slow twitch fibres in other muecles
low grade contraction that lasts, provides support + control
need both muscle types for successful function
Whats responsible for stability at various joints
Upper quadrant
GHJ → scapula muscles tg = stabilisers for shoulder mvnt
middle + lower traps position scapula on chest wall
Lower quadrant
spine + trunk = multifidus + transversus abdominus (TrA) → support for trunk and lower quad mvnt
glut medius = NB at hip to support pelvis in WB acts
vastus medialis at knee
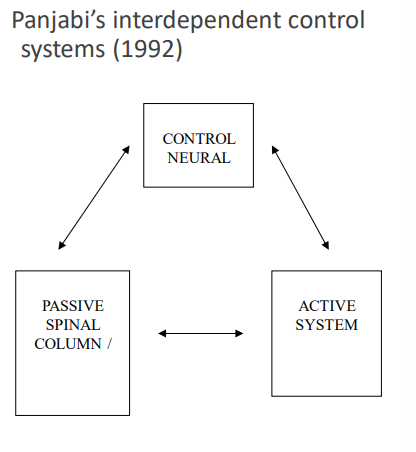
Why does back pain happen + 3 subsystems
Back pain occurs when deficit in one subsystem can no longer be compensated for by another
3 subsystems are matched
if have passive failure → will lead to muscle dysfx → changes in control → pain
Spinal stability (PASSIVE) (ligaments + art surfaces)
interspinous + supraspinous ligaments + facet joints + joint capsules + intv discs = stabilising structures for trunk flexion
ant long. lig + ant aspect of anular fibrosis + facet joints = stabilise end range trunk ext
intervertebral discs + facet joints = rotational mvnts
Spinal stability (ACTIVE)
consists of spinal muscles + tendons
Lumbar spine = unstable at low loads when muscles removed
Shows muscles are essential for spinal stability
Muscle activity = critical even for light tasks
Spinal stability (NEURAL)
Neural control = receives input from passive + active subsystems
Determines what's needed to keep spine stable
If neural control dysfunction + not restored after injury → other spinal structures at risk of injury
LBP patients = often have persistent neuromuscular control deficits
Recovery of proper neural control = NOT automatic after initial injury
Evidence base for core
TrA + multifidus = role in stabilising lumbar spine
TrA activates before + during unilateral arm + leg movements
Multifidus
deepest layer of back muscles
global muscles (erector spinae) run over it to extension movement
effects of LBP
transversus abd affected by LBP
loss of motor control (timing of activation, delayed activation, activation → phasic instread of tonic)
multifidis adversely affected on ipsilateral side as symptoms in LBP
fatigueability, activation, muscle composition, muscle size
Same core stability theories applied to chronic neck pain & headaches → focused on deep neck flexors + upper quadrant postural muscles as foundation for functional rehab.
Principle remains: stabilisers must work first before optimising others
Pilates + core stability
Pilates focuses on central core (pelvic floor, diaphragm, TrA, multifidus) → "centering" refers to this core.
Pilates = one method to activate & train spinal stabilisers if taught properly.
Where are we now with ideas on stability ?
Core stability ideas have been challenged recently as pain science evolved.
Biopsychosocial model says physical deficits aren't the only cause of pain — rehab must consider everything.
Focus on encouraging movement (not just rigidity), and core should work with other muscles, not be seen as more important.
Stability and movement systems are not separate — they function as a continuum, with muscles and joints sometimes doing both at once.
Core stability alone improves LBP in the short term but not long term, where general integrated exercises are just as effective.
There's some evidence that improved core strength enhances athletic performance. The focus should be on overall motor control and control during functional tasks.
NB things to note
Exercise and movement = key to recovery; avoid sedentary.
Match stability with dynamic mobility. Build rehab around patient's goals & needs.
No muscle group is more important than others — all work together for function.
The spine is not fragile — don't discourage movement or encourage too much stiffness, and avoid catastrophising about the back pain.
Assessing trA
2 methods:
Pressure biofeedback unit (objective measure of fx)
Method:
Before beginning explain anatomy and function of muscle
Prone lying, arms at side, neck straight if able or forehead resting on hands
Biofeedback cushion under abdomen with top edge in line with ASIS
Inflate cushion to 70mmHg
Without breathing activate TrA (pelvic floor, zip, hammock)
Pressure on cushion should decrease by 8-15mmHg
Hold for 10seconds while breathing diaphragmatically
Repeat 10x
Hands on monitoring (needs good palpation skills, useful if taught properly)
Manual method:
Before beginning explain anatomy and function of muscle
Crook lying
Physio and patient, palpate TrA 1cm in and 1cm down from ASIS
Breathe or sigh to relax abdominals
Without breathing activate TrA muscle (Pelvic floor, Zip, Hammock)
Palpate for contraction
Hold contraction x10 diaphragmatic breathes
Repeat 10x
Tricks:
breath holding, recuiting rectus, recruiting obliques (watch bulge) + shallow breathing
Multifidus retraining
standing/lying → pt to palpate MF
bulge muscle under fingers w/o active lumbar extension
hold contraction with diaphragmatic breathing
Assessing multifidus
palpation
prone lying w head in neutral
palpate muscle at each segment adjacent to spinous process on L + R side
breath in/hour, sigh to relax
command = gently swell out your muscles under my fingers without moving your spine or pelvis
hold 10x diagphragmatic breaths
repeat at next level then compare
TrA retraining
Stage 1
and drawing in to activate TrA + hold for 10 secs
use preferential activation w expiration
exercise e.g. = hundreds
Stage 2
challenge core contraction with diff positions
apply to sport/function
modify starting positions
Stage 3
introduce fx limb mvnts to challenge core contraction
use pressure biofeedback for ex in crook lying, sitting, standing while maintaining pressure on cushion
start w closed chain ex
choose ex based on pathology/fx/requirements of job or sport
Stage 4
incorporate core stability into fx + dynamic ex
reate ex to job/sport + apply sport training situations
make sure you can do this
Could you explain purpose
Demonstrate ex in steps
Set up posture and starting position
Facilitate mvt and gradually withdraw your input Introduce breathing
Use visualisations
Slow progressions – keep reviewing the basics!