T5 - IE4 - Infectious Diseases - Fong - Line Infection & Infective Endocarditis (IE)
1/157
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
158 Terms
Enterococcus spp. Penicillin and gentamicin susceptible 2 β-lactams treatment
Ampicillin (2 g IV q4H) 6 weeks
PLUS
Ceftriaxone (2 g IV q12h) 6 weeks
Synergy and use for two β-lactams discovered in 2012
Enterococcus spp. Penicillin and gentamicin susceptible treatment
Ampicillin (2g IV q24h) 4-6 week duration*
or
Penicillin G (18-30 million units / 24h IV continuously or in 6 equally divided doses) 4-6 week duration*
PLUS
gentamicin 1 mg/kg IV q8H 4-6 week duration*
*4 weeks if symptoms <3 months, 6 weeks if symptoms > 6 months or prosthetic valve
enterococcus spp
Staphylococcus spp. PROSTHETIC valve (MRSA, CoNS) treatment
vancomycin (dosed to target trough ~15 mg/L) ≥ 6 weeks
PLUS
rifampin (300 mg IV q8h); consider several day delayed start 2/2 resistance; ≥ 6 weeks
PLUS
gentamicin (3 mg/kg IV Q24h) 2 weeks
Staphylococcus spp. - PROSTHETIC valve MRSA, CoNS
Staphylococcus spp. PROSTHETIC valve (MSSA, CoNS) treatment
Nafcillin / Oxacillin (2g IV q4H) ≥ 6 weeks
PLUS
Rifampin (300 mg IV q8H) - considered several day delayed start 2/2 resistance; ≥ 6 weeks
PLUS
Gentamicin 3 mg / kg IV q24h 2 weeks
Staphylococcus spp. prosthetic - MSSA, CoNS
What is the benefit of de-escalating from vancomycin to nafcillin or cefazolin for treating MSSA?
A. less toxicity
B. narrower spectrum
C. easier dosing
D. lower mortality
E. all of the above
F. none of the above
All of the above
Nafcillin / cefazolin will have less nephrotoxicity, narrower spectrum which prevents resistance, easier dosing and has been proven since β-lactams have lower mortality in MSSA than vancomycin
Highly susceptible VGS and S. gallolyticus (bovis), PROSTHETIC valve treatment
penicillin G (24 million units / 24hr IV continuously or in 4-6 equally divided doses) for 6 weeks
OR
ceftriaxone 2 mg IV q24H for 6 weeks
±
gentamicin 3 mg / kg IV q24h or 1 mg / 1 kg IV q8h for 2 weeks
Highly susceptible VGS and S. gallolyticus - PROSTHETIC
Organisms of IE: streptococcus spp. - _______ ____________ / _________ ___________ are a significant risk factor
- poor dentition / dental procedures (are a significant risk factor)
Modified Duke Criteria - minor criteria for diagnosis IE: immunologic
glomerulonephritis
Osler's nodes
Roth's spots
rheumatoid factor
Modified Duke Criteria - Major Criteria for Diagnosis IE: Blood Culture - organism consistent with ____________ _______ in ___ separate blood cultures
- (consistent with) infective endocarditis
- 2 (separate blood cultures)
Mitral valve location
between left atrium and left ventricle
MitraL = left
Tricuspid = right
IE
infective endocarditis
Infective endocarditis
IE
When do we get blood cultures: just about ______ _____ ______
- all the time (regardless of source)
Systemic sign / symptoms of infection in hospitalized patients
Blood cultures are systemic _____ / ____________ of infection in hospitalized patients
- (systemic) sign / symptoms (of infection)
Incidence of bacteremia
community acquired pneumonia: as low as 5%
UTI: up to 15%
cellulitis: 10%
intra-abdominal infections: < 10%
infective endocarditis: > 80%
How to obtain good blood cultures: ____ ____ sets from ___ different sites
- ≥ 2 (sets)
- 2 (different sites)
Clean site of venipuncture
Avoid indwelling lines unless suspecting line infection
Before antibiotics started
How to obtain good blood cultures
Clean site of venipuncture
Avoid indwelling lines unless suspecting line infection
Before antibiotics started
How to obtain good blood cultures: _________ site of venipuncture
- Clean (site of venipuncture)
How to obtain good blood cultures: ________ indwelling lines unless suspecting line infection
- Avoid (indwelling lines)
How to obtain good blood cultures: ________ antibiotics
- Before (antibiotics)
Goal of good blood cultures
maximize probability of identifying pathogen, minimize probability of contaminants
Interpreting blood culture information: look for number of bottles __________
- (bottles) positive
4/4 vs. 1/4: high-grade bacteremia vs. possible contamination
Interpreting blood culture information: look for number of bottles positive
4/4 vs. 1/4: high-grade bacteremia vs. possible contamination
Depends on bug 4/4 and 1/4, sometimes it doesn't matter may also be quantity of the infection (i.e., if it Staph Aureus, we fear MRSA)
Interpreting blood culture information: organism identified tells you a lot of information
contaminant vs. infection
polymicrobial cultures: contaminants?
Interpreting blood culture information: organism identified tells you a lot of information - polymicrobial cultures...
contaminants
Interpreting blood culture information: generally provide _______, _______ answers
- clues
- NOT (answers)
Contaminants: who they are and why they matter
common contaminants - skin flora
~1-5% of blood cultures have contamination
Common contaminants - who they are and why they matter: Skin Flora
Coagulase - negative Staphylococcus epidermidis (CoNS)
Propionibacterium acnes
Corynebacterium spp.
Bacillus spp.
Contaminants: who they are and why they matter - ___-___% of blood cultures have contamination
- 1-5(% of blood cultures)
Increased cost to patients / healthcare system (~$1000 / patient in 1995)
Requires additional work-up, empiric antibiotics
Contaminants - who they are and why they matter: increased cost to ___________ / ___________ _________
- patients / healthcare system
~$1000 per patient in 1995
Contaminants - who they are and why they matter: requires additional...
work-up
empiric antibiotics
Contaminants - who they are and why they matter: WHEN contaminants matter
present of foreign material (e.g., pacemaker, prosthetic valves)
Skin flora do not set up infection in normal host, but in a patient with many comorbidities then it may cause many problems
Blood culture clinical pearls
There should always be a reason a culture is drawn
A positive blood culture alone does not guarantee true infection
Know the contaminants, but also know the pre-test probability
- pre-test probability: likelihood your test is going to be positive before testing
Blood culture clinical pearls: there should __________ be a reason a culture is ________
- always (be a reason)
- (culture is) drawn
Determine, if the patient has a fever, increased WBC when it was drawn...
Blood culture clinical pearls: a positive blood culture alone does _____ ____________ true infection
- (does) not guarantee (true infection)
Blood culture clinical pearls: know the ____________, but also know the _____-________ ___________
- contaminants
- (know the) pre-test probability
Pre-test probability: likelihood your test is going to be positive before test
Pre-test probability
prevalence (%); likelihood your test is going to be positive before test
When do we believe in blood cultures: _______________ identified fits the ___________ syndrome
- organism (identified fits)
- clinical (syndrome)
S. pneumoniae, in a patient highly suspected to have pneumonia; E. coli in a patient highly suspected to have a UTI
When do we believe in blood cultures: Organism identified fits the clinical syndrome
S. pneumoniae, in a patient highly suspected to have pneumonia
E. coli in a patient highly suspected to have a UTI
When do we believe in blood cultures: can help ________ diagnoses, but also determine ___________ of illness
- (help) confirm (diagnoses)
- (determine) severity (of illness)
Bacteremia often means sicker patients with risk for worse outcomes
When do we believe in blood cultures: can help confirm diagnoses, but also determine severity of illness
Bacteremia often means ________ patients with risk for ________ outcomes
- sicker (patients)
- worse (outcomes)
When do we believe in blood cultures: bacteremia needs a __________
- (needs a) source
Transient bacteremia (e.g. tooth brushing, cuts) rarely causes true infection...
When do we believe in blood cultures: transient bacteremia (e.g. tooth brushing, cuts) rarely causes __________ __________
- (rarely causes) true infection...
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (-) & CVC and AC ≥ 15 CFU
OR
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
CVC
central venous catheter
CFU
colony forming unit
AC
arterial catheter
Streptococcus grows in...
chains
Staphylococcus grows in clusters...
Staphylococcus grows in...
clusters
Streptococcus grows in chains...
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever
Blood cultures (-) & CVC and AC ≥ 15 CFU
FOR S. aureus...
TREAT 5-7 days, monitor closely for signs of infection, repeat blood cultures accordingly
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever
Blood cultures (-) & CVC and AC ≥ 15 CFU
FOR S. aureus: TREAT __-__ days, monitor closely for ______ of infection, ________ blood cultures accordingly
- (TREAT) 5-7 (days)
- (closely for) signs (of infection)
- repeat (blood cultures)
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever
Blood cultures (-) & CVC and AC ≥ 15 CFU
If due to other microbes...
monitor closely for sings of infection
repeat blood cultures accordingly
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
Coagulase-negative staphylococci
REMOVE catheter & treat with systemic antibiotic for 5-7 days
If catheter is retained, treat with systemic antibiotic + antibiotic lock therapy for 10-14 days
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
Coagulase-negative staphylococci - if catheter is retained, treat with __________ ______ + _________ _____ therapy for 10-14 days
- systemic antibiotic
- antibiotic lock (therapy)
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
Coagulase-negative staphylococci - if catheter is _________, treat with systemic antibiotic + antibiotic lock therapy for ___-____ days
- (catheter is) retained
- 10-14 (days)
Rifampin is good for activity against ____________
- (activity against) biofilms
Biofilms
Colonies of bacteria that adhere together and adhere to environmental surfaces.
Biofilms can cause difficult to manage major infections
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
Staphylococcus aureus, enterococcus, gram-negative bacilli
We _________ the catheter and treat with ___________ antibiotics
- remove (the catheter)
- (treat with) systemic (antibiotics)
The days of treatment may vary for each one i.e., Staphylococcus aureus ≥ 14 days; enterococcus 7-14 days, gram-negative bacilli 7-14 days
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
Candida
We _________ the catheter and treat with ____________ therapy for ____ days after the first negative blood cultuer
- remove (the catheter)
- (treat with) antifungal (therapy)
- 14 (days)
How do you know if it's a line infection - in a patient with a CVC or arterial catheter who has a fever...
Blood cultures (+) & CVC and AC ≥ 15 CFU by roll-plate of ≥ 10^2 sonication methods
Only coagulase-negative staphylococci may we __________ or ________ the catheter
- remove
- (or) retain
All of the other positive blood cultures REQUIRE the removal of catheter
Patients going for a deep-clean at the dentist may require ___________ __________
- (at the dentist may require) antibiotic prophylaxis
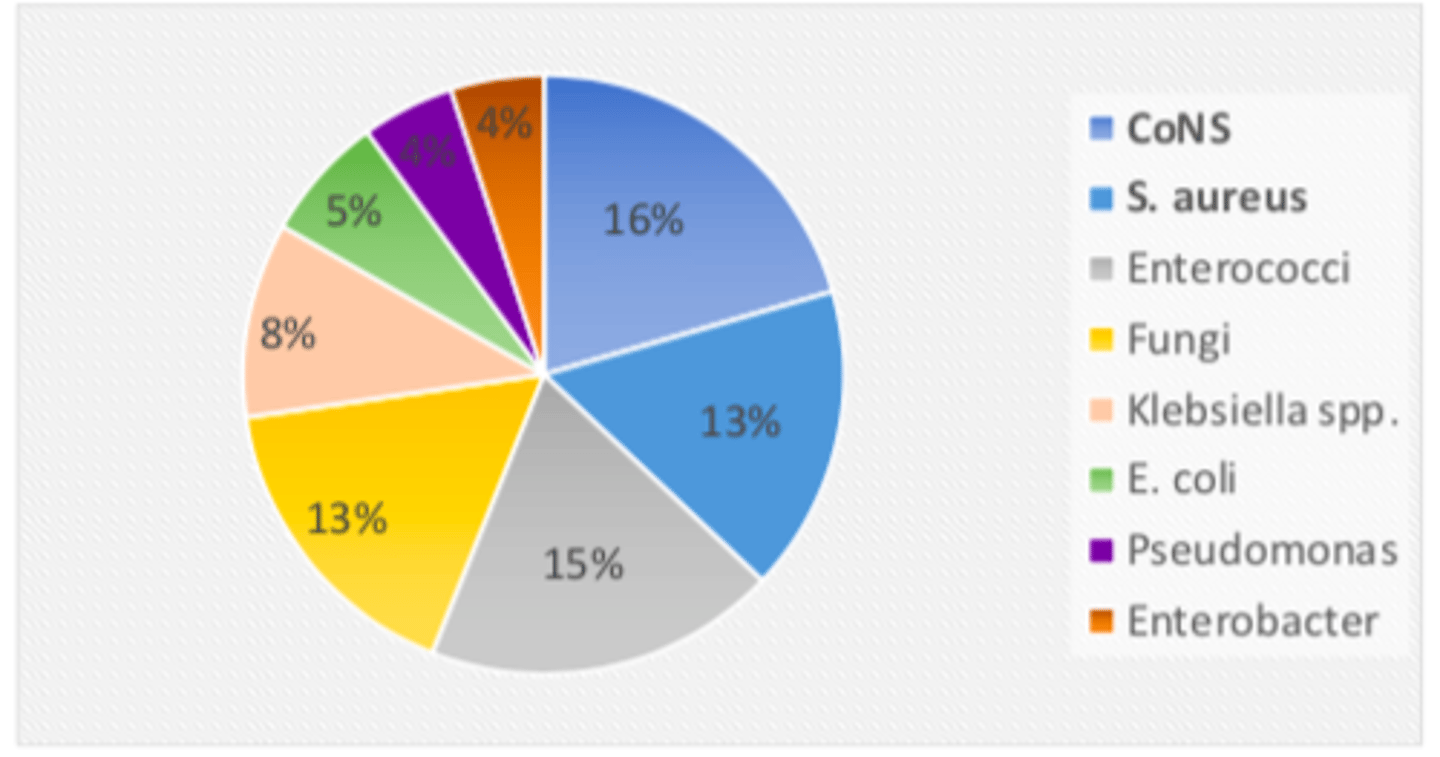
Microbiology of line infections figure
Infective endocarditis (IE) pathophysiology: ____________ host / immune system is generally capable of preventing ________ _____________
- Healthy (host / immune system)
- (preventing) infective endocarditis
Transient bacteremia rate from toothbrushing as high as 25%
Most common treatment for line infections...
Vancomycin
Due to vancomycin coverage of gram positive organisms
Approach to line infections: treat when appropriate - pathogen directed
______-________ empiric coverage, pathogen-directed _________ therapy
- gram-positive (empiric coverage)
- (pathogen-directed) definitive (therapy)
Approach to line infections: treat when appropriate - _________ directed
- pathogen (directed)
Gram-postiive empiric coverage, pathogen-directed definitive therapy
Duration often 7-14 days dpeneidng on organisms
Approach to line infections: assess positive cultures - do organisms fit clinical picture?
CoNS >>> S. aureus >>> Enterococci > Candida spp. > GNR
Approach to line infections: initiate __________ antibiotics if clinically warranted, access the ________ of illness
- empiric (antibiotics)
- (access the) severity
Approach to line infections: Remove lines whenever possible
Culture the ____________ _____
- (Culture the) catheter tip
Approach to line infections: Remove lines ____________ ________
- (remove lines) whenever possible
Culture catheter tip
Approach to line infections: paired blood culture collection (____________ line + ________)
- suspected (line)
- peripheral
Approach to line infections
1. Paired blood culture collection (suspected line + peripheral)
2. Remove lines whenever possible
- Culture catheter tip
3. Initiate empiric antibiotics if clinically warranted
- Severity of illness
4. Assess positive cultures – do organisms fit clinical picture?
- CoNS >> S. aureus >> Enterococci > Candida spp. > GNR
5. Treat when appropriate – pathogen directed
- Gram-positive empiric coverage, pathogen-directed definitive therapy
- Duration often 7-14 days depending on organism
Line Infection: all of the other positive blood cultures require the _________ of the catheter with the EXCEPTION of __________-__________ __________________
- removal (of the catheter)
- (EXCEPTION of) coagulase-negative staphylococci
Infective endocarditis (IE): damaged endothelium allows for ______________ ___________
- (allows for) bacterial adherence
Infective endocarditis (IE): most common sites of IE
1. mitral valve
2. aortic valve
3. tricuspid valve
Infective endocarditis (IE): obstructs flow and function of the heart, can mimic __________ ___________
- (mimic) heart failure
HACEK group
Haemophilus
Actinobacillus
Cardiobacterium
Eikenella
Kingella
Organism consistent with IE
viridans Streptococci
S. bovis
S. aureus
E. faecalis
HACEK group
Modified Duke Criteria: Major Criteria for Diagnosis IE
1. Blood culture positive for IE
2. TTE / TEE positive for IE
- oscillating intracardiac mass on valve, abscess or new partial dehiscence of prosthetic valve
3. New valvular regurgitation
Modified Duke Criteria - Major Criteria for Diagnosis IE: Blood Culture
organism consistent with IE (viridans Streptococci, S. Boris, S. aureus, E. faecalis, HACEK group) in 2 separate blood cultures
OR
persistently positive blood cultures
- ≥ 2 positive blood cultures drawn > 12 h apart OR all 3 of a majority of ≥ 4 separate blood cultures (first and last ≥ 1 hour apart)
Single positive blood culture for Coxiella burnetii
Serious complications of IE
heart failure (30%)
embolic stroke (20%)
other emboli (> 20%)
- kidney
- splenic
- pulmonary
"Less" non-specific symptoms of IE
chills
anorexia
weight loss
myalgias / arthralgias
night sweats
Non-specific symptoms of IE
Fever (90%)
Malaise / fatigue
Dyspnea
Cough
Headache
Abdominal pain
Risk factors of IE
Men over the age of 60
IVDU
Poor dentition
Structural heart disease (valvular / congenital)
Prosthetic valves
History of IE
Hemodialysis
do not need to know, for reference
Infective endocarditis (IE): _________ flow and function of the heart
- obstructs (flow and function)
Infective endocarditis (IE): __________ endothelium allows for bacterial adherence
- damaged (endothelium allows)
Most commonly affects
1. mitral valve
2. aortic valve
3. tricuspid valve
Infective endocarditis (IE) pathophysiology: healthy host / immune system generally capable of preventing IE
Damaged endothelium allows for bacterial adherence
Most commonly affects
1. mitral valve
2. aortic valve
3. tricuspid valve
Obstructs flow and function
- can mimic heart failure
Tricuspid valve location
between right atrium and right ventricle
Tricuspid = right
MitraL = left
Modified Duke Criteria - Major Criteria for Diagnosis IE: Blood Culture - single positive blood culture for ____________ __________
- (culture for) Coxiella burnetii
Modified Duke Criteria - minor criteria for diagnosis IE: vascular
septic pulmonary infarcts
intracranial hemorrhage
conjunctival hemorrhage
Janeway's lesions
Modified Duke Criteria - minor criteria for diagnosis IE: fever
> 38°C
Modified Duke Criteria - minor criteria for Diagnosis IE
1. predisposing heart condition or IVDU
2. fever (> 38C)
3. vascular: septic pulmonary infarcts, intracranial hemorrhage, conjunctival hemorrhage, Janeway's lesions
4. immunologic: glomerulonephritis, Osler's nodes, Roth's spots, rheumatoid factor
5. microbiologic: positive blood culture not meeting major criteria
Modified Duke Criteria - minor criteria for diagnosis IE: predisposing _______ condition or ______
- heart (condition)
- (or) IVDU
IVDU will usually present with _______-______ heart failure
- (present with) right-sided (heart failure)
Intravenous goes into the venous system and into one of the vena cavas, thus, the right side of the heart
IVDU
intravenous drug user
Modified Duke Criteria - Major Criteria for Diagnosis IE: new ___________ __________
- (new) valvular regurgitation
Modified Duke Criteria - Major Criteria for Diagnosis IE: TTE / TEE positive for IE
Oscillating intracardiac mass on valve, abscess or new partial dehiscence of prosthetic valve
Modified Duke Criteria - Major Criteria for Diagnosis IE: _____ / ______ positive for IE
- TTE / TEE (positive)
Oscillating intracardiac mass on valve, abscess or new partial dehiscence of prosthetic valve
Modified Duke Criteria - Major Criteria for Diagnosis IE: Blood Culture - persistently positive blood cultures
≥ 2 positive blood cultures drawn > 12 hours apart
OR
all of 3 or a majority of ≥ 4 separate blood cultures (first and last ≥ 1 hour apart)
Osler's nodes
painful immune-complex depositions
