O&G Matrix
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
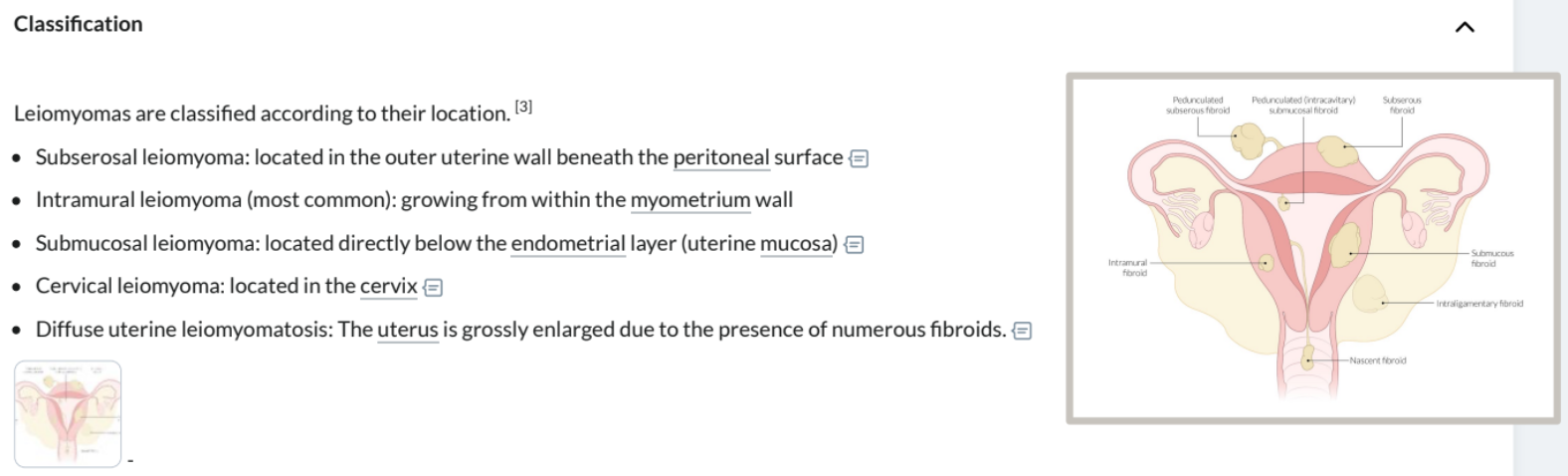
Leiomyomata Fibroids (R1) Ix
Benign uterine tumour primarily composed of smooth muscle and fibrous connective tissue
Round, firm, and well-circumscribed nodules
Located either submucosal (beneath endometrium), intramural (within uterine wall), or subserosal (beneath peritoneum)
Sx: mostly asympt., excess uterine bleeding → anaemia/menorrhagia, back/abdo/pelvic pain, bowel/urine sx miscarriage/infertility (distorted uterine cavity)
RF: obesity, age 25-40yrs, nulliparity, early menarche, African Americans
First Line: Exam (enlarged irregular uterus, irregular firm pelvic mass on bimanual exam)
Gold Standard: Pelvic US (well circumscribed uterine tumours), Endometrial Biopsy, Hysteroscopy
Other: MRI pelvis ± IV contrast (characterise leiomyomas), Sonohysterography, Bloods (CBC, BMP, Urine preg.; Abn. Bleeding = PT, PTT, fibrinogen, TSH, LFTs, von Will disease studies)
Leiomyomata/Fibroids (R1) Mx
First Line: nil if asymp., annual follow-up
Long Term:
Surgical: hysterectomy, myomectomy (remove leiomyomas to preserve fertility)
Uterine Artery Embolisation
Pharmacotherapy: GnRH Agonists/Antagonists, IUDs, Oral Contraception
Cx: miscarriage/infertility (distorted uterine cavity)
DDx: Adenomyosis, Endometriosis, Uterine Polyps, Uterine Leiomyosarcoma
Endometrial Carcinoma (R2)
Type I = endometrioid origin/hyperplasia; Type II = serous/clear cell origin
Early stage = favourable prognosis
RF: postmenopausal women (age 55-64yrs)
Sx: Painless Abnormal Uterine Bleeding!, Pelvic Pain, Palpable Mass
Ix: Transvaginal US → Endometrial Biopsy
Mx: Surgical (Total hysterectomy w bilat. salpingo-oophrectomy), Radiotherapy/Chemo, Hormone therapy
Endometritis (R2)
Inflammation of the uterine lining (endometrium) caused by infection typically postpartum (within first week or 1-6wks)
Usually a polymicrobial infection
Rare = Critically Ill w Sepsis/Septic Shock from Strep. pyogenes (GAS) or Clostridiums
RF: C section
Sx: fever (>38°C), lower abdo pain, uterine tenderness, purulent vaginal discharge
Ix: vitals + clinical exam
Mx: Abx (nonsevere = amoxicillin + clavulanate, severe = IV gent/tobramycin + amoxi/ampicillin + met)
Endometrial Polyps (R2)
Benign endometrial tumor: localised overgrowths of endometrial tissue within uterine wall
0.5-4% of polyps are premalignant/malignant
RF: postmenopausal women, HTN, Obesity, Tamoxifen, Lynch syndrome
Sx: asymp., irregular vaginal bleeding = menorrhagia/spotting, infertility in premenopausal
Ix: Transvaginal US, hysteroscopy, Endometrial biopsy (rule out)
Mx: surgical removal if symp. (hysteroscopy)
Adenomyosis (R2)
Benign endometrial tissue within the uterine wall
RF: early menarche, increased parity, past uterine surgery
Sx: dysmenorrhea, abnormal bleeding, menorrhagia, chronic pelvic pain; Exam = bulky, tender, diffusely enlarged uterus
Ix: Transvaginal US, Endometrial Biopsy
Mx: IUD!, Hysterectomy, Hormone Therapy, NSAIDs/TXA
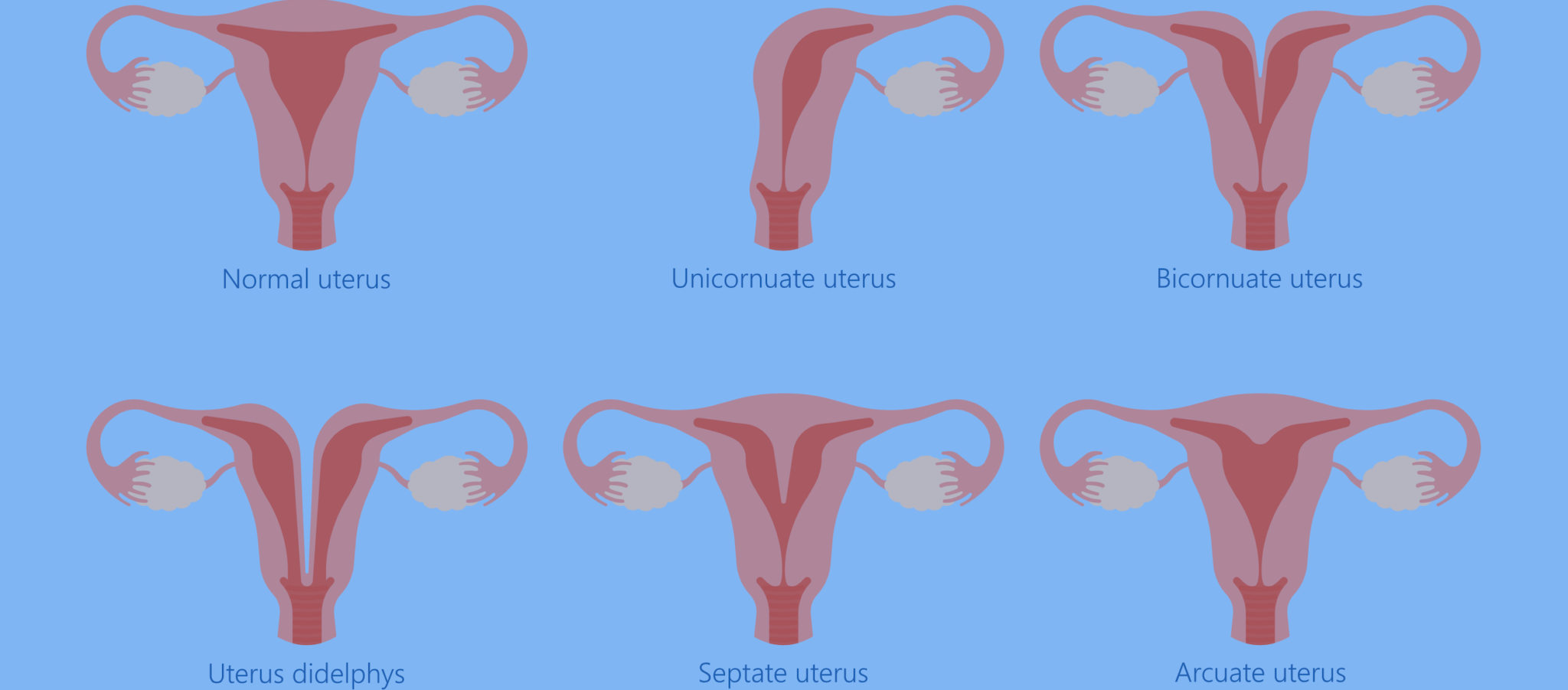
Congenital Uterine Malformations (R3)
Structural malformations of the uterus occurring during fetal development when the Müllerian ducts fail to properly fuse, affecting approx. 5% of women
Often asymptomatic, but can cause infertility, recurrent miscarriage, preterm birth
Types of Malformations:
Septate Uterus (Most Common): A partition (septum) divides the uterus into two parts, though the external shape is normal
Bicornuate Uterus ("Heart-shaped"): The uterus has an abnormal, indented top, creating two distinct cavities
Uterus Didelphys ("Double Uterus"): The Müllerian ducts fail to fuse at all, resulting in two separate uteri and often two cervices
Unicornuate Uterus: Only one side of the uterus develops fully
Arcuate Uterus: A minor variant with a slight indentation at the top, usually considered a minor anatomical variation.
Absent Uterus (Müllerian Agenesis): Uterus fails to develop
Uterine Sarcoma (R3)
Uterine cancer developing in the supporting muscles or connective tissues (myometrium/mesenchymal cells), often unrelated to estrogen
Much rarer than Endometrial Carcinomas (5% of cases)
Often more aggressive
Cervical Carcinoma + Pre-Cancer (R1) Ix
Third most common type of gynecological cancer (after endometrial and ovarian) but declining with Pap Smears and HPV Vaccinations
Types:
Squamous Cell Carcinoma: Most Common (80%), Usually HPV 16, invasive, irregular cell morphology (hyperchromatic, loss of basal membrane)
Adenocarcinoma: (20%) Usually HPV 18, Atypical columnar epithelium
Small Cell Carcinoma: (2%) Neuroendocrine tumour, infiltration of monotonous round atypical cells in a nesting pattern (nuclei w salt + pepper chromatin)
Cervical Intraepithelial Neoplasia/CIN: premalignant epithelial dysplasia preceding cervical carcinoma
RF: HPV infection (types 16 + 18) → early onset sexual activity, multiple sexual partners, STD Hx, immunosuppression; DES exposure in-utero, smoking
Sx: early = asymp.; advanced = vaginal bleed/postcoital spot, purulent discharge, pelvic pain ± lower back pain
First Line/Screening: Pap Smear, HPV DNA test, Speculum/Bimanual Vaginal Exam
Gold Standard: Colposcopy + Cervical Biopsy (Grades CIN I-III)
Cervical Carcinoma +.Pre-Cancer (R1) Mx
High-Grade CIN: Excision
Invasive: surgery, radiation therapy ± chemotherapy
Prevention: HPV Vaccination (age 9-26yrs), Screening (PAP Smear = age 25-65yrs every 5yrs)
Mx of Abnormal Screening Results: HPV 16/18 = Colposcopy; Other HPV = Repeat Screen in 12m
Cervical Ectropion (R3)
Benign, common and harmless condition where glandular cells typically lining the cervical canal spread to the outer surface of the cervix. Driven by estrogen levels influencing fragile cervical epithelium
Does not increase risk of cervical cancer
Usually no Hx of purulent discharge
RF: Commonly seen in adolescent or pregnant women, women on contraceptive pills and fertile women
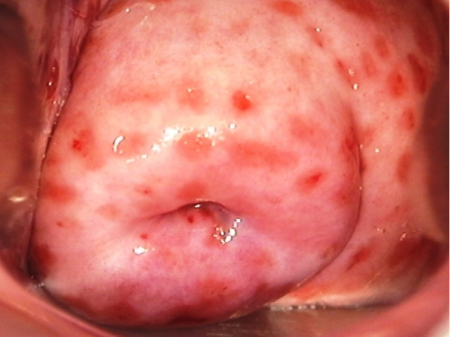
Acute & Chronic Cervicitis (R3)
Inflammation of the cervix characterised by a purulent endocervical exudate and/or easily induced endocervical bleeding (caused by manipulation with an atraumatic instrument like a cotton swab)
Pathogens: Neisseria gonorrhoeae, Chlamydia trachomatis, HSV
Sx: Often Asymptomatic, ‘Strawberry Cervix’ (trach.), postcoital bleed, purulent vaginal/cervical discharge
Cx: Pelvic Inflammatory Disease (if left undiagnosed or untreated) → infertility, chronic pelvic pain
Cervical Polyps (R3)
Small, benign, finger-like growths developing on the surface of the cervix or inside the cervical canal
Rarely cancerous, usually asymptomatic incidental findings
Most common in women >20yrs (esp. premenopausal or multiparous)
Generally associated w chronic inflammation or hormonal fluctuations
Nabothian Follicles/Cysts (R3)
Small, benign, mucus-filled lumps forming on the surface of the cervix
Naturally occurring due to normal cervical skin cells blocking the small mucus-producing glands, trapping mucus
Are harmless and require no Mx unless if grown exceptionally large
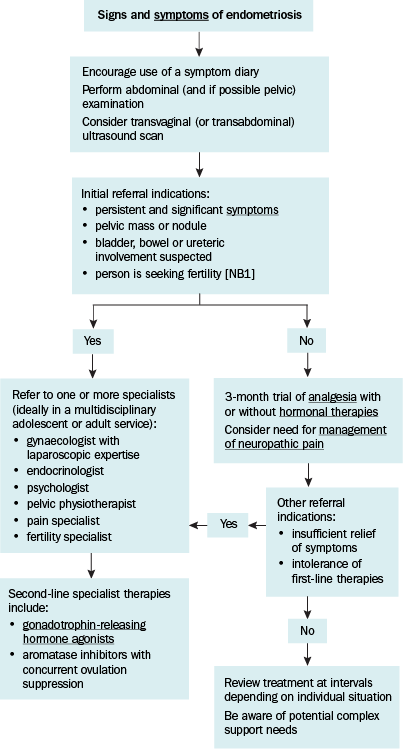
Endometriosis (R1) Ix
Benign chronic disorder where endometrial tissue occurs outside the uterus
Common Locations: ovaries, rectouterine pouch, fallopian tubes, bladder, cervix, peritoneum
Endometrial tissue reacts to the hormone cycle
Sx: dysmenorrhea, dyspareunia, chronic pelvic pain, infertility rectovaginal tenderness (sx may improve after preg./menopause)
First Line: Transvaginal US (chocolate ovarian cysts, nodules in bladder or rectovaginal septum)
Gold Standard: Laparoscopy (endometriotic implants and adhesions), MRI (asym. myometrial thickening, cysts)
Endometriosis (R1) Mx
First Line:
Analgesia: NSAIDs
Hormone Therapy: OCP, Progesterone-Only Contraception (IUD, Mini-Pill), GnRH Agonists (goserelin, nafarelin)
Long Term: Surgical removal of endometriotic tissue (hysterectomy, single excision)
PCOS (R1) Ix
Endocrine Disorder characterised by Hyperandrogenism, Oligoovulation/Anovulation ± presence of Polycistic Ovaries
Sx: Hyperandrogenism (hirsutism, acne, virilisation, alopecia), Oligoovulation/Anovulation (irregular periods, amenorrhea), Metabolic Syndrome (obesity, NAFLD)
First Line:
Clinical Exam: ↑ BMI, ↑ BP, Signs of insulin resistance (acanth nigr., skin tags), Hirsutism
US: Transvaginal/Transabdominal, not required for dx, shows cystic follicles
Laboratory Tests: ↑ Testosterone, ↓ SHBG, Androgens, Lipids, TSH/Prolactin (to rule out), Serume LH/FSH (if amenorrhea - ↑LH w LH/FSH ration >2:1), 24hr urine cortisol (rule our Cushing’s)
Confirm hyperandrogenism and exclude similar DDx (congenital adrenal hyperplasia)
PCOS (R1) Mx
Must tailor Mx to reproductive goals
First Line:
Lifestyle: loss of 5% of body weight, manage RFs (CVD, Psych, Lipids, DM etc)
OCP/IIUD (if preg. not desired): mx menstrual disturbances
Ovulation Inducers (if preg. desired): Letrozole
Antiandrogens: Spironolactone, Finesteride
Metformin: improves glucose metabolism + suppresses ovarian androgen production (not commonly used)
Long Term: Surgically remove underlying cause (androgen-secreting tumours)
Cx: Metabolic Syndrome (obesity, insulin resistance, hypercholesterolemia), Endometrial Cancer (screen! lack of progesterone-induced endometrial shedding → endometrium proliferation → ↑ risk endo ca.)
Ovarian Carcinoma (R1) Ix
RF: BRCA1/2 gene, Hormonal RFs (↑ nbr lifetime ovulations), Age >60, HNPCC syndrome
Sx: asymp./abdo discomfort/urinary freq/bloating in early stages, ascites, pelvic pain
Red Flag: persistent bloating in older women
Types of Ovarian Tumours:
Epithelial Ovarian Tumour: from ovarian surface epithelium, mostly benign
Benign: cystadenomas, brennar tumours
Malignant: cystadenocarcinoma, endometrioid carcinoma, clear cell tumout
Germ Cell Ovarian Tumour: from primordial germ cells (oocytes), benign or malignant (agressive)
Benign: dermoid cysts/mature cystic teratoma, struma ovarii
Malignant: immature teratoma, yolk sac tumour, dysgerminoma, nongestational choriocarcinoma
Sex Cord and Stromal Ovarian Tumours: from sex cord cells (Sertoli, Granulosa cells) or stromal cells (Fibroblasts, Primitive Gonadal Stroma), benign or malignant
Benign: ovarian fibroma, theca cell tumour, Sertoli-Leydig cell tumour
Malignant: granulosa cell tumour, occ. Sert-Ley
First Line: Transvaginal US, CA-125 Tumour Marker (can also be raised in menstruation/endometriosis)
Benign:
Unilocular
Small solid components
Presence of acoustic shadows (indicates dermoid cyst/mass)
Smooth multilocular tumour
No blood flow on doppler
Malignant:
Irregular solid component
Ascites
>4 papillary structures
Irregular large multilocular solid tumour
Very strong blood flow on doppler
Ovarian Carcinoma (R1) Mx
Poor Prognosis
First Line: surgical staging/debulking, chemo, radiation
Premenstrual Syndrome/PMS (R1) Ix
Somatic and psychological sx during the luteal phase of the menstrual cycle
Sx: irritability, mood swings, anxiety, depression etc, bloating, headache, breast discomfort
First Line: Hx/Sx Charting over 2 menstrual cycles
Exclude Other Causes: thyroid disorders, menopause etc
Premenstrual Syndrome (R1) Mx
First Line/Long Term:
CBT
OCP: suppress ovulation → reduce sx (progestogens alone are ineffective)
SSRIs/SNRIs: Fluoxetine, Sertraline, mx physical/psych sx used only during luteal phase (2wks before menstruation)
Spironolactone: relieve bloating, swelling, breast discomfort, limited evidence
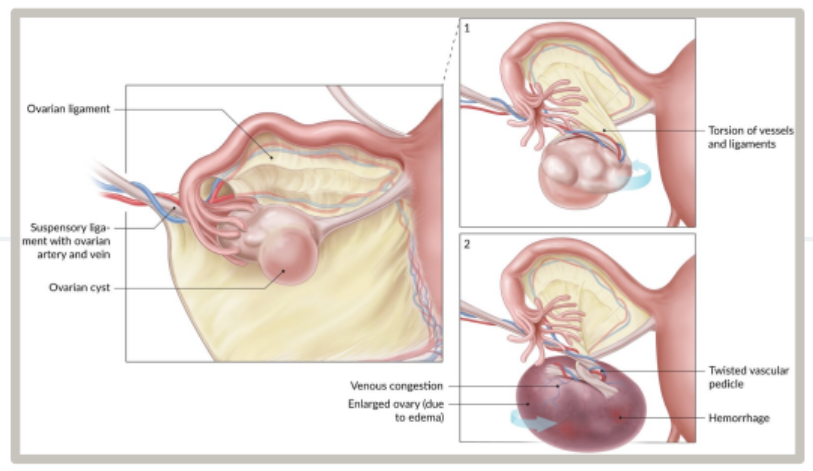
Ovarian Torsion (R1) Ix
Twisting of an ovary around the adnexal ligaments: partial or complete twisting of the ovary and fallopian tube around their supporting ligaments
Torsion → venous congestion/edema → ovarian blood supply cut off
RF: women of child-bearing age, ovarian enlargement (cysts/dermoid cysts, tumours etc → weight on ovaries), pelvic ligament laxity, Hx PID, previous pelvic surgery
Sx: sudden onset unilateral lower abdominal/pelvic pain, palpable adnexal mass/adnexal tenderness
Intermittent/spontaneously resolving pain = partial torsion
First Line:
Pelvic US w Doppler (Transvaginal): enlarged. edematous ovary with decreased blood flow
Bloods: G+H/Coagulation Panel/CBC (emergency preoperative tests)
Other: MRI/CT Abdo/Pelvis w Contrast (if US inconclusive)
Ovarian Torsion (R1) Mx
Surgical Emergency!
First Line: Exploratory Laparoscopy (indicated in all pts w suspected ovarian torsion) - adnexal detorsion + ovary preservation, oophrectomy ± salpingoectomy (if necrotic ovaries), ovarian cystectomy
Long Term:
Cx: ovarian necrosis + infertility if tx is delayed
Premature Menopause (R2)
Primary Ovarian Insufficiency (POI)
Permanent cessation of menses/ovarian function for >1yr before 40yrs of age
RF: FHx, Chemo/Radiation Exposure, Autoimmune Disease
Sx: clinical features of menopause (hot flushes, mood swings, cessation of menses), infertility, non-returning menstrual cycles post-hormonal contraception
Ix: Clinical Hx, Identify Underlying Cause, ?POI karyotyping (if <30yrs old)
Mx: hormonal therapy (↓ menopause sx) = OCP, HRT
Benign Ovarian Tumours (R2)
First Line Ix: Transvaginal US, CA-125 Tumour Marker (can also be raised in menstruation/endometriosis)
Benign:
Unilocular
Small solid components
Presence of acoustic shadows (indicates dermoid cyst/mass)
Smooth multilocular tumour
No blood flow on doppler
Types of Benign Ovarian Tumours:
Epithelial Ovarian Tumour: cystadenomas, brennar tumours
Germ Cell Ovarian Tumour: dermoid cysts/mature cystic teratoma, struma ovarii
Sex Cord and Stromal Ovarian Tumours: ovarian fibroma, theca cell tumour, Sertoli-Leydig cell tumour
Ovarian Cysts (Just to Know)
Fluid-filled sacs within the ovary, often resulting from a disruption in the follicles or corpus luteum development
Sx: Usually asymp., menorrhagia, PCOS sx, palpable adnexal mass, abdo pain
Ix: Pelvic US, B-hCG (rule out preg.)
Types of Ovarian Cysts:
Follicular Cyst: most common ovarian mass in young women, from growing Graafian follicles that fail to rupture/release egg (ovulation), large (~7cm)
Corpus Luteum Cyst: enlagement/buildup of fluid in the corpus luteum following failure to regress after ovum release, produces progesterone → delayed menses, common in preg.
Theca Lutein Cysts: multiple cysts typically developing bilaterally, from ↑ B-hCG/gonadotropins causing ↑ stimulation
Nonfunctional Ovarian Cysts: ovarian cysts that do not produce hormones (chocolate cysts, dermoid cysts, cystadenoma = serous or mucinous, malignant cysts/ovarian ca.)
Vaginismus (R3)
Involuntary tightening or spasm of the pelvic floor muscles surrounding the vagina
Automatic reaction making vaginal penetration (e.g. sexual intercourse, tampons, pelvic exam) difficult, painful, or completely impossible
Psychological or Physiological Triggers (anxiety, endometriosis)
Sx: Vaginal burning, stinging, or severe pain during any penetration attempts
Mx: pelvic floor physio, vaginal dilators, psychotherapy
Vulvodynia (R3)
Painful vulva of idiopathic origin
Chronic, unexplained pain, burning, or discomfort in the vulva (the external female genitalia) lasting for >3m
Sx: Pain with insertion at intercourse/w tampon + to touch
Mx: supportive/pain mx (Tricyclics, nerve creams etc)
Vulval Carcinoma (R3)
Malignancy of the outer female genitalia (vulva)
Predominantly occurs in postmenopausal women
Poor prognosis
RF: HPV infection, smoking, vulvar dystrophy/neoplasia
Sx: vulval lumps/lesions, itching, burning sensation, ↓ freq., vulvar bleeding
Ix: biopsy
Mx: surgical resection (radical vulvectomy), radiotherapy, chemotherapy
Vaginal Carcinoma (R3)
Malignancy of the inner female genitalia (posterior third of the vaginal wall)
Predominantly occurs in postmenopausal women
Poor prognosis
RF: HPV infection, smoking, vaginal dystrophy/neoplasia
Sx: vaginal lumps/lesions, itching, burning sensation, ↓ freq., vaginal bleeding
Ix: biopsy
Mx: surgical resection, radiotherapy, chemotherapy
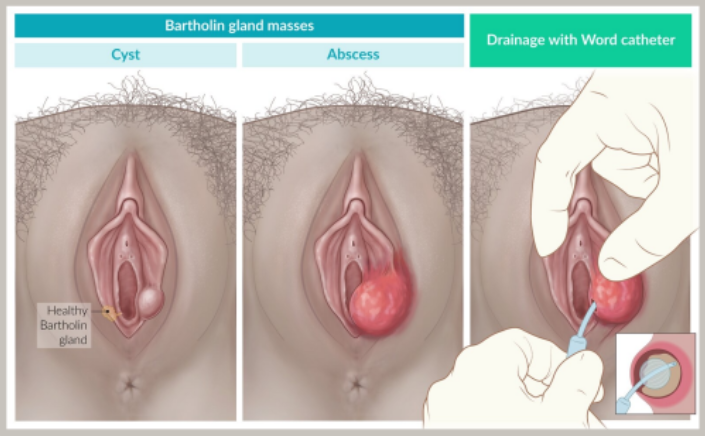
Vulval/Vaginal Cysts (R3)
Fluid or pus-filled lumps forming on/near the external genitalia or vaginal walls
Types:
Bartholin Cyst: mucus-producing Bartholin glands on inner sides of labia become inflamed/blocked, causing swelling, cyst and abscess (Mx = incision/drain)
Vaginal Inclusion Cysts: most common type of vaginal cyst, typically caused by trapped skin tissue (epithelium) following childbirth injuries or surgery
Epidermal & Sebaceous Cysts: Often found on the vulva, formed when oil-producing sebaceous glands or hair follicles become blocked
Gartner’s Duct Cysts: Form on the vaginal walls from remnants of embryonic development (the Müllerian or mesonepheric ducts)
Lichen Sclerosus (R3)
Chronic inflammatory skin condition predominantly affecting the vulva and anus and is associated with pruritus, pain, and dyspareunia
Can lead to scarring/malformation and ↑ risk of malignancy
Common Signs/Sx: itching, white paper-like skin, figure-8 around vulva
Lichen Planus (R3)
Idiopathic pruritic inflammatory disease affecting the skin, hair, nails, and mucous membranes, usually self-limiting in nature
Affects vulva, vagina and can be found orally
Characterised by pain, vaginal bleeding and discharge