total hip and knee arthroplasties and effects of anesthesia
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
joint arthroplasty indications
- no absolute age or weight restrictions
- based on person's pain and disability
- may be recommended if the person has: pain that limits everyday mobility, pain that is constant, failed conservative treatment
causes of joint pain/dysfunction
- OA
- RA
- post traumatic arthritis
- avascular necrosis hip
- childhood disease hip
- trauma/injury
goals of surgery
- relieve pain
- maintain or improve joint function/ROM
- improve quality of life
HIP
- total hip arthroplasties
- hip hemiarthroplasty
- hip resurfacing
- total hip revision
- ORIF
THA
- head of femur and a layer of the hip socket are removed
- a metal ball and stem are inserted in the femur and a plastic socket is placed in the enlarged pelvis cup
modular system components and materials
- cup
- liner
- head
- femoral stem

cemented
- used of cemented increases with age
- prosthesis fixated with cement
- provides immediate stability
- increased initial weight bearing orders
- generally used for older/less active patients
- also with patients with poor bone regneration
- disadvantage: loosens over time and with activity
cementless or press fit
- prosthesis have a porous metal coat on contact surfaces with a chemical to promote bony ingrowth
- may have decreased weight bearing status (PWB, TTWB)
- generally used on younger, more active populaiton
- patients with good bone regeneration
- less chance of loosening from wear
hybrid
- non-cemented acetabular component with cemented femoral prosthesis
- WB status per MD
risks and complications of THA
- DISLOCATION
- heart attack
- stroke
- PE
- DVT
- infection
- hematoma formation
- heterotypic ossification
- nerve injury
- fracture
- aseptic loosening
- change in leg length or apparent change in leg length
precautions to avoid dislocation risk based on surgical approach
- accessing the joint
- anteiror
- anterolateral
- lateral
- posterior
- posterolateral
posterior approach to THA
- most traditional and commonly used in US
- increased visibility for the surgeon
- requires splitting of the gluteus maximus and detachment of the external rotators
avoiding dislocation posterior approach
- no hip flexion beyond 90 degrees
- no IR past neutral
- no hip adduction past neutral
activity restrictions posterior dislocation approach THA
- avoid sitting on low surfaces
- no sleeping on operative side
- no turning on or towards the operated limb
anterior approach to THA
- continues to gain popularity
- smaller incision (restricted view of the hip joint)
- muscle sparing no detachment of muscles or tendons
avoiding dislocation anterior approach
- no hip extension
- no ER
if trochanteric osteotomy -
- no hip extension
- no ER
- no active/active-assissted hip abduction
activity restrictions to avoid dislocation anteiror approach THA
- avoid hip motion into prohibited ranges based on dislocation precautions dictated by the surgeon
- no sleeping on operative side
- no rotating on the operated limb
risk of dislocation
- <1-4% risk
- high risk in early rehab
- 6-8 weeks with clearance
signs of dislocation
- report sudden onset of pain in the hip and groin with snapping feeling
- leg shortening with either IR/ER
- unable to perform ROM
- unable to walk or weight bear on the leg
advocates for anterior approach
- lower pain levels post op
- faster functional recovery/more ADL potential
- lower dislocation risk
- shorter hospital stay
disadvantages to anterior approach
- longer procedure
- more demanding (steep learning curve - restricted view of hip joint)
- may not be appropriate for obese or very muscular patients (harder for surgeon to access joint)
- potential delay in incision healing
- some studies show higher surgical blood loss and fracture
- may be a reflection of. MD experience
advantages of lateral approach
- smaller incision
- good cup positioning --> decrease dislocation risk
- less sciatic nerve involvement
disadvantages of lateral approach
- superior gluteal nerve
- HO
- increased risk of antalgic gait (glute med, vastus lateralis)
posterior vs anterior vs lateral approach long term results
- no significant difference in clinical benefit in regards to pain, function, gait mechanics
indications for hip hemiarthroplasty
- performed when there is damage only to the femoral portion of the hip joint
- primarily frail elderly patients
- fractures involving the ball or displaced fracture of the femoral neck
- 10% of all hip arthroplasties
- unipolar vs bipolar prosthesis
- requires movement precautions
hip resurfacing
- 1% of hip procedures
- cemented femoral stem
- cementless press-fit acetabular cup
- conserves femoral bone
- caution with weight bearing, hip dislocation precautions may be warranted
hip revision types
- primary total joint replacement vs total joint revision
hip revision
- 10%
- performed due to damage of the joint from complications or normal wear and tear/life of the prosthesis
- complications from surgery same as with THA, higher risk of complications
prognosis of primary THA
- good to excellent results
- success reported to be greater than 95% for 10 year survival, can be much longer
prognosis of hemiarthroplasty
- bipolar with better outcomes than unipolar
hip resurfacing prognosis
97% survivorship at 8 years
Open Reduction Internal Fixation (ORIF) of the femur is
- NOT THE SAME as hip arthropasties
- 2 part surgery (broken bones reduced, hardware holds together)
- THA precautions do NOT apply
goals of rehabilitation post THA
- should begin day of or day after the surfery
- early post-op physical therapy is focused on functional mobility training, education, strengthening of hip musculature
education post hip replacement
- movement precautions and activity restrictions with mobility
- positioning
- encourage use of operated limb with functional activities
- signs/symptoms of complications
- handouts
exercise progression for hip
- deep breathing and anti-embolism exercises
- isometric quads and glutes (sub maximal)
- progress with prom --> prom --> prom quad activation in supine and sitting
- avoid straight leg raise
- progress to active, gravity only, hip flexion, abduction, extension OOB, as movements increase within precautions
- advanced strengthening programs with progressive resistive exercises (later phases and/or if cleared sooner)
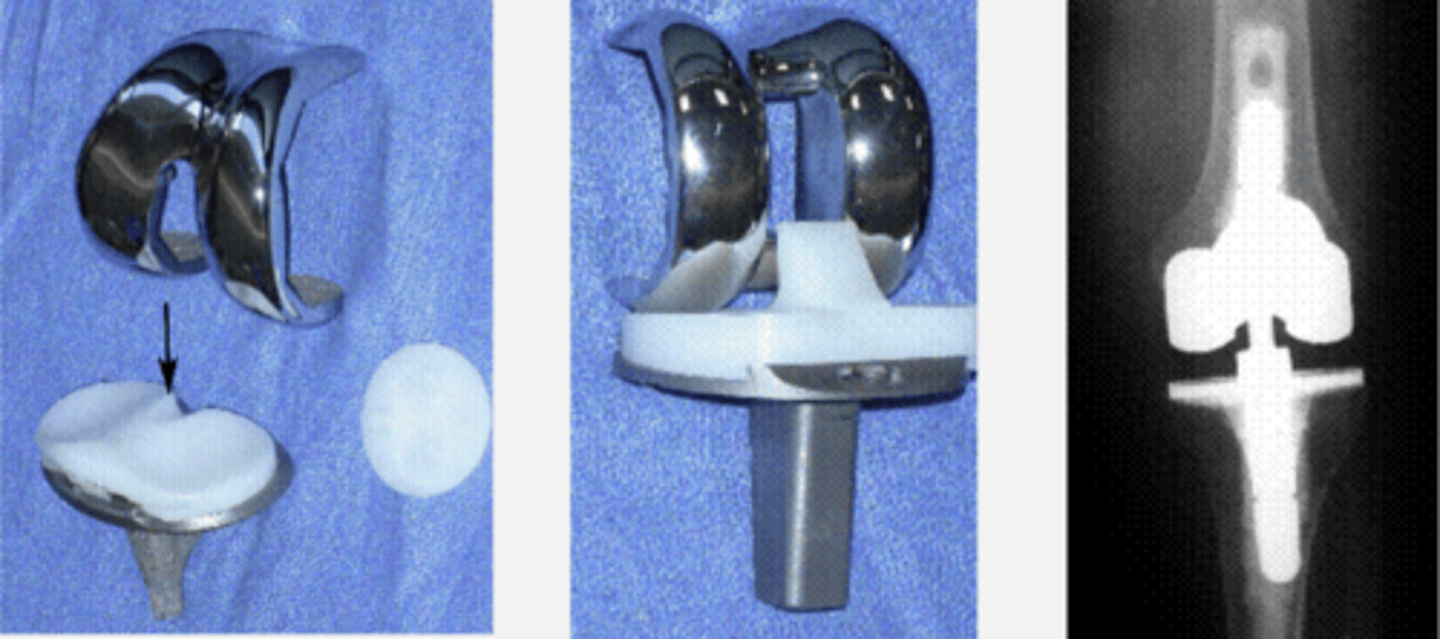
total knee arthroplasty
- femoral condyles, tibial articulating surfaces and dorsal surface of patella replaced
- cemented, uncemented, or hybrid
- weight bearing per MD
- any additional procedures may impact PT with ROM limits (lateral reticular release)
TKA design
- cruciate-retaining
- cruciate - substituting
- hinged
- fixed bearing
- mobile bearing
minimally invasive TKA goal is to decrease
- tissue injury
- post op pain
- blood loss
- length of stay in hospital
- time for recovery/rehab
disadvantages/complications of minimally invasive TKA
- not used for complex joint replacements or revisions
- potential for Mal-aligned components
- limited research
partial knee arthroplasty
- medial compartment: medial femoral and tibial condyles
- lateral compartment: lateral femoral and tibial condyles
- anteiror compartmnet: patellofemoral
- conservative treatment if area of damage is confined
- spares cruciate ligaments
- normal kinematics of the knee is preserved
- most will eventually need an TKA secondary to continued degeneration
- WB per MD
total knee risks and complications
- heart attack
- stroke
- PE
- DVT
- infection
- nerve injury
- fracture
- joint instability
- component failure/loosening
- patellar tendon rupture
- patellofemoral instability
- INADEQUATE ROM
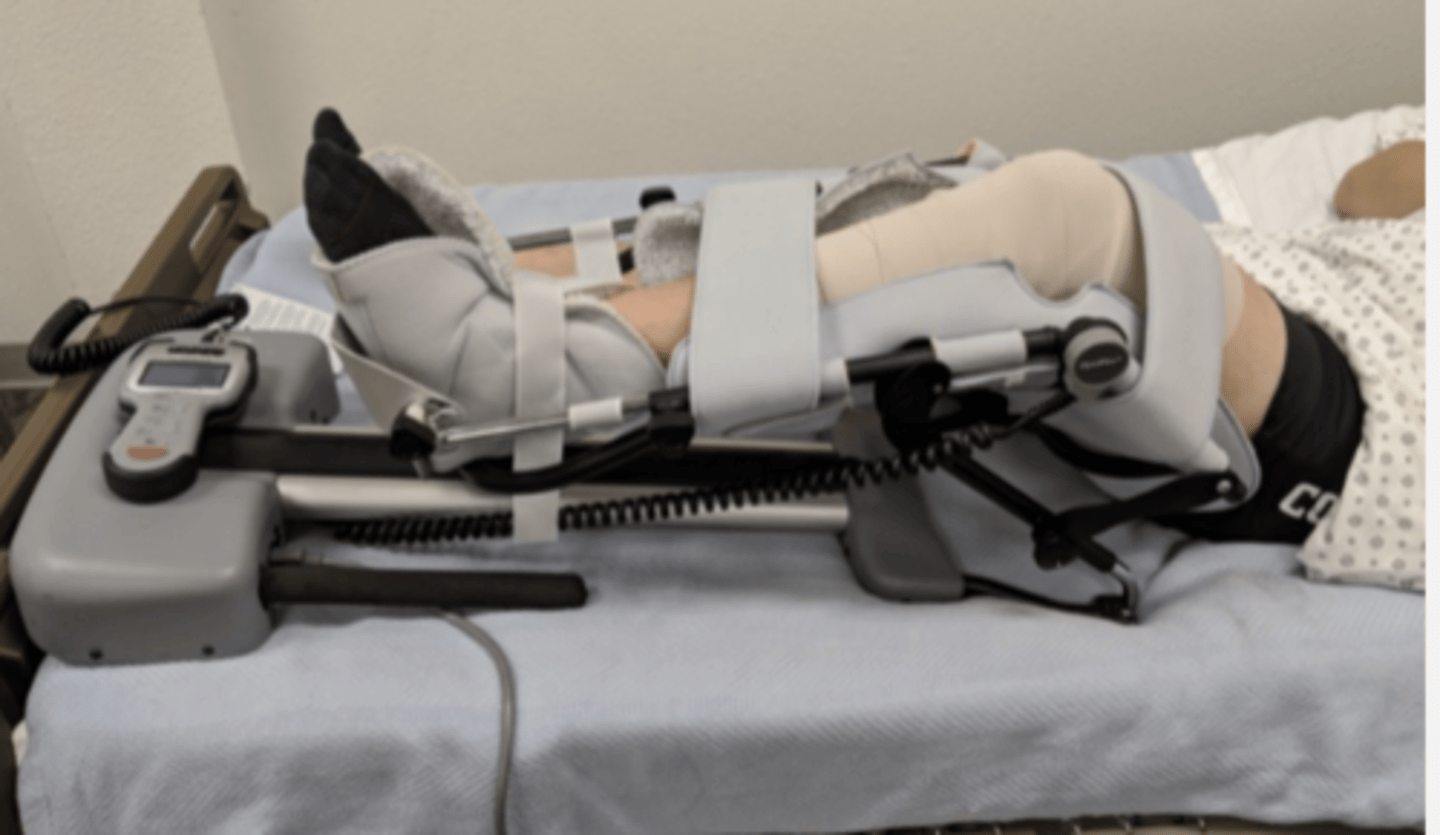
continuous passive motion machine CPM
- fit to patient's leg length
- initial setting usually 0-40 degrees
- to patients tolerance
- generally increase 10 degrees per day
- 6-8 hours/day
- needs to be watched for proper positioning
exercise progression for knee
- deep breathing and anti-embolism exercises (ankle pumps)
- isometrics for: gluteal, quad, and hamstring muscles in spine
- progress to aarom--> arom supine, sitting and standing
PROM, AAROM, AROM: exercise progressions or knee
- knee extension and flexion (heel slides, short arc quads, long arc quads)
- gentle stretching at end range within limits of pain in supine and sitting
- avoid tension at surgical site
- aarom --> arom straight leg raise
- hip abduction and adduciton
manipulation under anesthesia
- intervention for stiff knee (arthrofibrosis)
- focuses on gaining ROM (FLEXION)
- performed within the first 3 months post surgery
- research showing earlier decisions regarding ROM concerns may be more beneficial
manipulation under anesthesia ROM linked to functional activities:
- 93 degrees flexion (rise from a chair)
- 85-90 degrees (stair negotiation)
- 106 degrees (tying a shoelace)
- 125+ degrees (high level activities including squatting)
- goal: maximize ROM to 120 degrees as close to 0 degrees extension
bilateral total knee arhtroplasties
- places increased stress on cardiovascular system
- under the age of 70
- requires person to be fit with overall good strength and have good functioning cardiac, pulmonary and circulatory systems
benefits of B TKA
- one hospital stay (less expensive)
- one surgery (less anesthesia)
- ideally, total rehab process is shortened
- high importance on positioning and home set up
TKA prognosis
- 78% TKAs last 20 years
- >90% TKAs last for 10 years
- 90% have reduction in knee pain and improved ability to perform ADLs
goals of rehab post tKA
- should begin within 24 hrs post op
- improving knee ROM and strength
- exercise program
- positioning and edema control
- motor function training
- maximizing independence and safety with all mobility activities
education post knee surgery
- joint protection strategies
- no pivoting on the operated knee
- positioning of operated leg prior to sit/stand
- positioning in bed
- usual thought: no pillow under knee, avoid hip ER