MEDL350L Urinalysis Exam #1
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
Basic functions of kidneys (1-2)
filtration: remove waste & toxic byproducts of metabolism;
function of glomerular capsule & capillaries; requires endothelial, mesangial, & epithelial cells
chem modification & concentration of filtrate: Retention or excretion of most of the filtered salts (ex: Pi, HCO3-) & water
function of renal tubules (epithelial cells)
Basic functions of kidneys (3-5)
Endocrine organ: Oxygen sensing & secretion of EPO to maintain RBC
Renin to maintain water & Na+ balance
Vitamin D activation (tubular epithelial cells convert precursor to active form)
Water conservation and blood pressure balance
Acid-base balance
Nephron: Compromised on, # of nephrons, avg adult output
comprised of many epithelial & endothelial cells
average adult kidney contains 1,000,000 nephrons
normal adult urine output = ~800-1,200 mL/day
Compulsive water drinkers & individuals with polydipsia may increase
Lithium, ethanol, diuretic medications and caffeine can increase
Renal function & Cardiac function: Cardiac output, low BP, HTN & DM
Kidneys receive 25% of cardiac output, filtration is driven by high arteriolar blood pressure (BP)
Low BP perfuses the kidney inadequately & is a cause of acute kidney failure
Hypertension and DM (diabetes) are leading causes of chronic kidney
disease
Renal function: Filtration (glomerulus, PT, plasma proteins that can be filtered)
contains a glomerulus enclosed in a capsule, tubules & associated peritubular capillaries
Cell-free filtration of small molecules in plasma occurs in the glomerulus where 20% of the plasma water and content is filtered into the proximal tubule (PT)
Plasma proteins < 60 kDa are filterable, but neg charge repulsion between 60 kDa albumin & 3 filtration barriers prevents most from entering the PT
Renal function: Filtration (pos charged plasma proteins, filtrate modification, small filtered proteins)
Smaller and more pos charged plasma proteins are freely filtered
Filtrate enters tubules → chemically modified: 99% of water & Na+ are reabsorbed, with other electrolytes and glucose
Small filtered proteins & glucose are catabolized inside tubular cells
Renal function: Capillary anatomy, salts reabsorbed, DT
Juxtaposition of peritubular capillaries is important anatomical feature: H2O & salt can easily pass & balance
Most salts are reabsorbed constitutively from PT & LOH
DT adjusts, or “fine tunes,” excretion or retention of salts depending on need
3 Filtration barriers in glomerulus
Fenestrated endothelial cells prevent passage of cells into filtrate & make for a more highly permeable barrier than ordinary capillaries
Basement membrane (GBM) beneath endothelium is enriched in non-linear type 4 collagen in a “pickup stick” array
Epithelial cell projections (foot processes) wrap around GBM → filtration slits in “curving waterslide” – enriched in a transmembrane protein (nephrin & podocin) mesh
Glomerulus: Podocytes
primary arms & secondary projections (pedicels or foot processes) wrapping around glomerular capillaries
projections interdigitate to form narrow filtration slits
Filtration barriers in glomerulus: Neg/Pos Charges
High density of neg charge in all 3 layers: Repels neg charged RBC, WBC, PLTs and many plasma proteins
in healthy kidney: proteins that are highly neg charged & large (> 60kDa) are unlikely to pass through filtration barriers
Example: albumin (>200 negative charges/molecule)
Proteins that are small (<60 kDa), which carry neutral or pos charge are filtered & catabolized in tubular cells
Glycation
as seen in Diabetes Mellitus
diminishes neg charge in barriers & allows passage of albumin into filtrate: diabetic nephropathy/proteinuria (microalbuminuria/macroalbuminuria)
Albuminuria is a predictor of kidney disease progression and vascular disease in individuals with DM
MESANGIAL CELLS
close contact with the glomerulus, and are responsible for keeping them in the right conformation
can cause contraction or movement of the glomerulus
Renal function testing: Creatine, PCr storage, PCr potential
measurement of the filtration marker creatinine in plasma and urine, a spontaneous, non-catalyzed decomposition product of creatine (Cr) & creatine phosphate (PCr)
Creatine phosphate (PCr) is synthesized & stored in skeletal muscle using energy from ATP hydrolysis
PCr has a higher phosphate transfer potential than ATP and is used to quickly recharge ADP (conversion to ATP) in exercising & exhausted muscle
Renal function testing: Cr produce rate, Cr circulating levels, Cr indicator, Increases in circulating Cr
Creatinine is produced at a steady state rate
Circulating levels depend on an individual’s muscle mass & the renal filtration rate
A reliable index of filtration, creatinine is an indicator of the number of functioning nephrons in the kidney
Increases in circulating creatinine are seen when ≤ 50% of functional nephrons or nephron activity is lost
Creatine kinase (CK/CPK)
catalyzes the reversible conversion of creatine and creatine phosphate
CK has the highest activity in brain, skeletal and cardiac muscle and moderate activity in smooth muscle and other organs
Laboratory Estimation of the GFR (Glomerular Filtration Rate): Collection, define renal clearance, ideal marker of filtration
requires 24-hour urine collection
Renal clearance is defined as the volume of plasma that must flow through the kidneys/minute to completely remove a substance from circulation
Ideal marker of filtration or clearance should:
be freely filterable (e.g., not protein-bound like calcium)
not be further metabolized (metabolic end-product)
be produced at a steady state level
not be secreted by tubules
Laboratory Estimation of the GFR (Glomerular Filtration Rate): Cr plasma, urine, and clearance RR
Plasma creatinine level meets ¾ criteria for an ideal clearance marker
Plasma creatinine reference range: 0.5-1.5 mg/dL (lower in children)
Urine creatinine RR: 20-275 mg/dL ♀ / 20-320 mg/dL ♂
Creatinine clearance RR: Male: 97 to 137 mLs/min, Female: 88 to 128 mLs/min
Calculated formulas of GFR (eGFR): Sample used, normal Cr clearance value, filtration marker
use plasma creatinine and/or cystatin C & doesn’t require 24-hour urine collection
Calculated creatinine clearance is normal if > 60 mL/min
novel filtration marker:
Cystatin C is a cysteine protease inhibitor produced primarily by all nucleated cells
Due to low molecular weight and positive pI, (+ charge) it is easily filtered
serum concentration is independent of gender, age, or muscle mass
Glomerular Filtration Rate (GFR) & Creatinine Clearance formulas
UV/P (U = urinary Cr in mg/dL; V
Renal clearance: Renal plasma flow (RPF): Define, 20% RPF, RR
volume of plasma that passes through the glomeruli in both kidneys in one minute, normally 625 mL/min
20% of RPF is normally filtered per minute (125 mL/min) using the ideal filtration marker inulin
Renal clearance of creatinine is approximately 100 mL/min
This value = 100 mL of plasma is completed cleared of creatinine every minute in an individual with healthy kidneys
Renal clearance: Cr secretion, marker for filtration, rate of Cr/PCr decomposing
Cr can be secreted directly into the filtrate by the tubules → secretion quickly reaches a saturation point → not considered to have a significant effect on filtration
Perfect marker of filtration = inulin; It has to reach steady state by IV infusion → clinical use impractical
Rate at which Cr & PCr spontaneously decompose into creatinine is a physical constant, making for a steady state production without the need to infuse a xenobiotic
Water & Sodium balance: MD function & decreased [NaCl]
Macula Densa (MD) is a component of the distal tubule (DT) that senses NaCl concentration delivery
Decreased [NaCl] delivery drives MD to release prostaglandins:
Dilate afferent arteriole decreasing resistance, increasing capillary hydrostatic pressure & GFR
Increase renin release from the JGA, eliciting aldosterone secretion from adrenal cortex in the “RAAS.”
Aldosterone, a mineralocorticoid increases the rate of K+ excretion and Na+ retention by the DT
Net effect is to increase sodium and water retention, increasing BP
JG cells sense stretch via baroreceptors, decreased BP, increases renin secretion independently of MD
Water & Sodium balance: Increased [NaCl], net effect, autoregulatory mechanisms
Increased [NaCl] delivery to the MD results in vasoconstriction of afferent arteriole, decreasing GFR and renin secretion
Net effect is to decrease sodium and water retention, decreasing BP
Autoregulatory mechanism helps regulates balance of water, Na+ & BP, keeping GFR constant in the context of variable arterial pressure
Renin-Angiotensin-Aldosterone Axis (pathway & results)
BP decreases → kidney produces Renin → Renin activates Angiotensinogen to Angiotensin I → Angiotensin-converting enzyme (ACE) converts to Angiotensin I to II → Angiotensin II activate pituitary to produce Aldosterone → Aldosterone acts on kidney for Na+ retention → BP rises (vasoconstriction)
results: increased sympathetic drive, Na+ & H2O retention, vasoconstriction/increased BP, Anti-diuretic hormone secretion (H2O retention)
ACE Inhibitors & Angiotensin II receptor blockers
inhibitors (Lisinopri) & blockers (ARBs; Losartan) are typical first choices in treating hypertension (HTN)
Calcium channel blockers, beta-adrenergic blocking agents and older agents (various diuretics which can either be Ca or K) wasting or sparing are also used in treating volume overload and HTN
Aldosterone-to-Renin ratio (ARR): Function, potent, type of activity, secretion stimulated by
Aldosterone increases the rate at which the kidney tubules dump K+ into the urine & rate at which Na+ is moved from the filtrate back into circulation
Aldosterone is the major, most potent mineralocorticoid
Cortisol also has mineralocorticoid activity
Aldosterone secretion can be stimulated by ATII, & independently by hyperkalemia
Aldosterone-to-Renin ratio (ARR)
ARR is calculated as the aldosterone to renin activity (A/R) ratio
Informative in differentiating primary from secondary hyperaldosteronism (HA)
Clinical signs of HA are an inappropriately high circulating level of aldosterone → low plasma K+ & (ECG) cardiac conduction abnormalities
Plasma Na+ is usually not affected in HA since there are Atrial Natriuretic Factors (ANFs) in the heart
ANFs = hormones that respond to increased stretching of the atria, powering the dumping of sodium into the urine when it’s elevated
The ANFs offset the hypernatremic effect of aldosterone
Aldosterone-to-Renin ratio (ARR): Primary hyper- caused by & Secondary is caused by
Primary hyperaldosteronism is caused by an adrenal adenoma secreting inappropriately high levels of mineralocorticoid → hypokalemia
Hyperaldosteronism may be secondary to decreased arterial perfusion/pressure to the kidney in heart failure, or to congenital/acquired conditions that narrow the renal arteries (stenosis), as renin secretion is provoked in response → HA
Aldosterone-to-Renin ratio (ARR): Primary vs Secondary Aldosterone & Renin
Primary HA: Elevated aldosterone → increased movement of Na+ from the filtrate back into circulation → raising blood pressure.
Increase in BP is sensed by the heart and kidney → renin release is suppressed (classical negative feedback loop)
Secondary HA: Renin is likely continuously secreted due to vascular/cardiovascular problems → decreased blood flow to the kidney
Negative feedback effect is chronically dampened in the setting of low perfusion
Aldosterone-to-Renin ratio (ARR): Primary vs Secondary HA ARR
ARR is higher in primary HA
ARR ratio is lower in secondary HA
Licorice intoxication
Renal Water Balance
Angiotensin II induces secretion of antidiuretic hormone (ADH or arginine vasopressin) from posterior pituitary
ADH recruits water channels (aquaporin-2) to the apical membrane of connecting tubules and collecting ducts in the late (distal) nephron
Aquaporins allow for free passage of water from the filtrate back into circulation
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH): Etiology, ADH secretion, result effects
etiology: Paraneoplastic syndromes (ex: ectopic ADH secretion from small cell lung cancer cells, medication, etc.)
Characterized by excessive ADH secretion → Too much water moves into vascular space
Dilutional hyponatremia & increased urine osmolality (can use serum not plasma)
Central Diabetes Insipidus (DI): Etiology, ADH secretion, result effects, test
etiology: head injury, brain trauma, radiation therapy, severe illness
not enough of ADH is secreted → H2O lost via inability of kidney conservation
Extreme thirst, copious & dilute urine (up to 20 L/day), hypernatremia decreased urine osmolality, increased serum osmolality
Overnight water deprivation test (must be done in hospital) shows inappropriately dilute urine next morning
pituitary issues
Nephrogenic Diabetes Insipidus (DI)
ADH resistance: inherited or acquired defects in vasopressin type-2 receptor or aquaporin-2 genes → ADH insensitivity
inherited/acquired
Reagent test strips/”Dipsticks”
CLIA waived test
QC materials mandatory: Normal/ abnormal lyophilized human urine
document: QC/QA & Date reagent opening & expiration
test strip readers (better standardization)
Diagnostic sensitivity formula
TP / (TP + FN)
Test strips: Leukocytes (chromogen, normal, sensitivity/specificity, rule out, methodology)
Chromogen is converted to a colored product by a neutrophil protease (esterase)
normal = neg
Sensitivity for UTI is poor (< 50%) & Specificity is better
Better used to rule out UTI
Methodology: Enzyme catalyzed colorimetry
Test strips: Nitrite (detects, normal, sensitivity, methodology)
Detects nitrate reduction by gram negative bacteria such as E. Coli, Klebsiella, Proteus, & Enterobacter
normal = neg
Sensitivity (alone) for UTI < 30%
Methodology: Greiss reaction: nitrite diazonium formation, colorimetry
(Test strips) Urobilinogen: Define, parallels, decreases associated with, normal, methodology
Metabolite of bilirubin produced by gut flora that is partially reabsorbed from GI tract and excreted in urine
Parallels increase in plasma bilirubin
Decreases associated with biliary obstruction
Normal: 0.2-1.0 mg/dL
Methodology: Ehrlich’s reagent: p-dimethylaminobenzaldehyde, colorimetry
(Test strips) Bilirubin: Parallels, increased in, normal, methodology
Parallels increase in plasma bilirubin
Increased in biliary obstruction & other causes of hyperbilirubinemia (liver disease)
Normal: none
Methodology: diazonium salt, colorimetry
Test strips: Protein (most/less sensitive to, quant/qual, typically positive, microalbumin patches
Most sensitive for the presence of abnormal levels of albumin in urine, less sensitive to immunoglobulins or Ig light-chains
Semi-quantitative
Typically positive in UTI
Microalbumin patches or measurements for detection of early diabetic nephropathy
Test strips: Protein (quant/qual, normal, methodology)
Quantitative tests from lab available for protein/creatinine ratio or 24-hour protein excretion
Normal: negative
Methodology: dye binding (DIDNTB)
Test strips: Blood (sensitive to, reactive to, confirmed by, normal, methodology)
Patch is sensitive to the presence of heme-Fe found in Hb & myoglobin
Reactive to intact and hemolyzed RBC & free Hb
Should be confirmed by PPM
Normal: none
Methodology: heme Fe oxidizes Tetramethylbenzidine; colorimetry
Test strips: pH (urine pH, acid-base balance, normal, methodology)
Normal urine is acidic but can become alkaline after meals (> 6)
Should correlate with overall picture of acid-base balance in normal, & in metabolic/respiratory acidosis & alkalosis.
Normal: 4.5 – 8.0
Methodology: 2 pH indicators: methyl red and bromthymol blue
Test strips: Specific gravity (define, measures, elevated when, deionized water, urine specific gravity, chem formula)
Sum of total solute concentration: salts, urea, other small molecules
Measures overall concentrating ability of kidney
Is elevated after water deprivation
Specific gravity of ultra-pure deionized water = 1.000
Urine is normally 1.005-1.030
RCOOH + Na+ → COONa+ + H+
Test strips: Specific gravity (<1.003, >1.010, place in context, refractometer is sensitive to, reagent methodology)
< 1.003 is probably not urine
> 1.010 reflects concentrated urine
Place in context of dehydration and water imbalances such as diabetes insipidus, SIADH, etc.
Refractometer is sensitive to glucose, contrast materials, dipstick is not
Reagent methodology relies on change in pKa of a polyelectrolyte, dissociation of H+ in presence of pH indicator
Test strips: Ketones (quant/qual, increased in, normal, methodology)
Semi-quantitative
increased in carbohydrate starvation; keto-acidosis
normal = neg
methodology: Na nitroprusside colorimetry
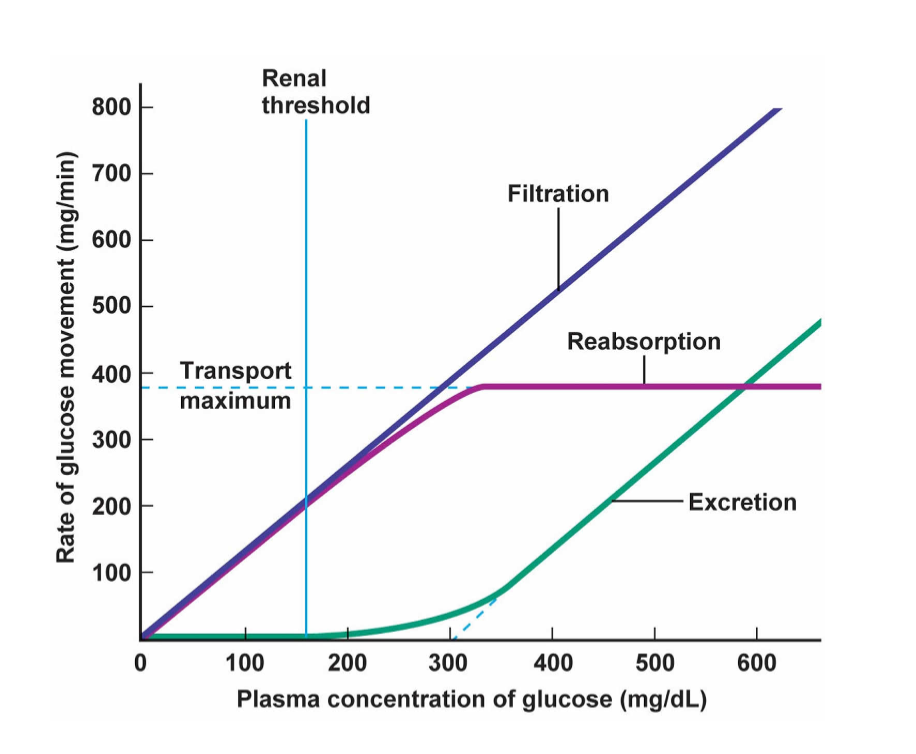
Test strips: Glucose (quant/qual, specific for, normal, methodology)
Semi-quantitative; specific for glucose above renal threshold of glucose excretion; diabetes mellitus (DM)
normal = neg
methodology: glucose oxidase reaction produces peroxide which reacts with chromogen
Proteinuria
Most plasma proteins are neg charged at pH (7.40) & are electrostatically repelled from the filtration barriers which carry a high density of neg charge
The smaller (< 60 kDa) & more pos charged a plasma protein is → more likely it is to be filtered by the glomerulus & catabolized by renal tubular cells (RTCs)
Albumin is small enough to be filtered but carries > 200 negative charges ay physiologic pH
A very small amount of albumin & other proteins (Tamm-Horsfall protein) can be detected in normal urine.
Proteinuria: Normal value in 24hr urine, glycation of proteins in DM, 30-300 mg/day, >300 mg/day, nephrosis
norm value in 24 hour urine = < 150 mg/day total protein, < 20mg/day albumin
Glycation of the proteins in the filtration barriers in DM diminishes the electrostatic repulsion of albumin & other proteins → progressively increasing their excretion
30-300 mg/day = moderately increased albuminuria (microalbuminuria) = increased risk for CV disease
> 300 mg/day = severely increased albuminuria, overt proteinuria (macroalbuminuria)
Nephrosis: > 3.0 g of protein excreted per day
Proteinuria: Protein/creatinine ratio, nephrosis, normal protein/creatinine ratio, ratios >3.5 mg/mg
Urine protein/creatinine ratio (Spot 1st or 2nd void):
Nephrosis: > 3.0 g of protein excreted per day
Normal urine protein-to-creatinine ratio is less than 0.2 mg/mg
Ratios greater than 3.5 mg/mg are in the nephrotic range for proteinuria
Renal glucose threshold (RTg)
Glucose is filtered and reabsorbed by renal tubular cells within its normal circulating concentration (<100 mg/dL)
Threshold for urinary excretion of glucose is plasma glucose > 180 mg/dL as this concentration exceeds the rate of reabsorption
RTg may be higher in those with DM
Renal glucose threshold (RTg): Gliflozins (define, effective in, Empagliflozin, adverse effects)
Medications that inhibit sodium-glucose cotransporter 2 (SGLT2) in the proximal tubule (PT), which reabsorbs 90% of filtered glucose
Effective in lowering glucose levels in individuals with T2DM and treating heart failure & CKD.
Empagliflozin = Jardiance
Adverse effects: Ketosis, UTI, Yeast infections, Fournier’s Gangrene
Normal Urine sediment: Squamous epithelial cells (arise from, normal value, increases in, clue cells, subjective call)
SECs arise from lower urinary tract (skin, urethra)
Normally ≤15-20/hpf (400X)
Increases in UTI, infection, inflammation of lower urinary tract
Clue cells: speckled SECs found in some forms of bacterial vaginosis: Gardnerella vaginalis
Subjective call: fishy smell of sample may be better “clue”
Normal Urine sediment: Hyaline casts (morphology, formed in, normal value, increased in)
Transparent, translucent & cigar-shaped
Formed in distal tubules (DT) in matrix of Tamm-Horsfall protein
Normally ≤5/lpf (100X)
Increased numbers seen in dehydration, urinary stasis & illness
Normal Urine sediment: Harmless crystals (hyaline casts, Ca oxalate, uric acid)
Hyaline casts: more than a few = considered to be abnormal
Calcium oxalate: Maltese cross, envelope (vegetable source) – “stone former”
dihydrate = octahedral
monohydrate = dumbbell-shaped
Uric acid: amorphous or football-shaped (purine end-product)
Urine pathological findings: RBCs (morph in older urine, increased in, chronic & painless hematuria)
Puckered (crenated) appearance in older urine
Increased in UTI and by strenuous exercise (marathon running, e.g.)
Chronic and painless hematuria requires cystoscopy
Urine pathological findings: WBCs (morphology, urinary eosinophil)
Grainy, granular surface with visible nuclei
clumping and/or attached bacteria
Urinary eosinophil count for interstitial nephritis (disseminated/inflammatory reaction to medications in kideys)
Urine pathological findings: Bacteria (usual morphology, most common gram neg & pos bacterium cultured)
Usually motile rods
Most common gram-neg organisms cultured:
Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Enterobacter cloacae
Most common gram-pos organisms cultured:
Enterococcus faecalis, Enterococcus faecium, Staphylococcus saprophyticus
Urine pathological findings: Yeast & Trichomonas (yeast: usually & trich: what, must be, tests available)
yeast: Usually Candida; Urine contaminant
trich: STD & Urine contaminant
Must be swimming to properly ID n sediment
DNA level tests available
Urine pathological findings: Renal transitional epithelial cells (morphology, arise from, indicative of)
Smaller than SEC, larger than WBCs; Larger N/C ratio than SEC
Arise from renal pelvis and ureters
Indicative of more serious inflammation, infection, transplant rejection, renal cell carcinoma
Urine pathological findings: Renal tubular epithelial cells
Slightly larger than WBC; Large N/C ratio
Indicative of serious pathology: acute renal tubular toxic injury, necrosis, transplant rejection, Renal Cell Carcinoma
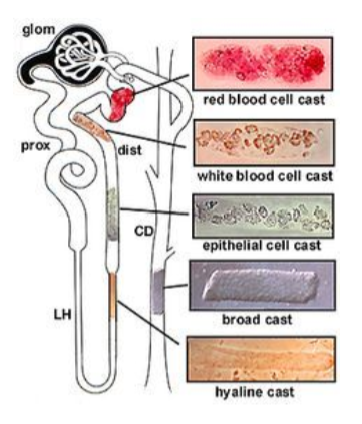
Urine pathological findings: Renal casts (hyaline, granular, RBC, WBC, cells, waxy/broad)
Hyaline, normal unless > 5/lpf
Granular: non-specific finding seen in many conditions including stress, infections including UTI, severe illness
RBC: contains RBC, Hb; seen in acute glomerulonephritis (AGN), pyelonephritis
WBC: common finding in pyelonephritis, AGN
epithelial & renal cells
Waxy or broad cast: found in end-stage renal disease, indicative of tubular necrosis
Normal crystals: Can cause, concept of pre-test, lots of crystals, lots of casts
Can cause kidney stones (especially calcium-oxalate) in those who are prone genetically, or by not drinking enough water
Concept of pre-test probability helps to guide a clinician through nephrolithiasis
If have lower flank/back pain & painful urination, & got lots of these crystals → pre-test probability is high that you have formed a stone
Like normal crystals, squamous epithelial cells & hyaline casts can be seen in a healthy person’s urine
If see more than normal → suspicion of infectious or inflammatory causes should be raised
Urine pathological findings: Pathological crystals
Aminoacidurias: disorders characterized by errors of amino acid metabolism
Calcium oxalate / calcium phosphate
Uric acid
Struvite/Triple phosphate (associated with UTI involving urease + organisms)
Urine pathological findings: Triple phosphate/struvite
Coffin lid shape
Highly associated with gram neg UTI (Urease positive organisms; Proteus but not E. coli)
More common in women than men
Common veterinary finding
Urine pathological findings: Triple phosphate/struvite
MgNH4PO4.6H20-Ca10.[PO4]6.CO3
Form in highly alkaline urine
Common finding in patients with anatomic abnormalities that lead to urinary stasis, such as congenital urinary malformations and obstruction of the ureteropelvic junction, a persistently hydronephrotic renal pelvis is also known to form struvite stones
Urine pathological findings: Triple phosphate/struvite
Also found in gross hematuria, advanced age, hypertension, fever, urinary diversion surgery, neurogenic bladder, indwelling catheters, medullary sponge kidney, distal tubular acidosis, diabetes, and low serum phosphorous levels
Staghorn calculi: Upper urinary tract stones that involve the renal pelvis and extend into at least 2 calyces
Acute renal failure (acute kidney injury)
develops over period of a few days
Tubular damage
Acute blood loss: lack of perfusion to kidneys
“Pressure pants”
Reversible
Chronic kidney disease
progressive loss of nephrons (< 50% viable) usually caused by Diabetes Mellitus & high blood pressure (hypertension)
Nephrosis vs Nephritis
Nephrosis: selective loss of protein, typically acellular urine
Nephritis: inflammatory, infectious, cellular urine featuring casts & proteinuria
Glomerulonephritides
IgA nephropathy: aka Berger’s disease, caused by deposition of IgA immune complexes in glomerulus
Goodpasture syndrome: anti-GBM autoantibody disease (anti-collagen Ig) affecting lungs & kidneys
Membranous nephropathy (glomerulonephritis)
Rapidly progressive (crescentic) glomerulonephritis
Membranous nephropathy (glomerulonephritis)
autoantibody attacks podocyte antigens: the secretory phospholipase A2 receptor, thrombospondin & others causing endothelial damage and swelling
Rapidly progressive (crescentic) glomerulonephritis
Rapid loss of renal function over a short period (days to weeks)
Nephritis: proteinuria, micro or macroscopic hematuria, dysmorphic red blood cells (RBC), RBC casts, anti-GBM antibodies
Cellular crescent formation in the glomeruli; proliferative cellular response seen outside the glomerular tuft within Bowman's capsule (crescents)
Fatal if not treated
Nephrogenic diabetes insipidus
mutations in vasopressin type-2 receptor or aquaporin-2 genes causing ADH insensitivity