WK FOUR - Diabetes (Hypo/Hyper/DKA)
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Diabetes Gender Distribution
1.3 times more common in males than females (age-controlled).
Indigenous Australian Risk
Diabetes is 3 times more common in Indigenous Australians.
Organs of the Endocrine System
hypthalamus
pituitary gland
pineal gland
thyroid gland
parathyroid gland
thymus
pancreas
adrenal gland
gonads
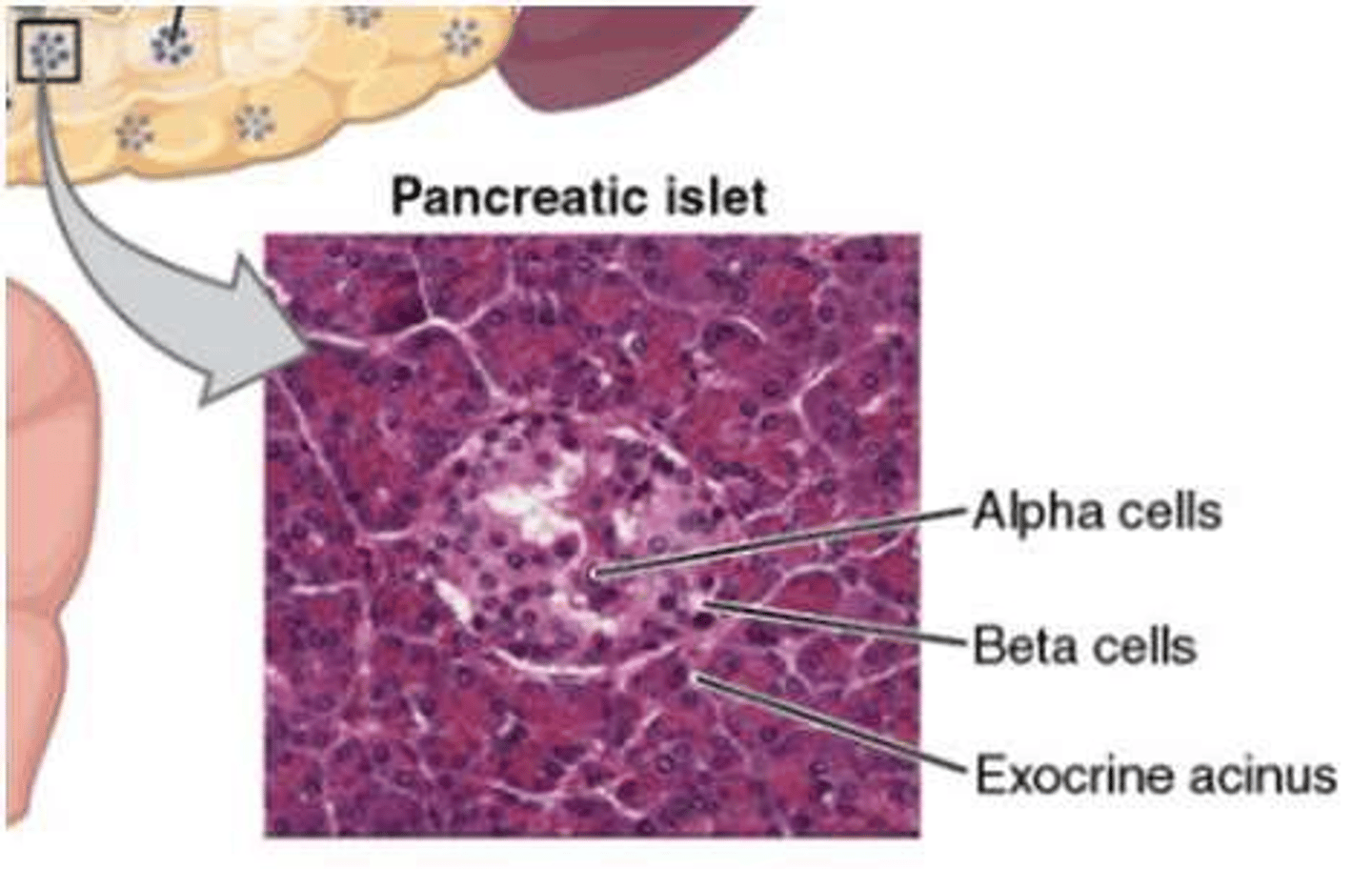
Pancreatic Acini Function
Secrete digestive fluids into the duodenum (exocrine function).
Pancreatic Islets Function
Perform the endocrine functions of the pancreas. (excrete glucagon, insulin, etc..)
Alpha Cells
Pancreatic cells that secrete glucagon.
Beta Cells
Pancreatic cells that secrete insulin.
Delta Cells
Pancreatic cells that secrete somatostatin (inhibits insulin and glucagon).
Glucose Storage Locations
Stored as glycogen in liver/muscles or triglycerides in adipose tissue.
Glucose Feedback Mechanism
Operates on a negative feedback loop sensed by pancreatic receptors.
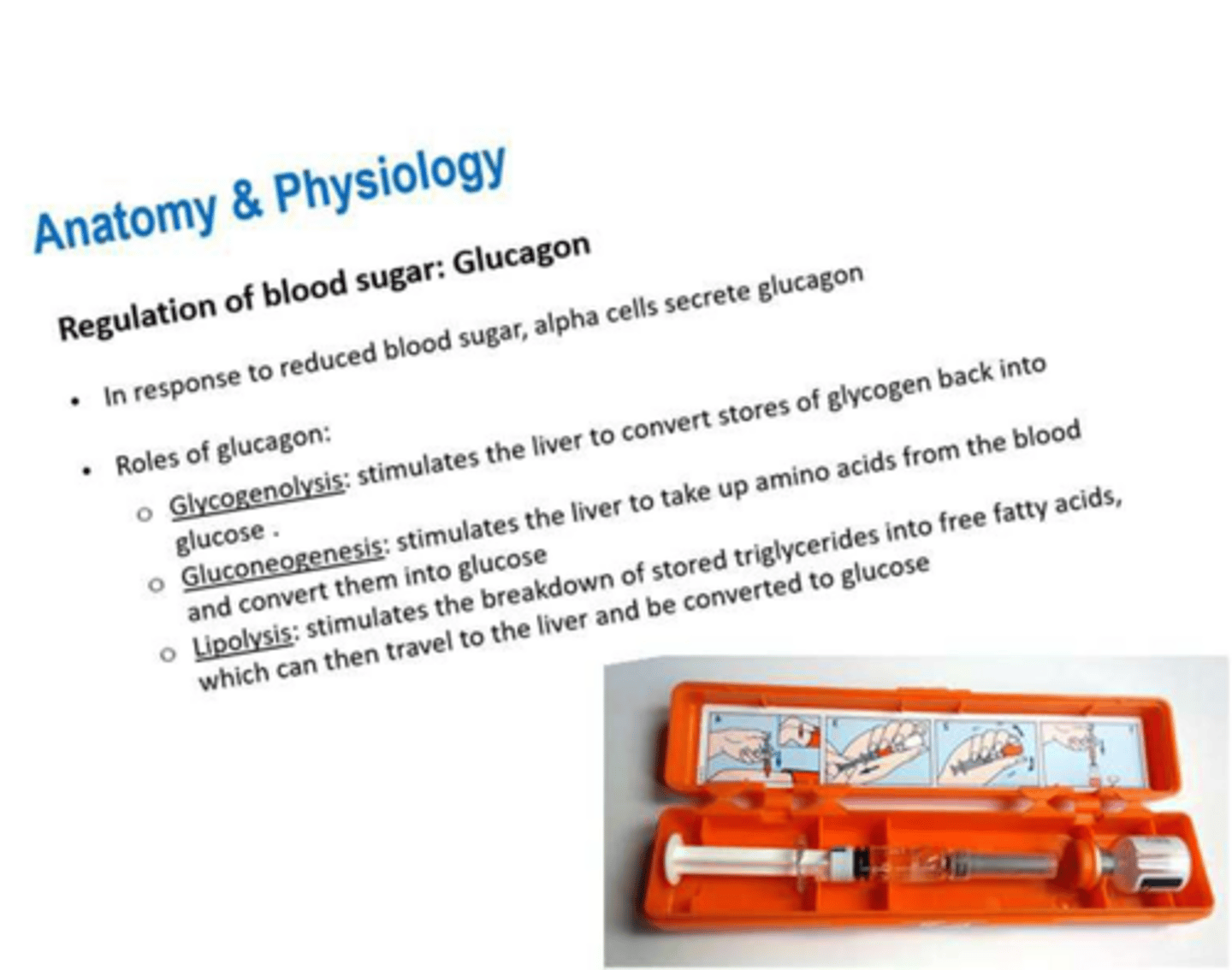
Glycogenolysis
Stimulates the liver to convert stored glycogen back into glucose.
Gluconeogenesis
Stimulates the liver to convert amino acids into glucose.
Lipolysis
Breakdown of triglycerides into fatty acids for conversion to glucose.
Blood Sugar Management Feedback Loop (Low)
A physiological mechanism that regulates blood glucose levels by signaling the release of glucagon in response to a drop in blood sugar.
Blood Sugar Management Feedback Loop (High)
A physiological mechanism that regulates blood glucose levels by signaling the release of insulin in response to a spike in blood sugar.
Insulin Role: Cellular Uptake
Facilitates glucose uptake into cells, mostly skeletal muscle and adipose tissue.
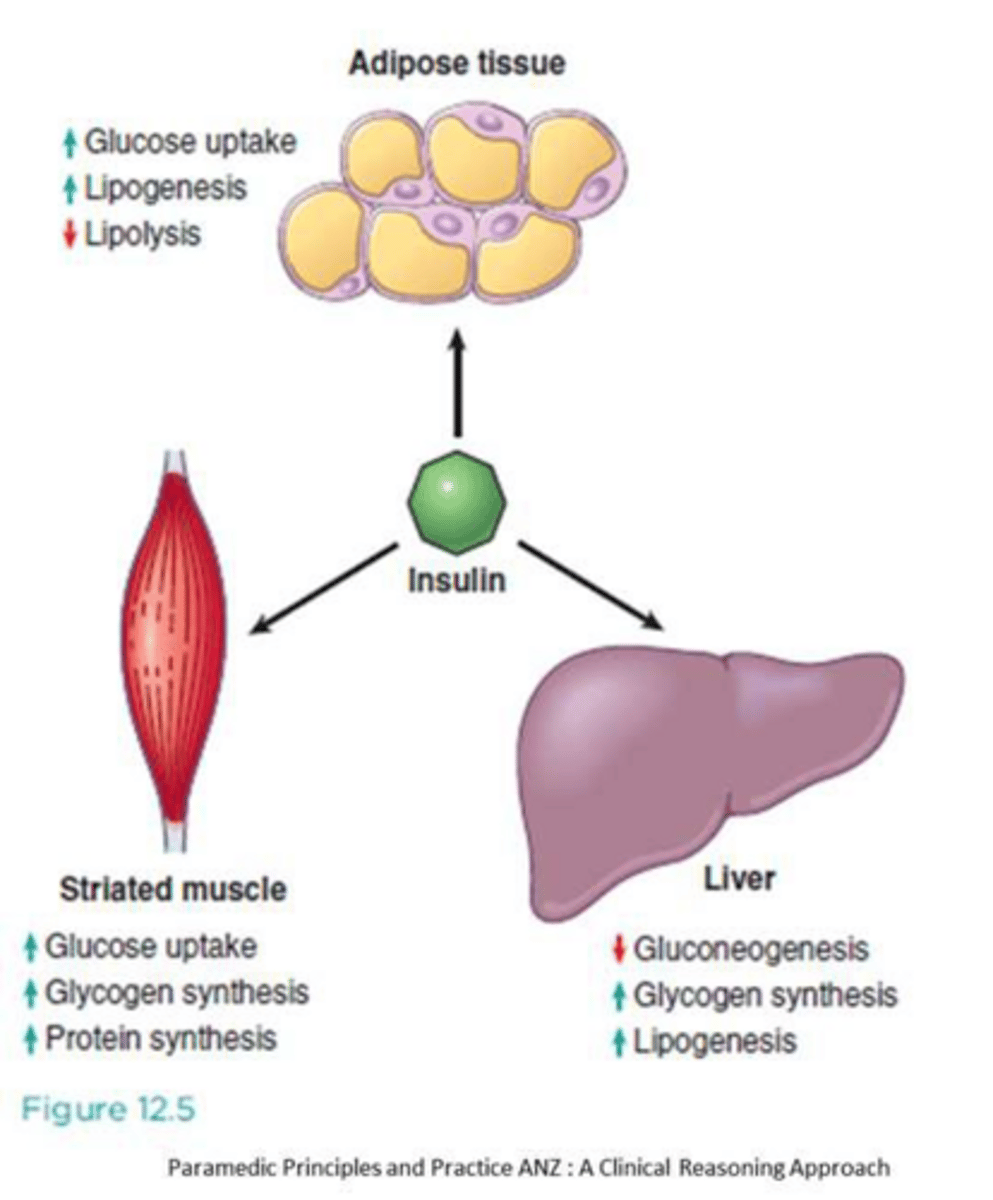
Insulin Role: Metabolism
Promotes fat, protein, and carbohydrate metabolism.
Insulin Role: Inhibition
Inhibits enzymes involved in glycogenolysis and gluconeogenesis.
Insulin Carbohydrate Metabolism
Insulin activates membrane receptors on target cells causing most body cells to become highly permeable to glucose and facilitates its conversion to glycogen for storage.
Insulin Fat Metabolism
Decreases fat utilization for energy and promotes triglyceride conversion.
Insulin Protein Metabolism
Promotes amino acid uptake for conversion into proteins (anabolic metabolism).
Diabetes Mellitus Definition
Diseases of abnormal carbohydrate metabolism characterized by hyperglycemia.
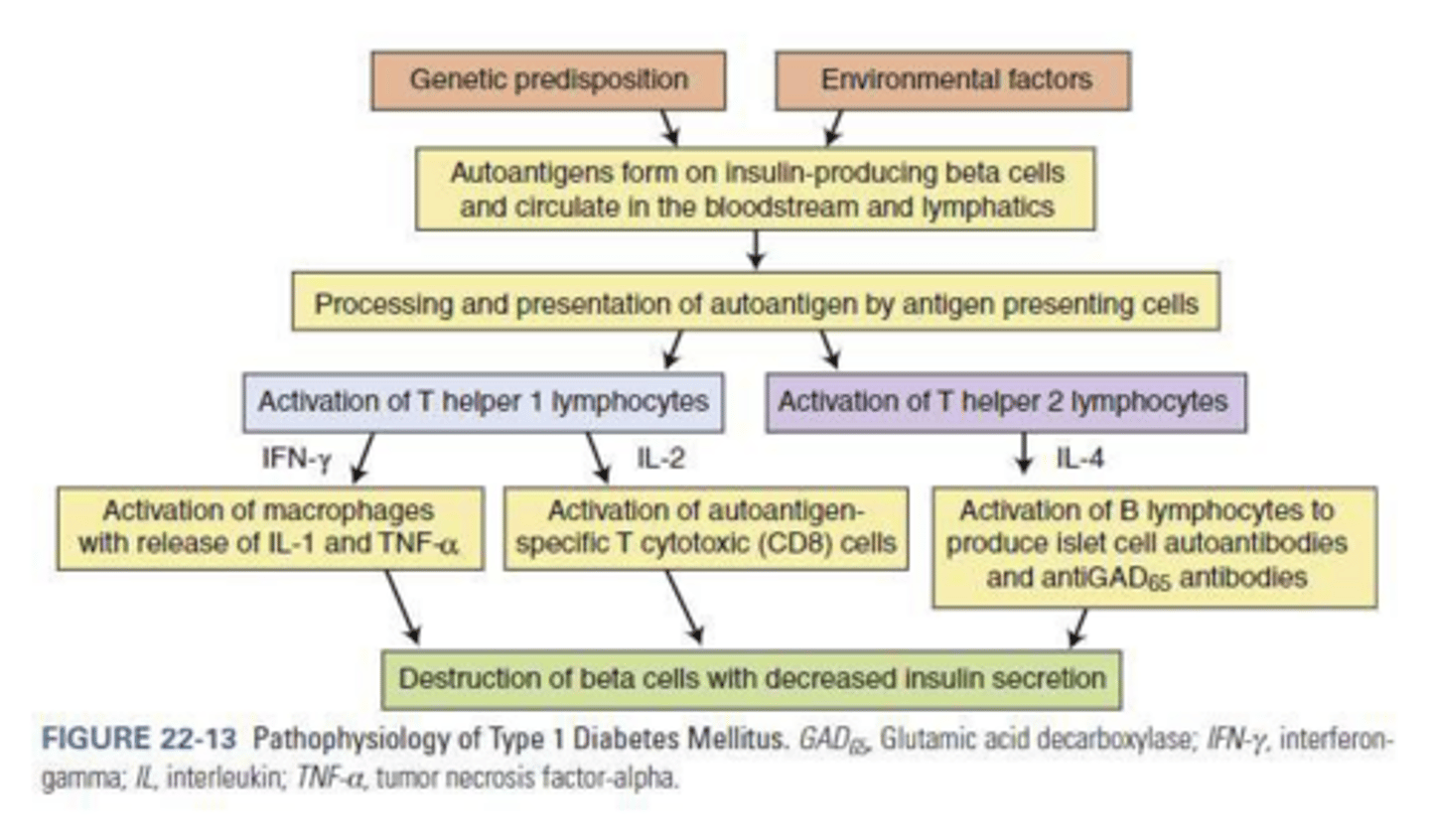
Type 1 Diabetes Mellitus (T1DM) Pathophysiology
Autoimmune destruction of pancreatic beta cells leading to absolute insulin deficiency typically due to genetic & environmental factors.
T1DM Peak Incidence
Between 9 months and 14 years of age.
Hyperglycaemia Classic Triad
Polydipsia (thirst), polyuria (excessive urination), and weight loss.
Type 2 Diabetes Mellitus (T2DM) Pathophysiology
Insulin resistance combined with progressive loss of beta cell insulin secretion.
T2DM Prevalence
Accounts for approximately 85% of diabetes in adults.
T2DM Risk Factors (Age/Lifestyle)
Age > 55, overweight, hypertension, smoking, PCOS, GDM or GDM in utero, and sedentary lifestyle.
Pre-diabetes
Condition of elevated fasting glucose and insulin resistance; high risk for diabetes.
Gestational Diabetes (GDM)
Diabetes that presents during pregnancy; requires "DIESEL" pre-hospital treatment.
GDM Risk Factors
>30 years of age
have a family history of T2DM
overweight
ethnic background (chinese, middle eastern, etc..)
previous GDM
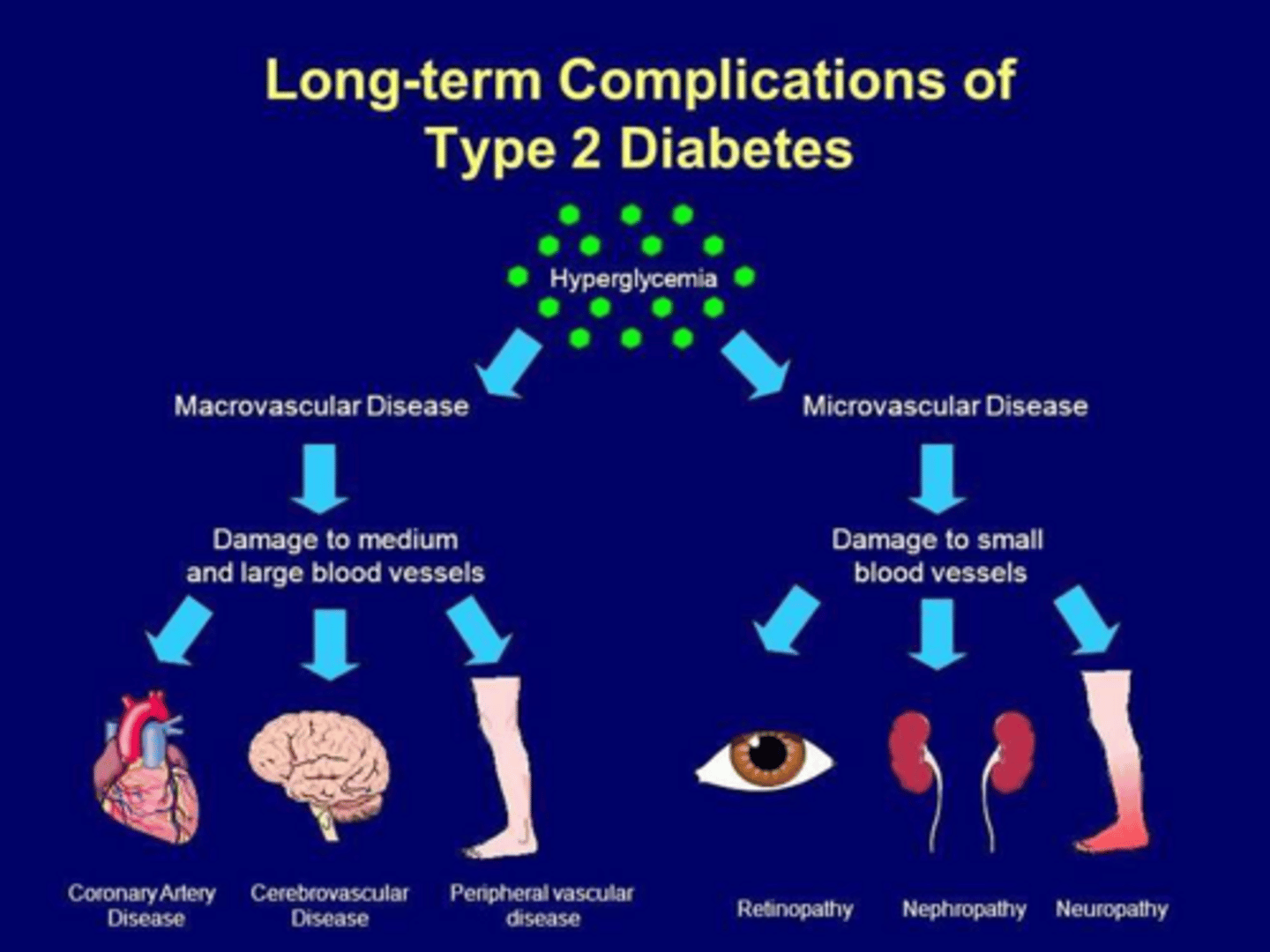
Long-Term Consequences of DM
macrovascular
microvascular
cardiovascular
Macrovascular Complications
Hyaline arteriolosclerosis (hardening) and atherosclerosis (stroke/AMI).
Microvascular Complications
Retinopathy (blindness), nephrotic syndrome (kidney damage), and peripheral neuropathy.
Cardiovascular Complications
Silent Ischemia/AMI, Atypical cardiac presentations
Silent Ischaemia in Diabetics
Increased incidence of unrecognized AMI (40% in diabetics vs 25% in non-diabetics).
Hypoglycaemia Definition
Blood Sugar Level (BSL) < 4.0 mmol/L.
Euglycaemia Range
Fasting BSL between 4 to 6 mmol/L.
Brain Susceptibility in Hypoglycaemia
Neuronal glycogen stores deplete in 2 minutes, risking brain damage.
Causes of Hypoglycaemia
Excess insulin, missed meals, alcohol ingestion, unplanned exercise, or infection.
Hypoglycaemia: Adrenaline Release Effects
Increased HR, diaphoresis, increased respiratory rate, and cold skin.
Neurogenic (Autonomic) Symptoms
Hunger, tremor, anxiety, palpitations, tachycardia, sweating, and pallor.
Neuroglycopenic (CNS) Symptoms
Headache, irritability, confusion, ataxia, diplopia, hemiparesis, and seizures.
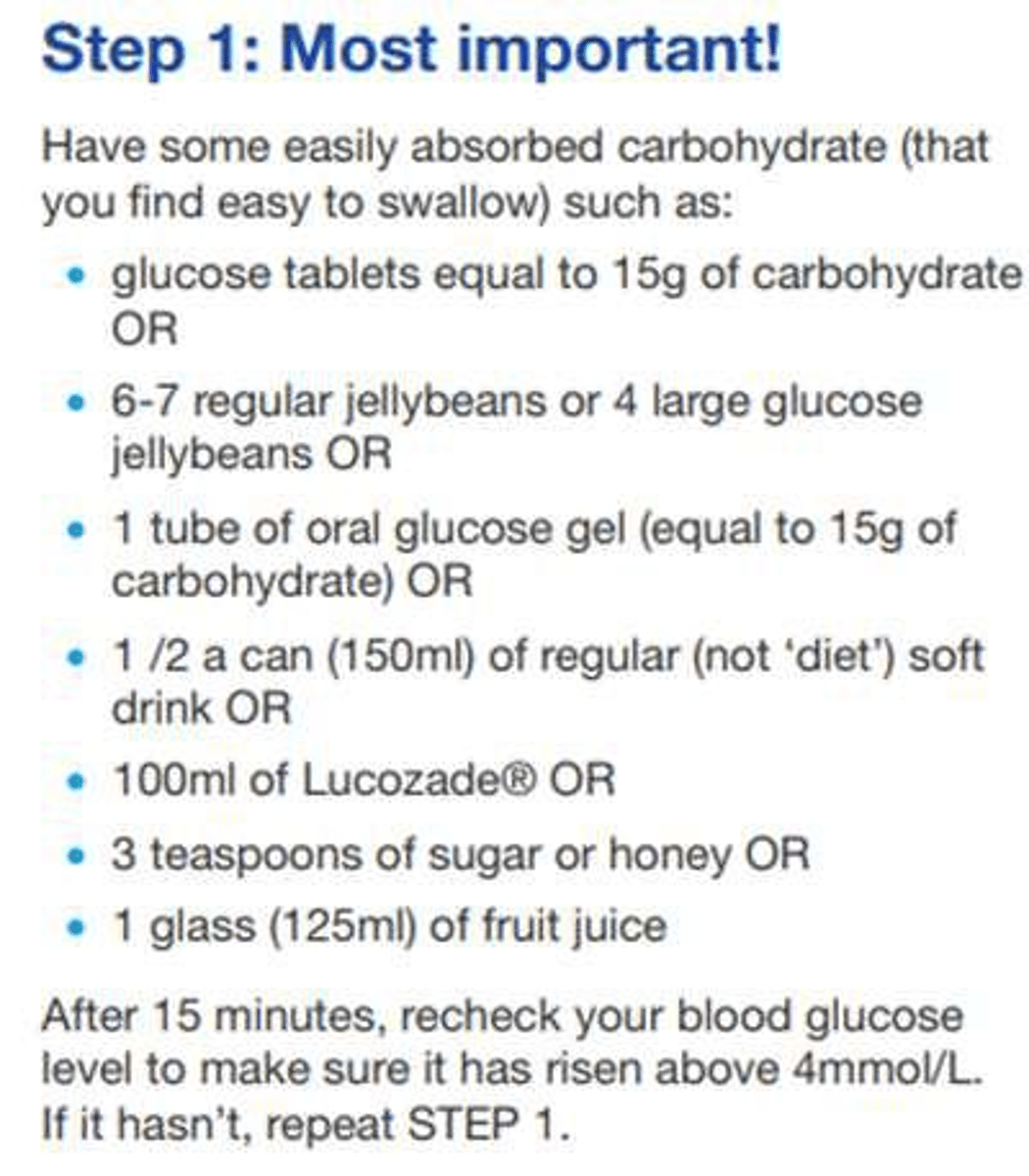
Pre-hospital Management: Glucose Gel
15g dose; requires the patient to be able to obey commands.
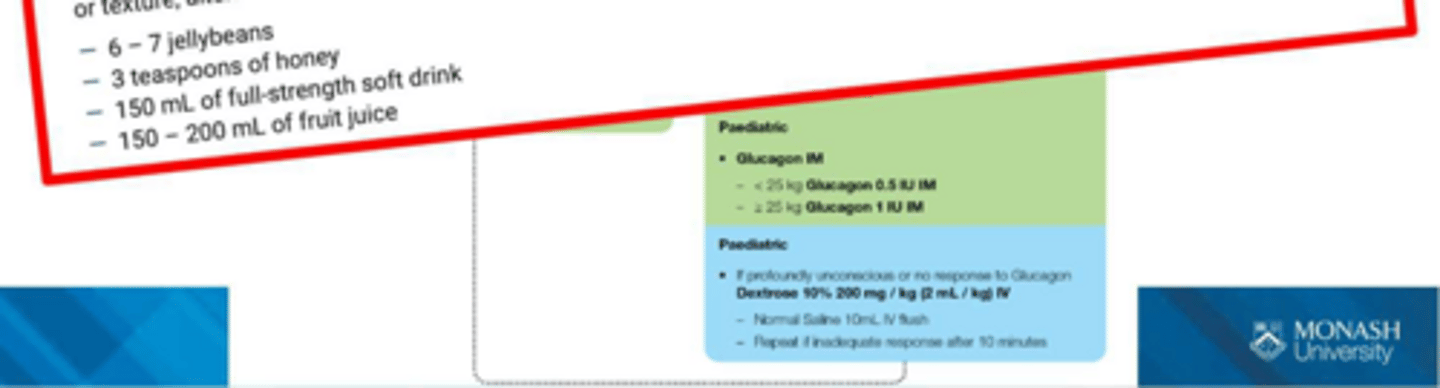
Pre-hospital Management: Glucagon IMI
Intramuscular injection; less effective if patient has poor glycogen stores.
Pre-hospital Management: IV Dextrose
5-10% concentration; can cause tissue necrosis if extravasation occurs.
Hyperglycaemia Definition (BGL)
Blood glucose levels > 10 mmol/L.
Normal Ketone Level
<0.6mmol
Elevated Ketone Level
Ketone level > 3 mmol/L.
Precipitating Factors for Hyperglycaemic Emergencies
Infection, discontinuation of insulin, or inadequate insulin therapy.
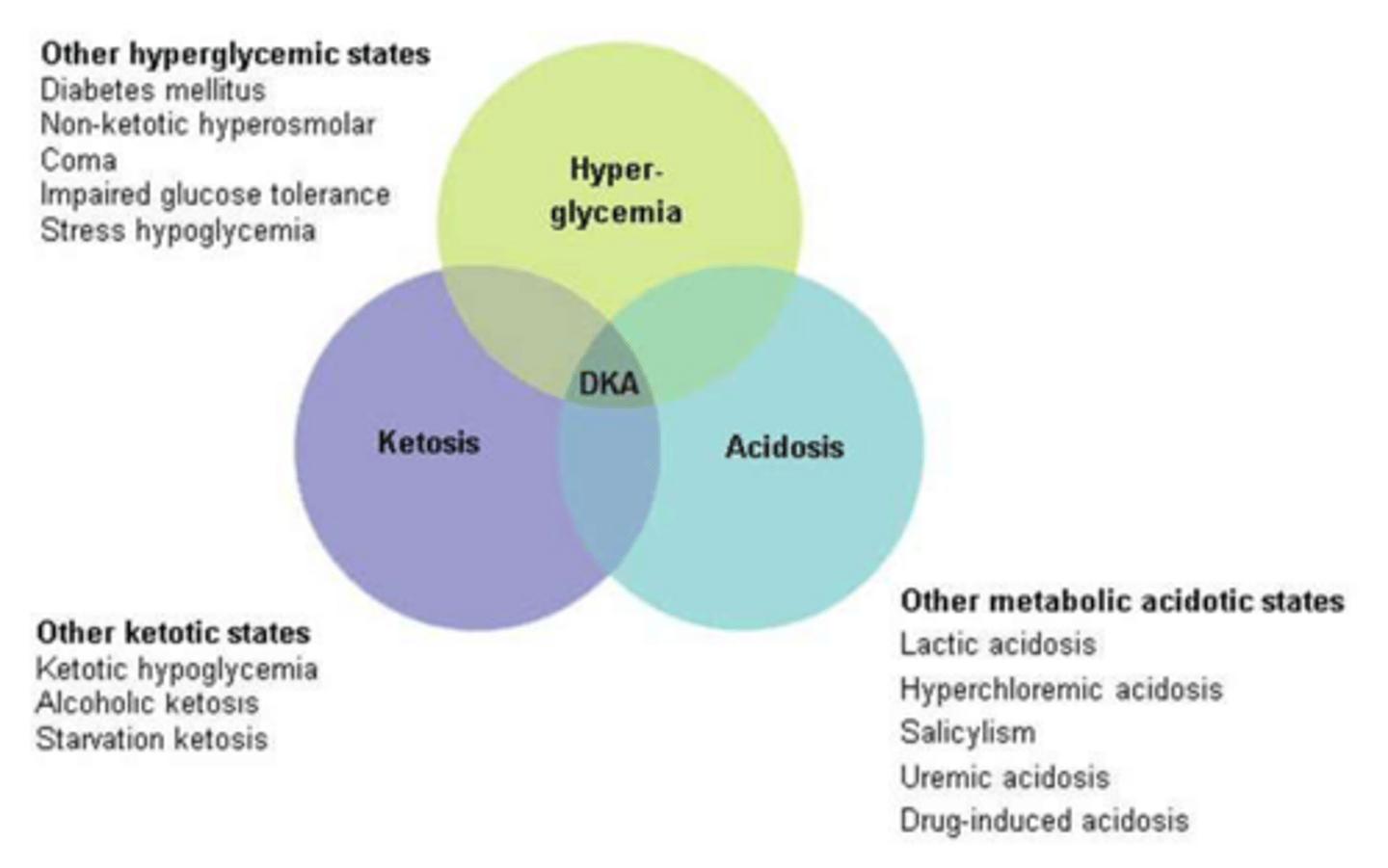
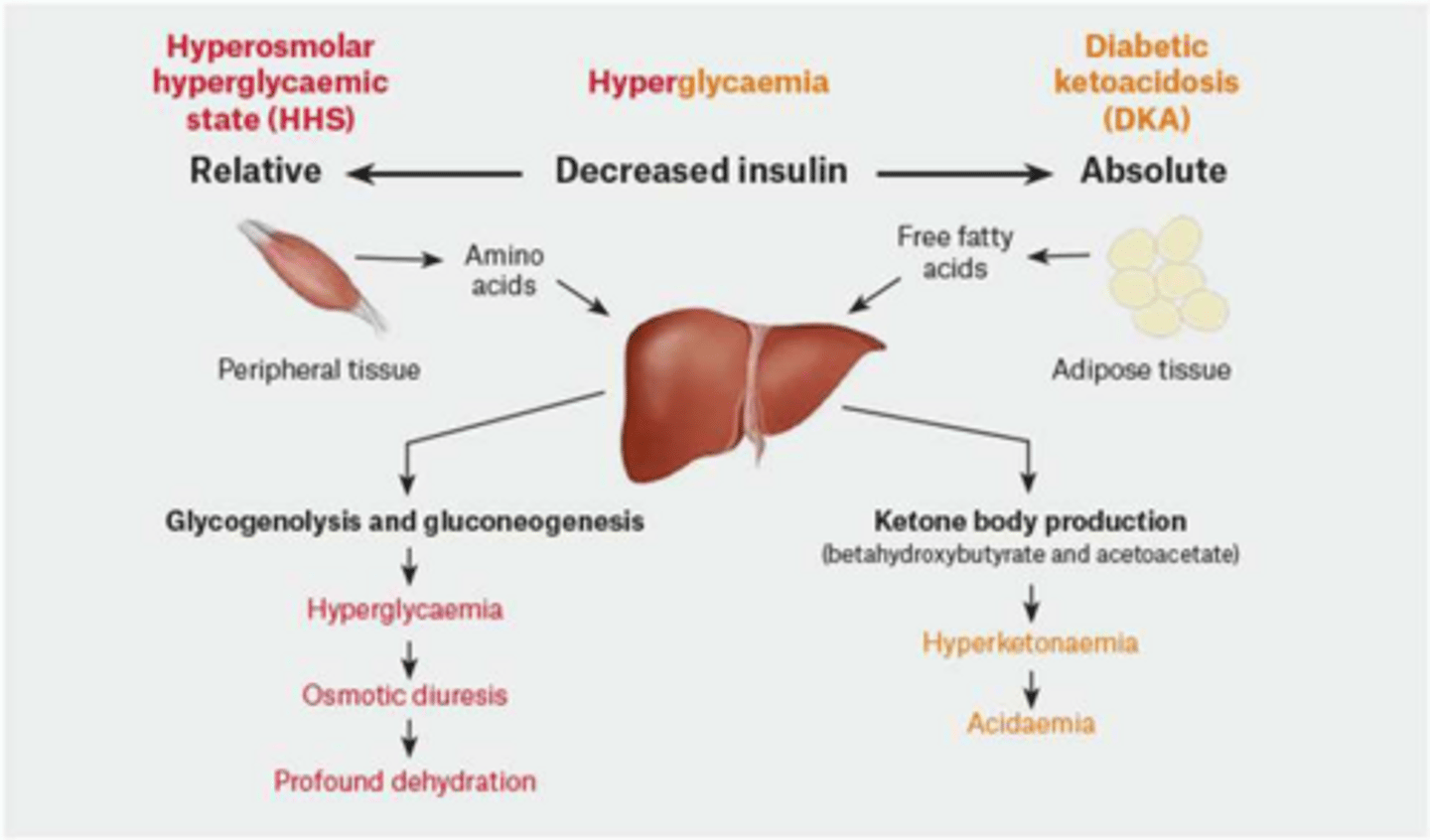
DKA Pathophysiology: 3 States
Hyperglycaemia, ketosis, and metabolic acidosis.
DKA Pathophysiology
uncontrolled catabolism associated with carbohydrate insufficiency
insulin deficiency is a necessary precondition
DKA Fluid Loss
Averages approximately 6-9 L.
DKA Presentation: Evolution Time
Usually evolves rapidly, over a 24-hour period.
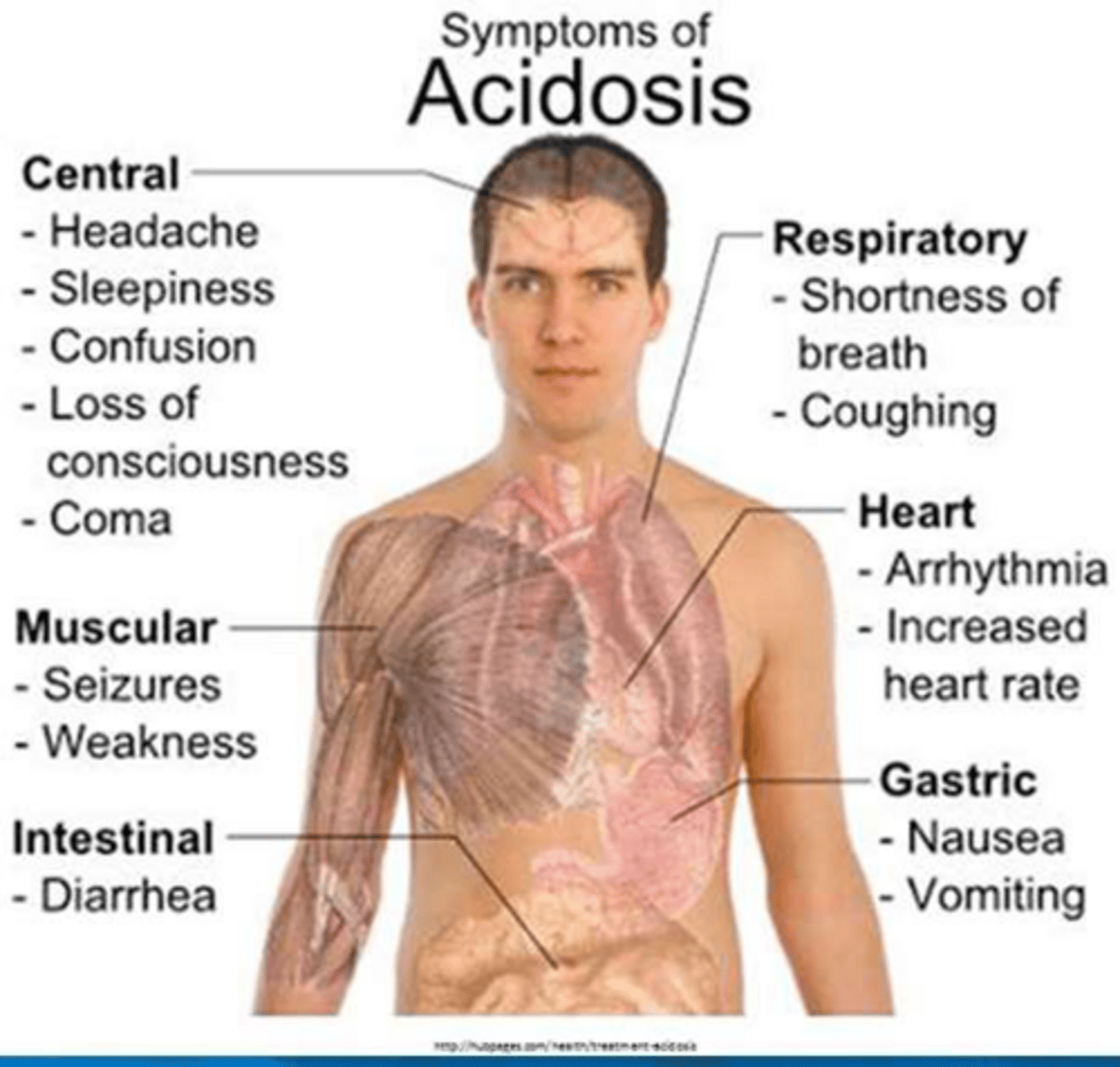
DKA Signs: Dehydration/Shock
Tachycardia, hypotension, arrhythmias, and altered consciousness.
Kussmaul Respiration
Deep, labored breathing pattern associated with severe metabolic acidosis.
HHS?
Hyperosmolar Hyperglycaemic State
HHS vs. DKA: Ketones
HHS has enough insulin to prevent ketone production; DKA does not.
HHS Risk Factors
Elderly, reduced fluid intake, infection, MI, or stroke.
HHS Presentation: Neurologic Symptoms
ALOC, seizures, hemiparesis, aphasia, muscle twitching, or hallucinations.
HHS Presentation: Evolution Time
Develops insidiously over several days.
HHS Pathophys
insulin deficiency enough that hyperglycemia develops, but not enough to produce fatty acids/ketones
severe hyperosmolarity and dehydration
Assessment of Hyperglycaemic Emergencies
Check BSL and ketones; assess dehydration and RSA.
Management: IV Fluid Goal
Replace total volume loss within 24-36 hours.
Euglycaemic Ketoacidosis
Normal BSL with elevated ketones (>3 mmol/L).
Euglycaemic Ketoacidosis Risk Factors
SGLT inhibitors, fasting (surgery), or illness/infection.
How can dehydration be assessed?
dry mouth
tented skin on forearm
hypotensive
acs