Pharm II Week 10 (Stimulants, Antipsychotics, Mood Stabilizers)
1/116
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
117 Terms
ADHD - Epidemiology and Scope
One of the most common neurodevelopmental disorders found in children and adolescents
National survey data from 2016 indicate 8.4% (5.4 million) of children 2 to 17 years of age currently had ADHD, representing 5.4 million children.
Boys are more than twice as likely as girls to receive a diagnosis of ADHD
ADHD - A Clinical Diagnosis (DSM5)
A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development
•Onset of sx presents < 12 y/o
• Sx present at 2+ settings
• The disturbance causes significant impairment in social, occupational, and academic functioning.
• The disorder is not accounted for by any other behavior disorder
< 17 years old = ≥ 6 symptoms for 6 months
≥ 17 years = ≥ 5 symptoms for 6 months

DSM V Types of ADHD
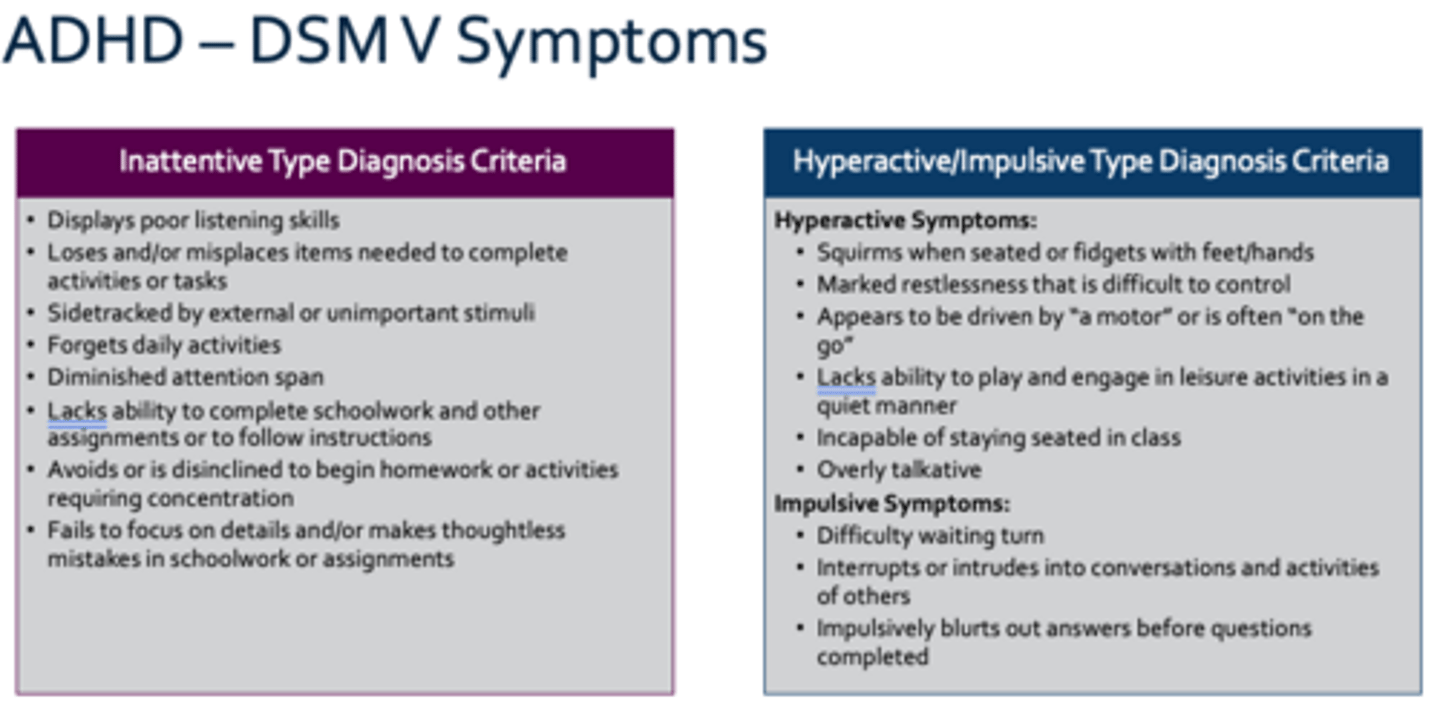
• Predominantly inattentive
• Predominantly impulsive or hyperactive
• Combination of the above
Inattentive Type vs Hyperactive/Impulsive Type Diagnosis Criteria
ADHD - Symptom Manifestation by Age
Preschool: Hyperactive-impulsive behavior
School Age: Hyperactive-impulsive behavior, Academic problems, Poor social interaction
Adolescents: Academic problems, Poor social interaction, Low self-esteem, Oppositional behavior
College Age: Academic problems, Poor social interaction, Low self-esteem, Substance/sex abuse, Accident/injury
Adulthood: Occupational problems, Low self-esteem, Marital problem, Substance/sex abuse, Accident/injury
ADHD – Treatment Approach *KNOW*
4-5 years of age
Parent training in behavior management (PTBM) and/or behavioral classroom interventions
FDA approved medications (methylphenidate!!) can be considered when:
• Moderate-to-severe ADHD that did not respond to behavioral interventions
• In areas in which evidence-based behavioral treatments are not available.
ADHD – Treatment Approach *KNOW*
6-11 years of age
FDA-approved medications for ADHD with PTBM and/or behavioral classroom intervention (preferably both)
•First Choice: Stimulant (methylphenidate or amphetamine)
•Second Choice: Nonstimulant medications including norepinephrine reuptake inhibitors (atomoxetine) and selective α-2 adrenergic agonists (e.g., guanfacine or clonidine)
ADHD – Treatment Approach *KNOW*
12-18 years of age
FDA-approved medications, behavioral/training interventions, and educational interventions/supports
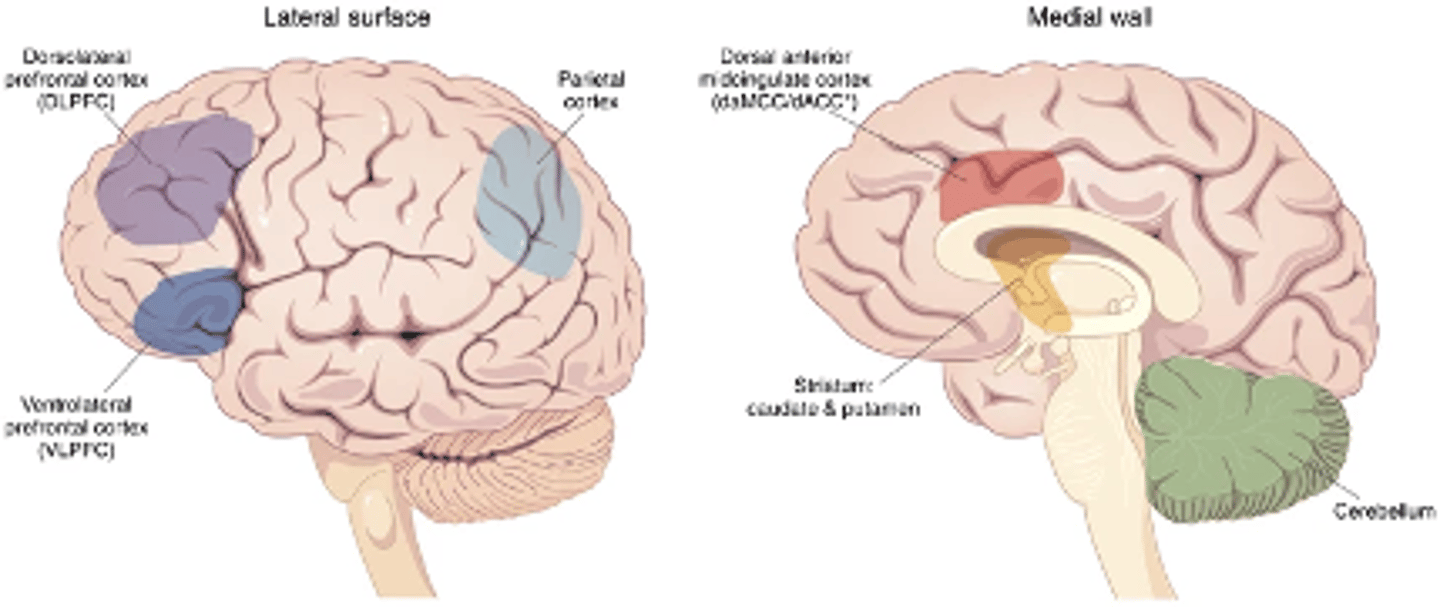
ADHD - Pathophysiology
not fully understood
•Cognitive/functional deficits that relate to diffuse abnormalities in the brain
•Deficits in anterior cingulate gyrus
•Motor control, attention, decision-making, and social cognition
•Deficits in dorsolateral prefrontal cortex (DLFPC)
•Planning, working memory, and executive functions
•Reduced activity in frontostriatal region
•Attention, cognitive control, and executive function
It is thought that these changes account for the deficits in goal-directed behavior
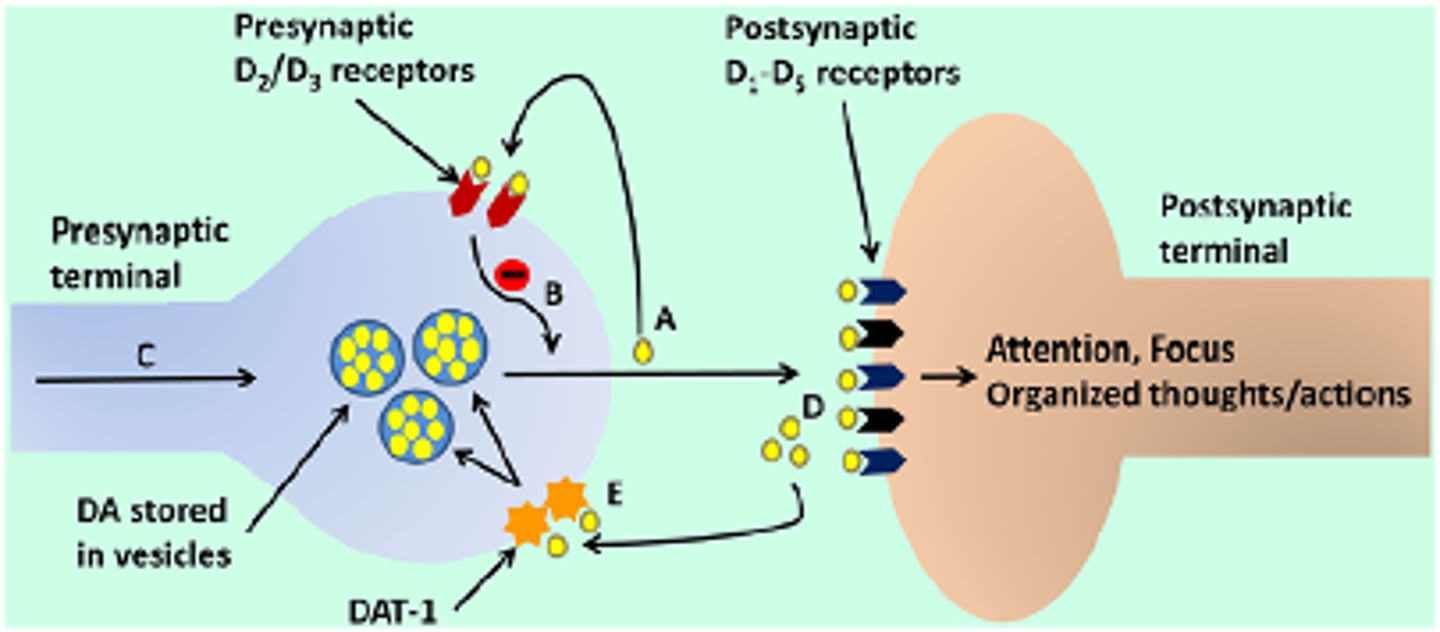
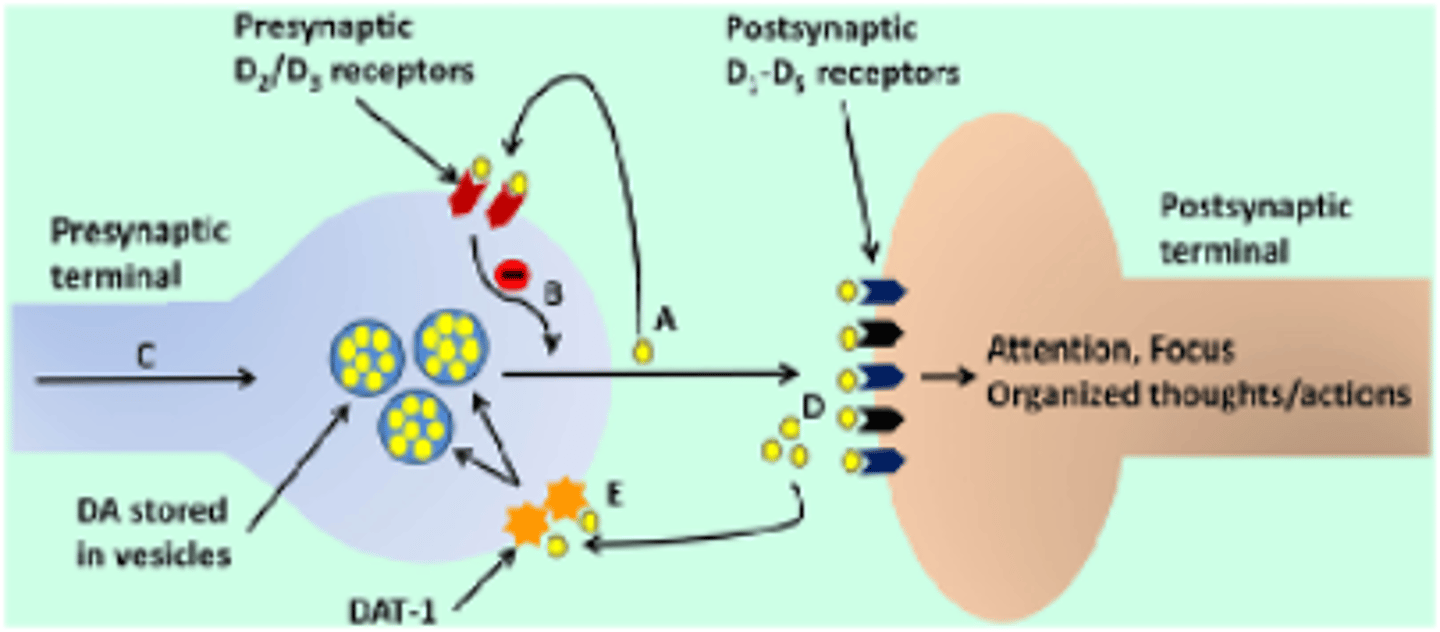
ADHD - Neuroreceptors
•Reduced levels or dysfunction of dopamine transporters and receptors
•Reduced levels of NE
•These NT are essential for motivation, focus, and impulse control
•When bored/fatigued, too little DA/NE is released --> insufficient activation of postsynaptic D1 and α-2 receptors --> individual becomes distracted & misguided attention
•When stressed, too many NT are released --> overstimulation of receptors --> misguided attention and responses
There are two classes of ADHD medication
Stimulants: Methylphenidate, amphetamines
Non-Stimulants: Atomoxetine
Titrate doses of ADHD medications to reach their maximum benefit with tolerable side effects
•Stimulants can be effectively titrated on a weekly basis
•Atomoxetine’s peak effect is approximately 4 to 6 weeks after initiation
•Guanfacine and clonidine demonstrate peak effects about 2 to 4 weeks after initiation
Stimulants
what are they? includes?
A broad class of drugs that increase the activity of the CNS
•Caffeine is the most commonly used stimulant in the world
•Also includes amphetamines, methylphenidate, ephedrine, cocaine, pseudoephedrine, modafinil
Amphetamine class of drugs is used for
medical (legal) and recreational (illegal) purposes
Prescription stimulants are considered ________ by the FDA
Prescription stimulants are considered Schedule II (drugs with a high potential for abuse, with use potentially leading to severe psychological or physical dependence)
Stimulants – Adverse Effects & Monitoring *KNOW*
Broad range of short-term and long-term adverse effects including
•Major influencers of ADRs include body weight, tolerance, and using with or without food
•Insomnia
•Loss of appetite, weight loss, anorexia
•irritability, emotional lability, anxiety
•increased BP, tachycardia
•dry mouth, NVD, abdominal pain, headache
Stimulants – Adverse Effects & Monitoring *KNOW*
Monitoring should be done frequently, especially when titrating doses, including?
•Check ht, wt, HR, BP at every visit
•Periodic EKGs
•Verify appropriate sleep
•Review with child's parents/teachers/caregivers for target sx relief
•Adjust dosing with changing weight and coverage needs that change with age
Methylphenidate MOA
blocks the reuptake of NE and dopamine into presynaptic neurons; appears to stimulate the cerebral cortex and subcortical structures
Methylphenidate ADRs
•Cardiovascular events, including increased BP, stroke, and heart attack; so avoid in patients with cardiac issues!!
•Growth suppression, including decreased weight and height
•Priapism
•New onset psychosis or mania (e.g., delusions), aggressive behaviors
The only stimulant FDA approved for 4 to 5 year old patients is??
Methylphenidate!
Methylphenidate - Short Acting Duration
•Onset of Effect: 20 to 30 minutes
•Duration of Effect: 3 to 6 hours
may need to admin at school
2 options for short-acting methylphenidates
Methylphenidate
•Ritalin
•Methylin Oral
Dexmethylphenidate
•Focalin
Methylphenidate - Intermediate Acting Duration & Delivery
•Onset of Effect: 60 to 180 minutes
•Duration of Effect: 3 to 8 hours (variable)
•Delivery System: the drug diffuses through a hydrophilic gel, leading to tablet disintegration and a steady release of methylphenidate
3 options for intermediate-acting methylphenidate
•Ritalin LA (capsule)
•Metadate (capsule)
•Methylin ER (tablet)
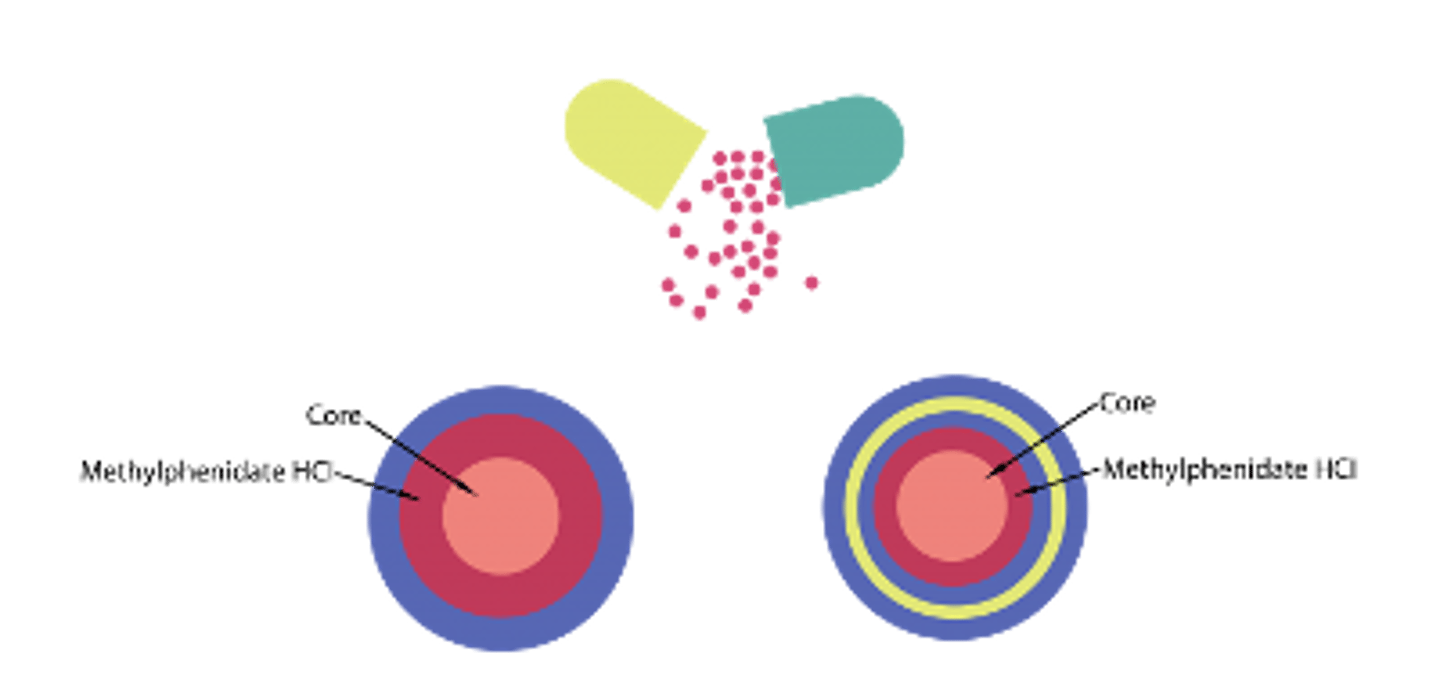
Methylphenidate - Long Acting Duration & Delivery
•Onset of Effect: 20 to 60 minutes
•Duration of Effect: 8 to 16 hours (variable)
•Delivery System: Different ratios of capsule particles
options for long-acting methylphenidates
Methylphenidate
•Ritalin LA
•Metadate CD
•Aptensio XR
•Quillivant XR
•Quillichew XR
•Cotempla XR ODT
Dexmethylphenidate
•Focalin XR
Methylphenidate - Transdermal KNOW
dosing/how to apply
Dose is NOT equivalent to oral MPH IR doses
•Pts begin with 10 mg patch due to increased bioavailability
•Patch should be placed on pt's hip 2 hrs before efficacy needed
•Rotate sites daily
•Remove after 9 hours max
• Absorption noted to continue for up to 3 hours post removal (‘skin depot formation’)
•Absorption also increases when heat is applied
Methylphenidate Transdermal Option
Daytrana (transdermal patch)
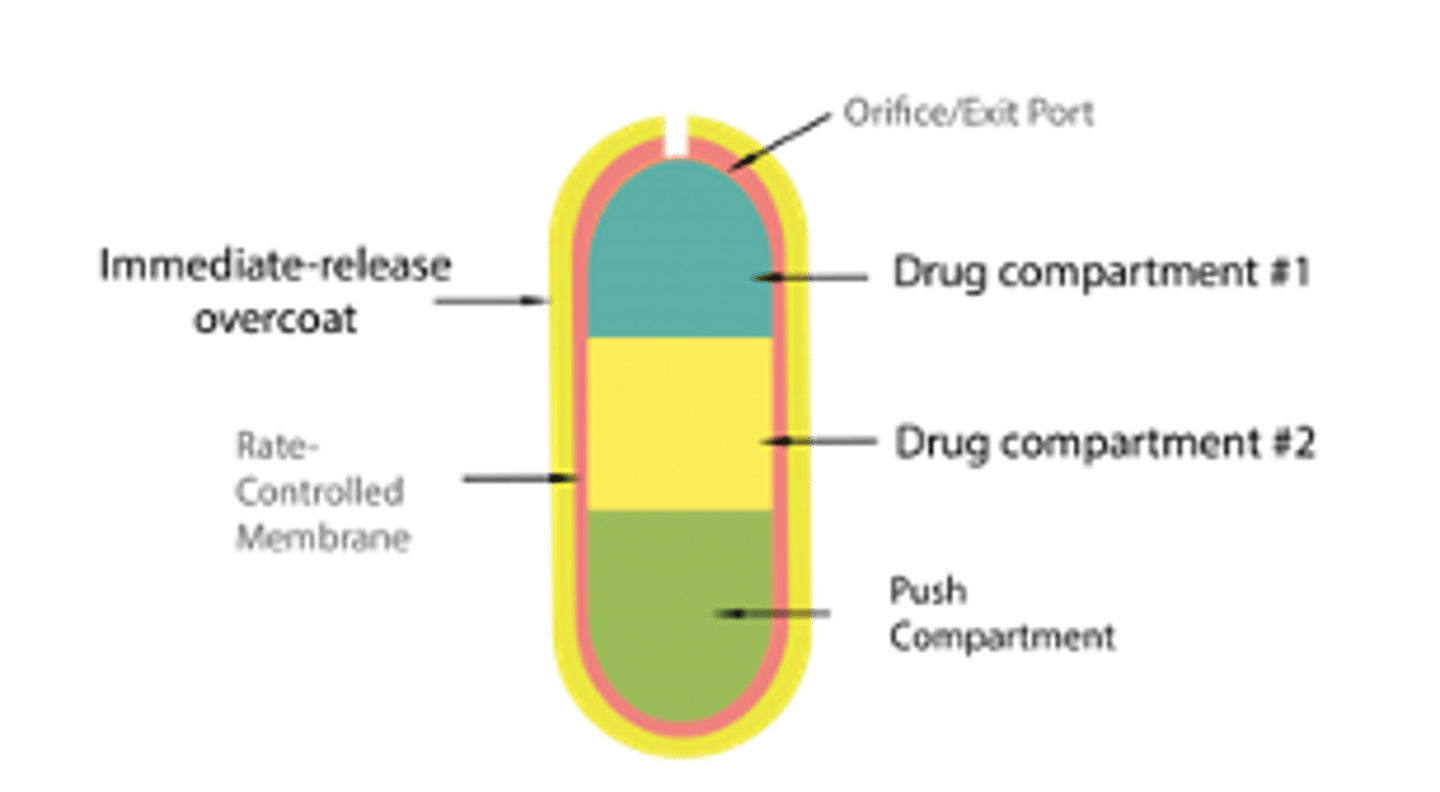
Methylphenidate - OROS
what is it and duration
•Osmotic controlled release oral delivery system (OROS)
•Tablet shell can be found in stool
•Duration of Effect: 12 hous
Methylphenidate - OROS
medication?
Concerta (tablet)
*Tablet shell can be found in stool
Amphetamines - MOA KNOW
Promote release of catecholamines (primarily dopamine and NE) from their storage sites in the presynaptic nerve terminals; minorly ability to block the reuptake of catecholamines
•Enhances release of NE in the periphery
•d-AMP is the more active isomer vs. l-AMP
Amphetamines - ADRs
•CV events, including increased BP, stroke, and heart attack; avoid in patients with cardiac issues
•Growth suppression, including decreased wt and ht
•New onset psychosis or mania (e.g., delusions), aggressive behaviors
•Serotonin syndrome when used with other agents that impact serotonin transmitters
serotonin sdr sx?
tachycardia, shivering, diarrhea, diaphoresis, muscle cramps, agitation, and increased body temperature; these symptoms are usually followed by hypertension, hyperthermia, hyperreflexia, delirium, tremors, and rigidity
if a patient is on an SSRI, what ADHD med to avoid?
Amphetamines
Amphetamines - Short Acting Duration
Duration of Effect: 4 to 6 hours
Amphetamines - Short Acting Medication Options
Dextroamphetamine
•Dexedrine
•Zenzedi
•Procentra
Mixed amphetamine salts
•Adderall (capsule)
Racemic amphetamine sulfate
•Evekeo (tablet)
•Dyanavel XR
Amphetamines - Intermediate Acting onset and duration
•Onset of Effect: 60 to 90 minutes
•Duration of Effect: 6 to 10 hours (variable)
Amphetamines - Intermediate Acting Medications
Dextroamphetamine
•Dexedrine Spansules
Amphetamines - Long Acting Prodrug
onset, duration
•Onset of Action: 30 minutes
•Prodrug: is metabolized into the active ingredient after being ingested
•Duration of Effect: 8 to 14 hours
Amphetamines - Long Acting Prodrug KNOW
medication?
Lisdexamfetamine -- Vyvanse!!
Modafanil MOA
•Not used in ADHD
•The exact MOA is unclear. Modafinil has been shown to significantly increase DA in the brain by blocking DA transporters; however, has a lower affinity for DA receptors compared to amphetamines.
Modafanil ADRs
•Cardiovascular events, including increased BP, stroke, and heart attack; avoid in patients with cardiac issues
•Hypersensitivity reactions
•Immediate: angioedema, anaphylaxis
•Delayed: Steven-Johnson syndrome, toxic epidermal necrolysis
•New onset psychosis or mania (e.g., delusions), suicidal ideation
modafanil indication
excessive daytime sleepiness associated with narcolepsy, obstructive sleep apnea, shift work sleep disorder
Which stimulant is a prodrug?
What are three monitoring parameters for ongoing stimulant use?
Which stimulant is a prodrug? Vyvanse
What are three monitoring parameters for ongoing stimulant use?
-Ht and wt
-Cardiac
-Sleep
Non-Stimulants include
Atomoxetine
Atomoxetine MOA
Selectively inhibits the reuptake of norepinephrine with little to no activity at the other neuronal reuptake pumps or receptor sites.
Atomoxetine BBW
Increase in suicidal ideation in children and adolescents
Atomoxetine ADRs
•CV events, including QTC prolongation, increased BP, stroke, and heart attack; avoid in patients with cardiac issues
•Growth suppression, including decreased weight and height
•New onset psychosis or mania (e.g., delusions), aggressive behaviors
•Priapism
Atomoxetine Onset and Duration
•Onset of Action: 2-4 weeks to see full effects
•Duration of Effect: 8-12 hours
Combat Methamphetamine Epidemic Act KNOW
Designed to limit the availability and distribution of precursor products for methamphetamine
•Ephedrine
•Pseudoephedrine
•Phenylpropanolamine (PPA)
Sale is limited to 3.6 g daily, 9 g per 30 day period. Mail order sales limited to 7.5 g per 30 day period.
•Regulated products must be sold “behind the counter”
•Required verification of identity prior to all sales i.e. driver’s license
Schizophrenia - Epidemiology and Scope
•Chronic brain disorder with a prevalence of around 0.3% to 0.7% globally
•Characterized by disruptions in thought processes, perceptions, emotional responsiveness, and social interactions
Typically diagnosed in the late teens years to early thirties
•Males: late adolescence – early twenties
•Females: early twenties – early thirties
Associated with significant health, social, and economic concerns
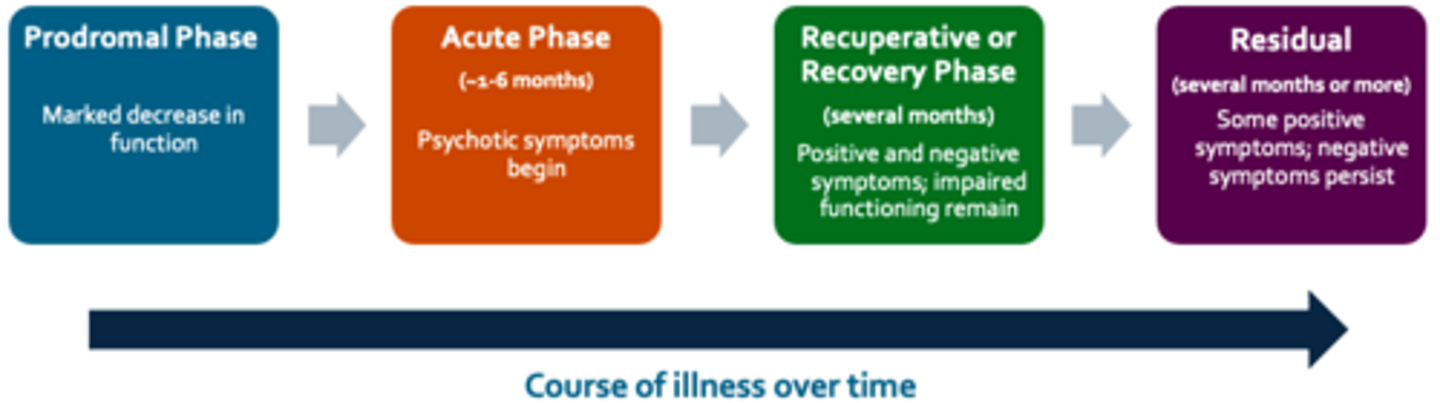
Schizophrenia - Symptom Manifestation
course of illness over time
Prodromal Phase: Marked decrease in function
Acute Phase (~1-6 months): Psychotic symptoms begin
Recuperative or Recovery Phase
(months): Positive and negative sx; impaired functioning remains
Residual (several months or more): Some positive sx; negative sx persist
Schizophrenia - DSM V Criteria
(A) 2+ of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated). At least one of these must be a characteristic symptom. (see image)
(B) For a significant portion of the time since the onset of the disturbance, level of functioning is markedly below the level achieved prior to the onset
(C) Continuous signs of the disturbance persist for at least 6 months, at least 1 month of sx (A)

Schizophrenia - Pathophysiology
•Not fully understood
•Associated with many NT
•Subcortical DA dysfunction = key factor in psychotic sx
Causes neuroanatomical changes over time
• various regions of the brain that have been implicated
• gray matter of the brain is consistently affected
Schizophrenia - Treatment Approach
Patient-centered treatment plan is essential
•Consider factors such as the severity of the illness, patient history of treatment response, the balance between medication efficacy and side effects, and patient preferences.
clozapine = patients that have tried and failed everything else, last ditch effort to help pt
Schizophrenia – Treatment Approach
SGAs vs FGAs
•No clear preference exists between SGAs and FGAs overall
•Individual medication efficacy varies
•Clozapine potentially more effective in treatment-resistant schizophrenia and for those patients with a high risk for aggression or suicide
Primary goal of antipsychotic treatment?
•Primary goal of antipsychotic treatment is to alleviate symptoms and restore the patient’s normal functioning
•Maintenance therapy is to prevent symptom recurrence, reduce hospitalizations, and improve quality of life
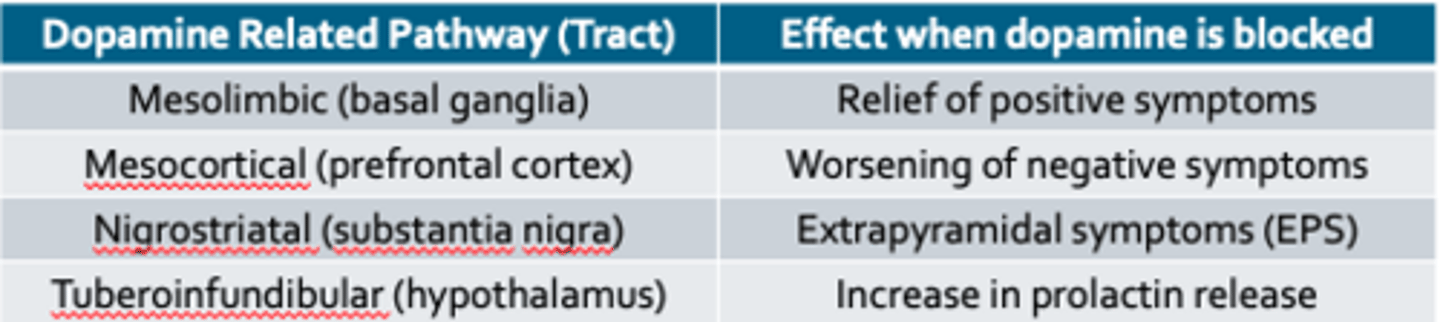
First Generation Antipsychotics (FGAs) MOA
•Dopamine (D2) receptor blockade; also have noradrenergic, cholinergic, and histaminergic blocking action
•Crucial in the mesolimbic pathway associated with positive symptoms of psychosis
•First-generation antipsychotics can be classified according to their ________
all compared to?
First-generation antipsychotics can be classified according to their potency
All are compared to chlorpromazine
All antipsychotics have BBW for ??
increased risk of death in elderly patients with dementia
schizophrenic patients that have tried and failed everything else, what med to give?
clozapine = patients that have tried and failed everything else, last ditch effort to help pt
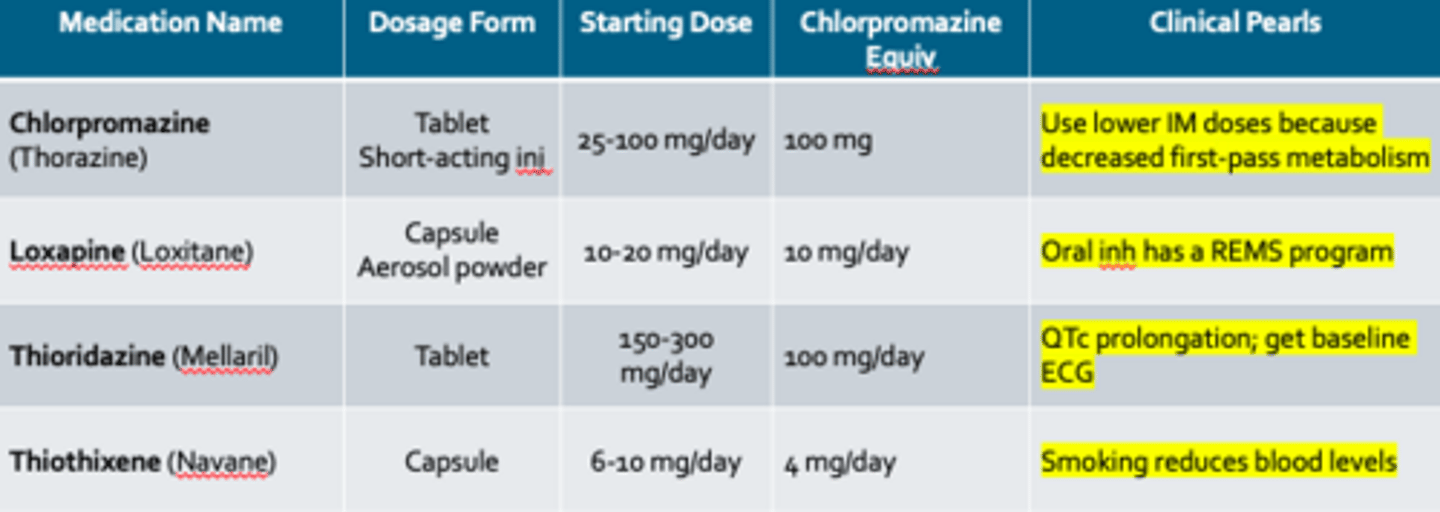
FGAs- Low-Med Potency agents
know first gen low/med/high potency antipsychotics + ADRs
only ones in the LO's:
Chlorpromazine (Thorazine)
Loxapine (Loxitane)
FGAs- Med-High Potency agents
know first gen low/med/high potency antipsychotics + ADRs
only one in the LO's:
Haloperidol (Haldol) - high potency
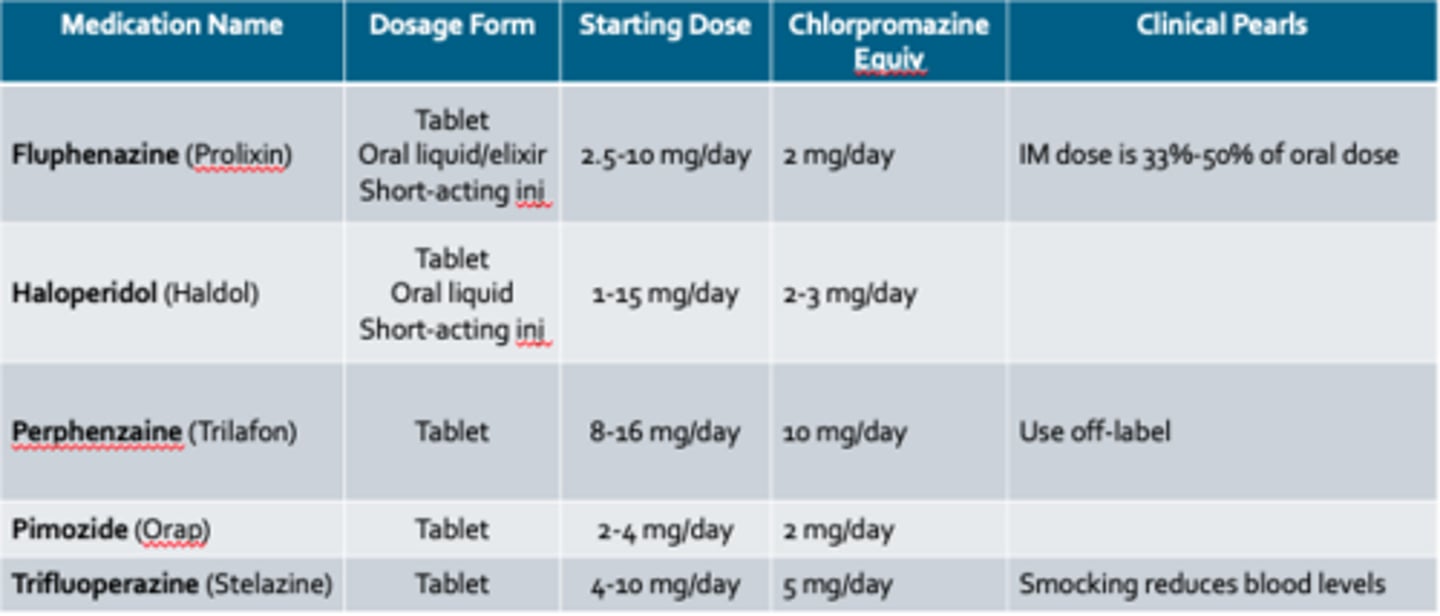
FGA - Side Effect Profiles *KNOW*
EVERYTHING compared to chlorpromazine (so know it well)
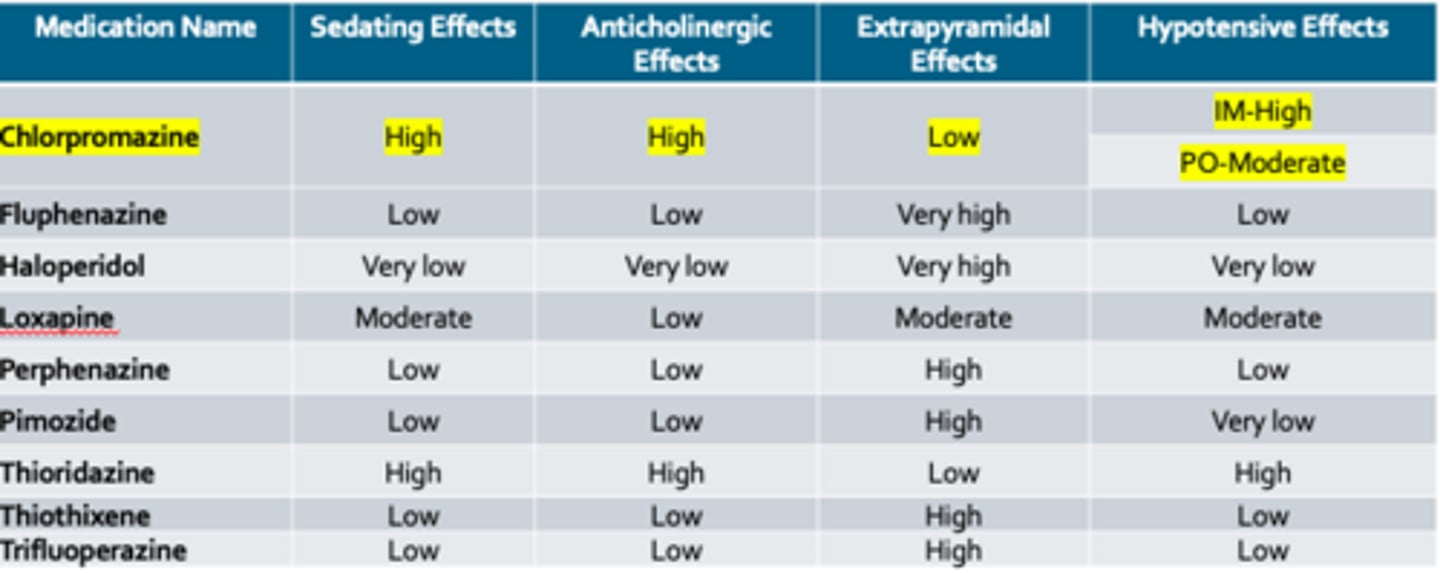
FGA- Extrapyramidal Side Effects
acute dystonia
akathisia
pseudoparkinsonia
tardive dyskinesia
Acute Dystonia
define and tx
Rigidity or stiffness in large muscles
Treatment:
•Centrally-acting anticholinergic
•Diphenhydramine
•Benztropine
Akathisia
define and tx
Restlessness with anxiety and inability to remain still
Treatment:
•Propranolol
•Benzodiazepines
Pseudoparkinsonism
define and tx
Shuffling gait, cog-wheel rigidity
Treatment:
•Centrally-acting anticholinergic
•Diphenhydramine
•Benztropine
•Amantadine
Tardive Dyskinesia
define and tx
Abnormal facial movements of tongue, or mouth
Treatment:
•Switch to a second generation antipsychotic or reduce the dose
•VMAT-2 Inhibitors - valbenazine, deutetrabenazine
FIRST GEN ANTIPSYCHOTICS = HIGHEST RISK FOR
EXTRAPYRAMIDAL EFFECTS
FGA- Neuroleptic Malignant Syndrome
Rare but fatal adverse effect that can occur at any time during treatment
The onset of symptoms is over 24 to 72 hours with:
•Increased temperature, severe muscular rigidity, confusion, agitation, elevation in white blood cell count, elevated creatinine phosphokinase concentrations, elevated liver enzymes, myoglobinuria, and acute renal failure
FGA- Neuroleptic Malignant Syndrome
Treatment
•The antipsychotic should be immediately discontinued
•Adequate hydration and cooling should be closely monitored, as well as vital signs and serum electrolytes
•Dantrolene is the drug of choice
Is haloperidol high potency or low potency?
What are common side effects of haloperidol?
high potency
acute dystonia
akathisia
pseudoparkinsonism
tardive dyskinesia

SGA MOA
•Blocking D2 dopamine receptors as well as serotonin receptor antagonist action
•5-HT2A subtype of serotonin receptor is most commonly involved
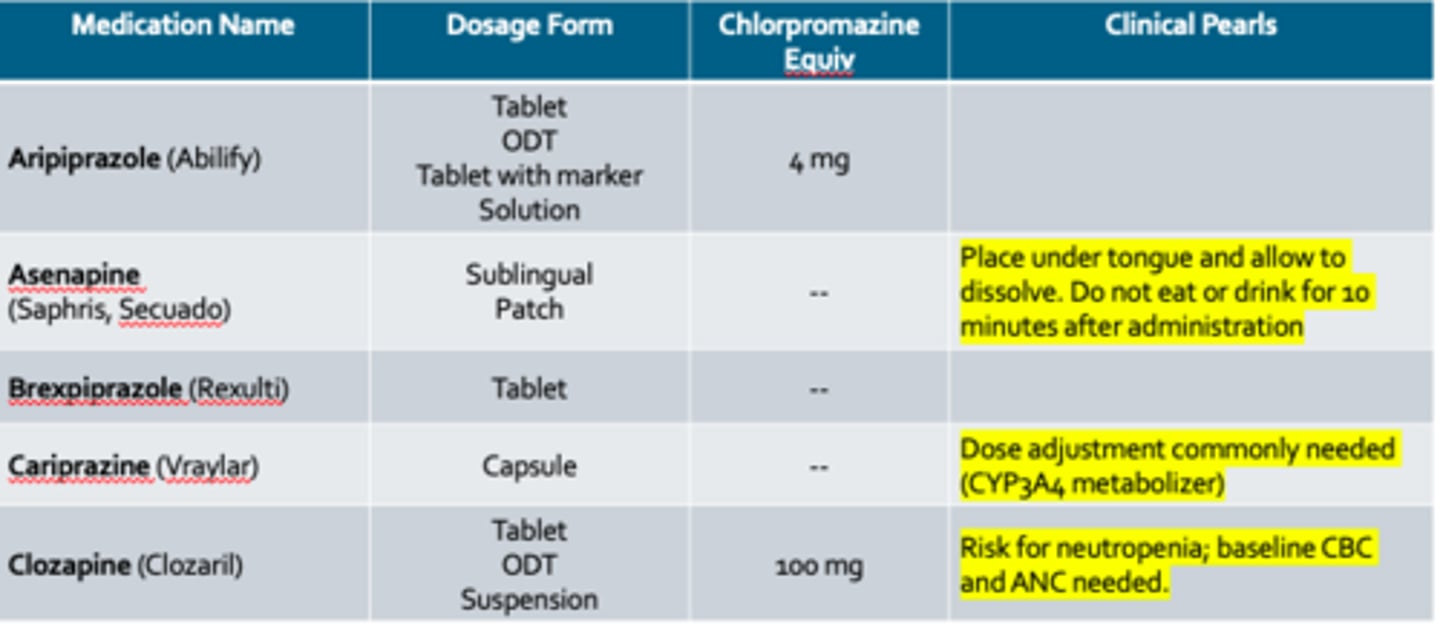
SGAs- Agents + clinical pearls
Aripiprazole (Abilify)
Clozapine (Clozaril)
**only 2 in the LOs
SGAs- Agents (cont.)
Olanzapine (Zyprexa)
Quetiapine (Seroquel)
only ones in the LO's
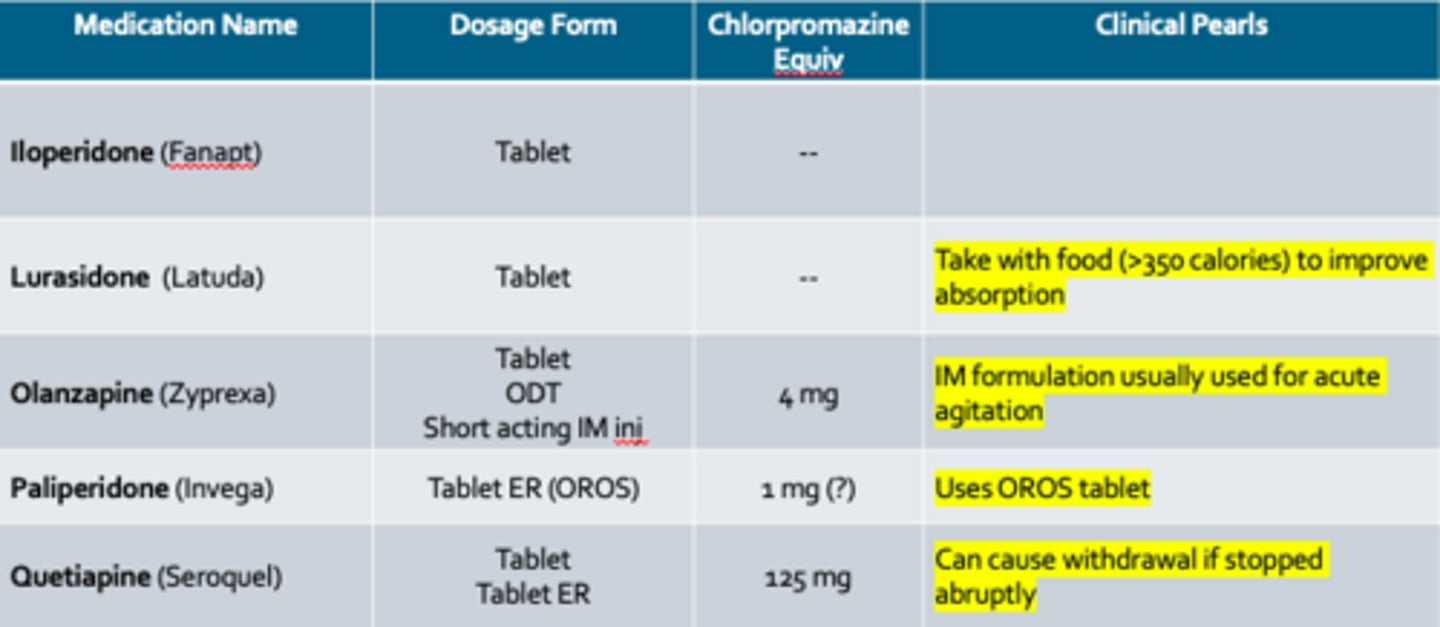
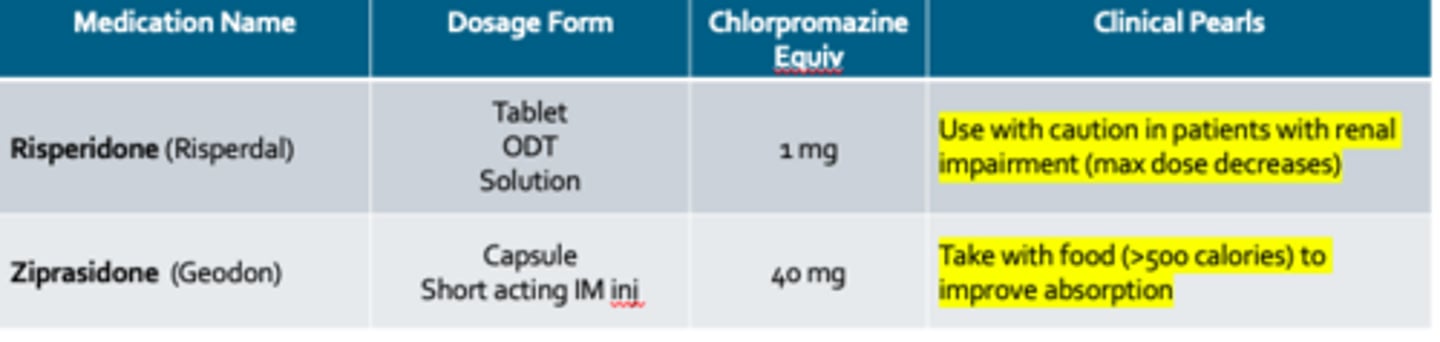
SGAs- Agents (cont. pt 3)
Risperidone (Risperdal)
Ziprasidone (Geodon)
SGA- Side Effects *KNOW*
•Have a much lower risk of extrapyramidal symptoms compared to FGAs
•QTc prolongation and other cardiac effects
•Hyperprolactinemia causing irregular periods, infertility, and lactation
QTc prolongation and other cardiac effects - highest and lowest risk drugs?
•Highest risk: Ziprasidone
•Lowest risk: Aripiprazole
Hyperprolactinemia causing irregular periods, infertility, and lactation - highest and lowest risk drugs?
•Highest Risk: Risperidone and Paliperidone
•Lowest Risk: Aripiprazole
SGA- also commonly associated with ??
More commonly associated with metabolic syndrome
•Increased weight gain/abdominal circumference
•Increased triglycerides/cholesterol
•Increased blood pressure
•Increased insulin resistance; assess family history of Type II DM!
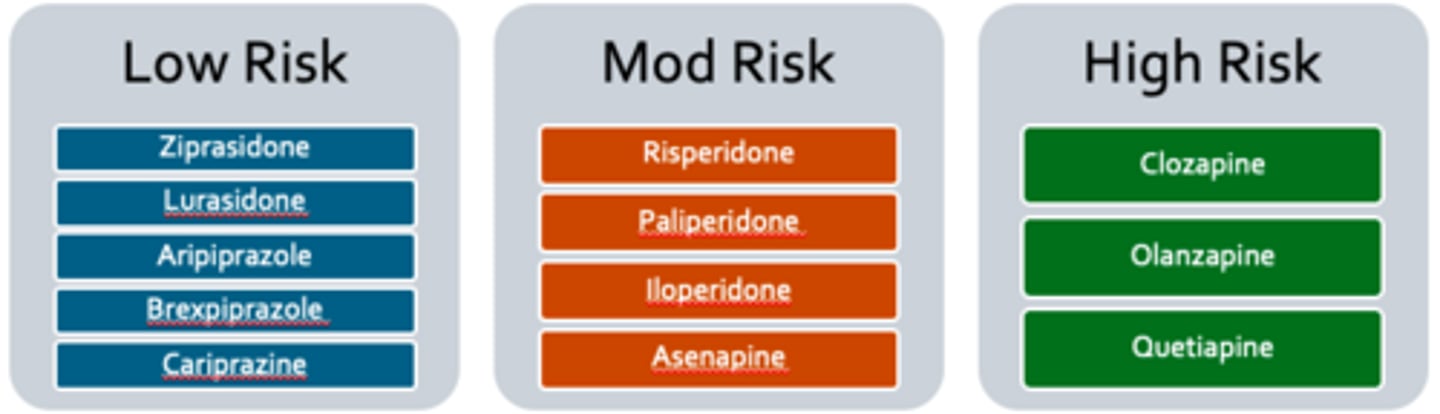
SGA- Metabolic Syndrome
high, mod, low risk??
Low Risk
•Ziprasidone
•Lurasidone
•Aripiprazole
•Brexpiprazole
•Cariprazine
Mod Risk
•Risperidone
•Paliperidone
•Iloperidone
•Asenapine
High Risk
•Clozapine
•Olanzapine
•Quetiapine
What second generation antipsychotics have a high risk of metabolic syndrome?
What second generation antipsychotic has the highest risk of QTc prolongation?
What second generation antipsychotics have a high risk of metabolic syndrome?
Clozapine
Olanzapine
Quetiapine
What second generation antipsychotic has the highest risk of QTc prolongation? Ziprasidone
Long Acting Injections - Rational
•Improve adherence in the outpatient setting
•Create less fluctuation in dosing
•Improve patient’s quality of life
•Decrease stigma
•Provide peace of mind to patient, family, and clinicians
First Generation Long Acting Injections (LAIs)
•Haloperidol Decanoate
•Fluphenazine Decanoate
Second Generation LAIs
Risperidone (Risperdal Consta)
Paliperidone (Invega)
•Sustenna
•Trinza
•Hafyera
Aripiprazole (Abilify Maintena)
Aripiprazole (Aristada)
Risperidone (Perseris)
Risperidone (Uzedy)
Bipolar Disorder - Overview
•Bipolar disorders comprise recurrent episodes of elevated mood and depression
•Affects more than 1% of the world's population. Has no predilection for race, sex, ethnicity, or socioeconomic status.
•¾ of patients with bipolar disorder have a history of three additional and concurrent mental health conditions
•Anxiety disorders, impulse control and attention-deficit/hyperactivity disorders, and substance use disorders are most common
•1/3 of patients will attempt suicide in their lifetime
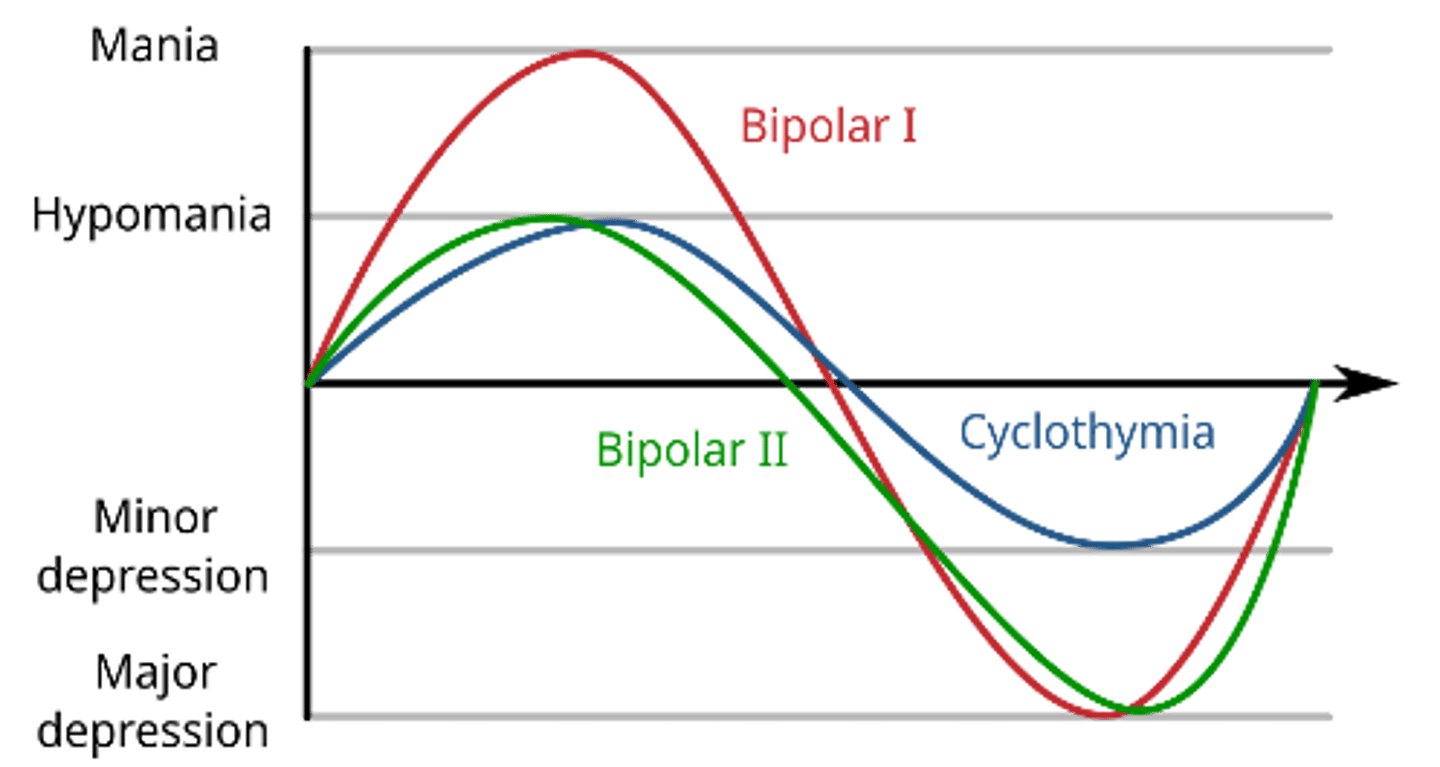
Bipolar Disorder - Bipolar I vs II
Bipolar I Disorder:
•At least 1 manic episode
•May be preceded or followed by hypomanic or depressive episode
Bipolar II Disorder:
•At least 1 hypomanic episode and at least 1 major depressive episode
•There has never been a manic episode
•Either depressive sx or the unpredictability of the fluctuations between hypomania and depressive episode cause significant distress or impairment
Bipolar Disorder - Symptoms
Mania
D Distractibility
I Indiscretion
G Grandiosity
F Flight of Ideas
A Activity Increase
S Sleep Deficit
T Talkative
Depression
S Sleep disturbances
I Interest decreased (anhedonia)
G Guilt and/or feelings of worthlessness
E Energy decreased
C Concentration problems
A Appetite/weight changes
P Psychomotor agitation or retardation
S Suicidal ideation
Bipolar Disorder - Treatment Approach
mainstay of tx?
Medications are the mainstay of therapy
•Selected depending on the presenting phase of illness, severity, and patient factors such as prior responses or current medications
Among patients using pharmacotherapy:
•Relapse occurs in up to 25% in the first year (40% if untreated)
•Relapse occurs in 70% of patients within five years, regardless of treatment approach
It is recommended that pharmacotherapy be continued indefinitely
first line for BPD
•Lithium
•Valproic acid/valproate/divalproex sodium
Second line for BPD
•Carbamazepine
•Lamotrigine
•Oxcarbazepine
BPD additional options
•Second generation antipsychotics (SGAs)
•Selective serotonin reupdate inhibitors (SSRIs)
Mood Stabilizers include
Lithium, Valproic Acid, Carbamazepine, Oxcarbazepine, Lamotrigine
Mood Stabilizers – Lithium MOA
Largely unknown for bipolar disorder despite a myriad of intra- and extra-cellular functions
•Onset of Action: 6 to 10 days
•Half-life: 20-27 hours, longer in the elderly
•Excreted via the renal pathway as unchanged drug
Lithium ADRs
•CNS depression
•Hypothyroidism (higher risk in women)
•Renal dysfunction and polyuria
•Weight gain
•Leukocytosis
Mood Stabilizers - Lithium Monitoring
Toxicity of lithium is dose dependent; overdose can be fatal
Monitor levels every 1-2 weeks, then every 3-6 months; also monitor renal function & thyroid
Therapeutic levels
Acute mania: 0.8-1.2 mEq/L
Maintenance 0.6-1.0 mEq/L
Lithium Toxicity
•mild toxicity – N/V/D, lethargy, drowsiness, tremor
•mod toxicity – severe N/V/D, confusion, ataxia, slurred speech, EKG changes
•severe toxicity – seizures, impaired consciousness, syncope, coma, renal insufficiency – can be fatal
what drugs increase lithium levels?
•NSAIDS
•ACE inhibitors
•Thiazide diuretics
what drugs decrease lithium levels?
•Caffeine
•Acetazolamide
•Theophylline