motor behavior quiz 2 ch 4-6
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
biomechanical approach to manage hypertonicity focuses on?
altering muscle length thru prolonged stretching → manually OR cast, orthoses, splits
altering pt position → improves muscle length
hierarchy of sensory function
low → high
detection → discrimination → quantification → cortical sensation
detection → single pt stimulus
discrimination → btw 2 stimuli
quantification → organize tactile stimuli according to degree (roughness/wt)
cortical sensation → graphesthesia, stereognosis (recognize car in hand)
UE flexion synergy presentation
scapular retraction & elevation
shoulder abd & ER
elbow flex
forearm sup
finger & wrist flex
LE extensor synergy
hip ext, add & IR
knee ext
ankle PF & inversion
toe PF
explicit learning is impaired w/ pt w/ lesion where?
medial temporal lobe damage (implicit retained)
lesion in prefrontal cortex impairs explicit or implicit learning?
both
what contributes to early recovery?
reduction of edema & resolution of diaschisis (loss of function in structurally intact brain area due to loss of input from anatomically connected injured area)
short vs long term habituation vs long term sensitization
short term → decrease in EPSP amplitude
long term → decrease in # of connections (structural change)
habituation exercises → inner ear disorder, dizziness w/ head mvmts
long term sensitization → increase in # of connections

BG pathology - hyper vs hypokinetic disorders
hypo → Parkinson
hyper → athletoid CP, huntington's, hemiballismus
hyperkinetic disorders characterized by
excess, involuntary mvmt & hypotonicity
chorea vs athetosis
both result of BG disorder
chorea → involuntary, rapid, irregular, jerky mvms (side effect of antiparkinsonian meds as well)
athetosis → slow, involuntary, writhing & twisting mvmts; UE > LE; may also involve neck, face, tongue
dystonia initiated/worsened w/?
characterized by?
primarily result of?
voluntary action
associated w/ overflow muscle activation, unintentional muscle contraction
characterized by agonist/antagonist muscle contraction
primarily disorder of BG disorder, but also could be thalamus, brainstem & cerebellum lesion
APTA model of practice
exam → history, review of systems, test & measures, data collection to form diagnosis, prognosis, POC
evaluation → clinical reasoning based on data from exam
prognosis, diagnosis → intervention
plan of care
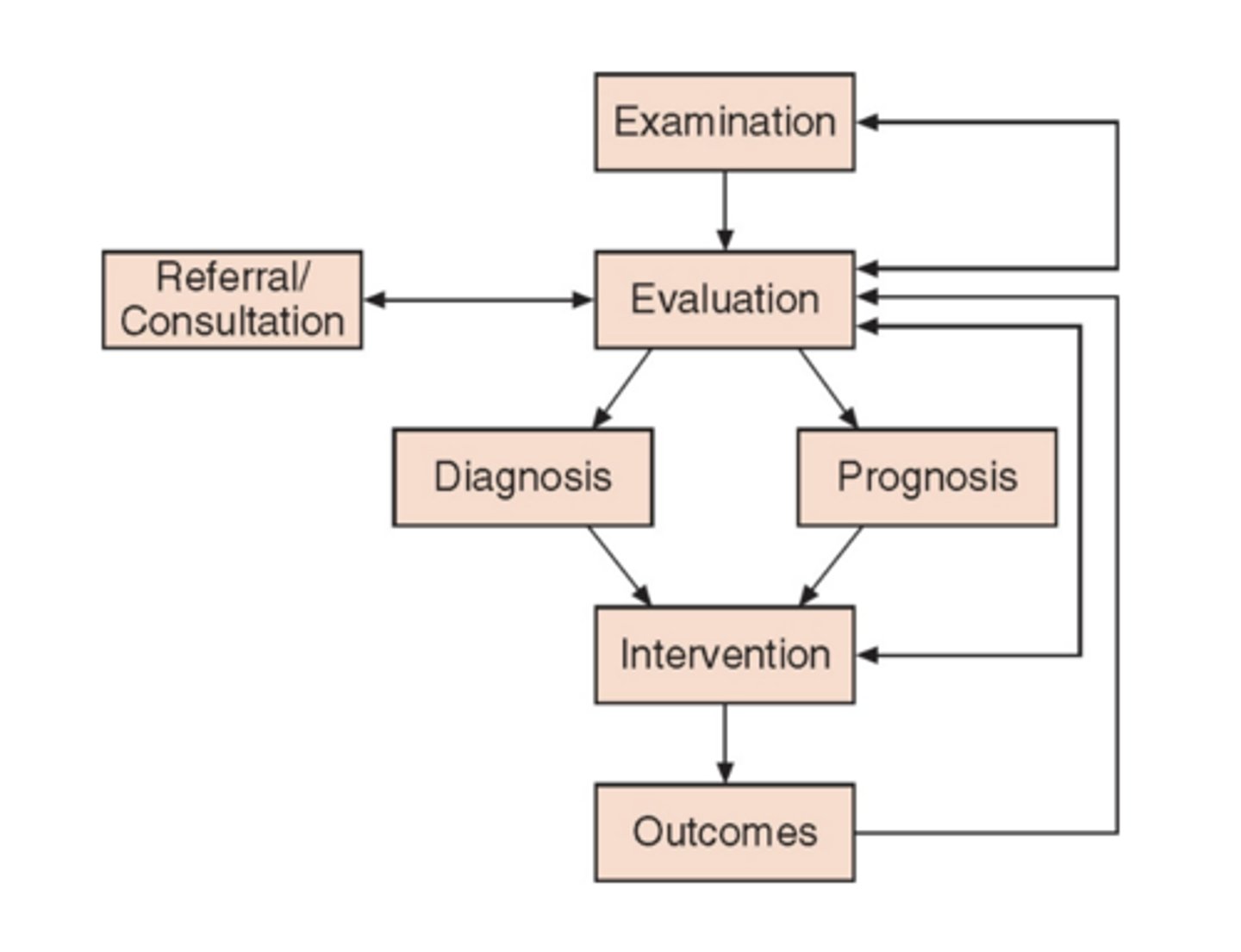
table 5.2 pg 134 non equilibrium test of coordination
10 principles of neuroplasticity article
use it or lose it
use it & improve it
specificity → skill acquisition enhances corticospinal excitability (specific rather than generalized)
repetition matters → acquisition of skill & continued performance over time
intensity matters → higher better as long as pt stable, sensitivity to overuse (potential neg side effect of training intensity after brain damage - overuse impaired extremities that worsens function)
time matters → gene expression → synaptic formation → motor map reorganization; find optimal window; time delays - self taught compensatory behavior
salience matters → what is important to pt, more motivated & increased attention, involves Ach → administration of Ach agonist - enhance recovery after brain damage;
age matters → younger brain recover better, older - can, takes longer; healthy old animals benefit from complex motor skills training, exercise, exposure to complex & social environments
transference → 1 facilitates another, direct electrical stimulation of motor cortex enhances recovery
interference → teaching 1 behavior can interfere w/ another