EKG/cardio review
1/154
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
155 Terms
angina/CAD/MI
s/s:
•Exertional chest pain
•Tight, squeezing, pressure
•Radiation (left arm? jaw?)
•Dyspnea, diaphoresis, N/V, indigestion, syncope
•PE may be Normal
•Tachycardia
•HTN
stable angina
CP lasts <30 minutes
unstable angina
CP lasts > 30 minutes or unrelieved with nitro/rest
•Troponins x 3
•CK-MB
•Risk factor screening:
•HEART Score
•Lipids
•DM status
•smoking
•family history
labs to order for suspected angina/CAD/MI
•Stable angina: normal vs. downsloping ST segment depression, reverses when ischemia disappears
•T-wave flattening or inversion
•ST-segment elevation: Check which leads are involved
•Q-wave
what findings may be seen on ECG in CAD/angina/MI
ECG
•Stress test
•Coronary angiography
•Monitors for arrythmias
•Echocardiogram
other studies to get for angina/CAD/MI
•MONA
•Heparin
•Beta-blockers
•ACE inhibitors
•Statins
•PCI/CABG
management for angina/CAD/MI
Calcium channel blockers
Tx for coronary vasospasm
•HTN
•Atherosclerosis
•Aneurysm
•Structural defects
RF for aortic dissection
type A aortic dissection
•involves arch proximal to left subclavian artery
type B aortic dissection
Involves proximal descending thoracic aorta just beyond left subclavian artery
aortic dissection
s/s:
•Sudden onset
•"Tearing" chest pain
•Radiation (to back)
•Hyper/hypotension
•Syncope
•Decreased peripheral pulses
•Aortic regurgitation murmur
•ECG: left ventricular hypertrophy
•CT scan
•Chest radiograph
•MRI
•Transesophageal echocardiogram
Dx for aortic dissection
•Reduce systolic blood pressure and pulse pressure
•Surgical intervention
Tx for aortic dissection
pericarditis
s/s:
•Chest pain – pleuritic, postural (better leaning forward, worse when taking a deep breath)
•Dyspnea
•Fever
Pericardial friction rub
•CBC
•Viral titers
•Cardiac enzymes- may be elevated
•ECG- diffuse ST elevation
•Sed rate
•ANA, RF, DS-DNA
•BUN/Creatinine
•Echocardiogram
Diagnostics to get for pericarditis
•NSAIDS/Colchicine
•Dialysis if uremic pericarditis
Tx for pericarditis
ASA
Tx for dressler syndrome
•Congenital
•Degenerative or calcific (atherosclerosis)
etiologies of aortic stenosis
aortic stenosis
s/s
•Systolic ejection murmur best heard at right upper sternal border
•Angina
•Heart failure
•Syncope
•Echocardiogram
•Cardiac catheterization
•ECG (LVH)
Dx for aortic stenosis
•Risk factor modification (ACEi, BB, diet, exercise, etc)
•Monitoring
Valve replacement
management for aortic stenosis
heart failure
s/s:
•Dyspnea
•Orthopnea
•PND
•Fatigue
•Cough
•Low cardiac output
•Pulmonary hypertension
•Increased venous pressure
•Decreased appetite
•Dependent peripheral edema
•Hepatomegaly
•Ascites
NYHA class I
Asymptomatic
NYHA class II
Mild limitation of physical activity; symptoms with ordinary activity
NYHA class III
Marked limitation of physical activity; symptoms with less than ordinary activity
NYHA class IV
Unable to perform any physical activity; Symptomatic at rest
HF stage A
No objective evidence of CV disease
HF stage B
Minimal CV disease
HF stage C
Moderate CV disease
HF stage D
Severe CV disease
•BNP
•Chest radiograph
•Echocardiogram
•ECG
•Cardiac Catheterization
Dx for heart failure
•Diuretic
•ACE inhibitor/ARB
•Neprilysin inhibitor/ARNI
•Beta-blocker – carvedilol (Coreg)
•ICD/Bi-ventricular pacing
•Daily weights
Dietary modifications
management for HF
dilated cardiomyopathy
causes: Idiopathic, alcohol, postpartum, other
s/s: LV or Bi-V Heart Failure Cardiomegaly, S3, elevated JVP, rales
echo: LV dilation and dysfunction
hypertrophic cardiomyopathy
Cause: Hereditary
s/s: Dyspnea, chest pain, syncope, Sustained PMI, S4, variable systolic murmur
Echo: LVH, asymmetric septal hypertrophy, small LV size, normal or supranormal EF
restrictive cardiomyopathy
Causes: Amyloidosis, post-radiation, post-open heart, diabetes
s/s: Dyspnea, fatigue, RV HF > LV HF, Elevated JVP, Kussmaul sign
Echo: Small or normal LV size, normal or mildly reduced EF
•Vasovagal
•Arrhythmia
•Cardiomyopathy
•Valvular heart disease
•Orthostatic
causes of syncope
vasovagal, situational, carotid sinus, atypical forms
causes of reflex-mediated syncope
primary/secondary autonomic failure, volume depletion, drug-induced
causes of orthostatic hypotension
arrhythmia- brady, tachy, drug induced, structural cardiac causes
causes of cardiac syncope
alpha 1 receptors
contraction of vascular and GU smooth muscle
beta-1 receptors
positive inotropic and chronotropic effects on the heart
hypertension urgency/emergency
180 or above/120 or above
stage 2 HTN
140 or above/90 or above
stage 1 HTN
130-139/80-89
elevated BP
120-129/<80
normal BP
<120/<80
•Headache
•Visual changes
•Chest pain
•Palpitations
•Dyspnea
•Claudication
•Sexual dysfunction
•Mental status change, n/v
•CV risk factors
symptoms to ask about in history for HTN
•thiazides, ACE/ARB, CCB
Tx for stage I HTN, non-black
•CCB, thiazides
Tx for stage I HTN, black
•2 or more drugs: ACE/ARB + Thiazide or BB
Tx for stage II HTN
•Orals/IV: Nifedipine, captopril, clonidine
•Reduce over hours
Tx for hypertensive urgency
•IV: Labetalol, nitroprusside
•Reduce BP by 25% in 1-2 hours
Tx for hypertensive emergency
arrhythmia
s/s:
•None!
•Palpitations
•Lightheaded/dizzy
•Pre-syncope/syncope
•Fatigue
•Dyspnea
•Altered level of consciousness
•Chest pain
•Tachycardia or bradycardia
•Irregular rhythm
•Hypotension
•ECG
•Holter monitor
•Event recorder- External loop recorder,, Internal loop recorder, Post-Event, MCOT
•Echocardiogram
•Stress test
Cardiac catheterization
general workup for arrhythmia
P wave
•Atrial depolarization
•<2mm high, <0.12sec wide
•Upright in leads I, II, V4-6, and AVF
•Inverted in AVR
•Variable in III, AVL and V1-3
ectopic atrial rhythm
Abnormal P wave inversion or morphology
Right Atrial hypertrophy
increased P wave height in V1
Left atrial hypertrophy
increased P wave width in V1
PR interval
•AV conduction time
•Measure from start of P to start of QRS
•Normal width: 0.12 – 0.20 sec
•Varies with heart rate
•Segment is isoelectric
•Long: possibly normal, 1st degree AV block, hyperthyroidism
•Short: Possibly normal, low atrial rhythm, WPW, HTN, Pheochromocytoma
QRS complex
•Ventricular depolarization
•Measured from beginning of QRS to end of S wave
•Width (duration): 0.05-0.10 sec
•Height: 5-30mm
Q wave
normal <0.04 sec and < 1/3 of the amplitude of the following R wave
ST segment
•Initial phase of ventricular repolarization
•Measured from end of QRS to beginning of the T wave
•Usually isoelectric
T wave
•Rapid phase of ventricular repolarization
•Normally upright in leads I, II, V3 and 5-6
•Normally inverted in lead AVR
•Variable in leads III, AVL, V 1-2
inversion can indicate ischemia
hyperkalemia
Peaked T waves, or height > 5mm in limb leads or 10mm in precordial leads indicates
QT interval
•Total duration of ventricular systole
•Measured from onset of QRS to end of the T wave
•Varies with heart rate and gender
•Long: Prolonged ventricular repolarization time (idiopathic, hypokalemia, meds , CAD, CHF, CVA)- Predisposes to arrhythmia
•Short: Digoxin, hypercalcemia, hyperkalemia
QTc
•Corrected Qt interval for heart rate
In general <0.45 seconds (roughly ½ the R-R)
R-R interval
•Measured from one R wave to the next
•Used to calculate rate
60-100 bpm
SA node rate
< 60 bpm
sinus bradycardia
>100 bpm
sinus tachycardia
automaticity focus
a potential pacemaker
atrial focus
60-80bpm
AV (junctional) focus
40-60bpm
ventricular focus
20-40bpm
paroxysmal tachycardia
•150-250bpm
flutter
•250-350bpm
fibrillation
350-400bpm
•one or more active automaticity sites
irregular rhythms are usually caused by:
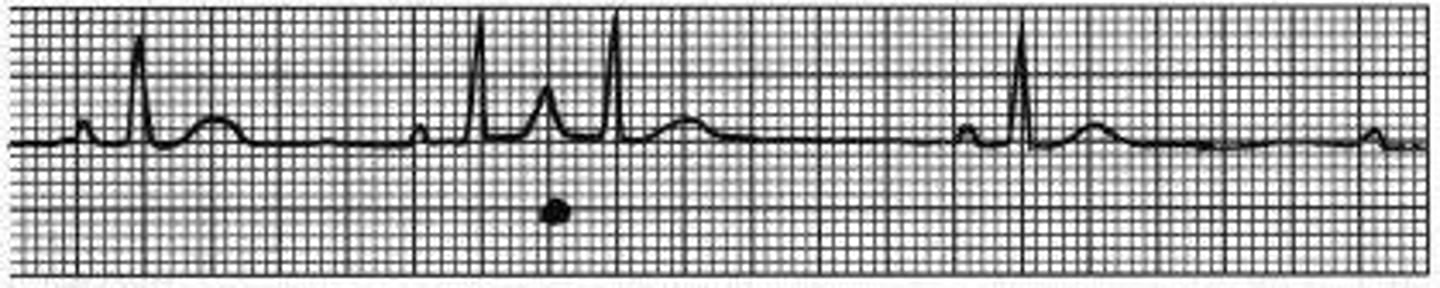
premature atrial contraction
•Premature stimulus that orriginates from an irritable atrial focus
•Atrial beat earlier than expected
premature atrial contraction
wandering atrial pacemaker
Irregular rhythms produced by nearby atrial automaticity sites
Rate is still <100bpm
Different p wave morphologies
wandering atrial pacemaker
multifocal atrial pacemaker
oRate is >100bpm
oAt least three different p wave morphologies
oCommonly seen in COPD
multifocal atrial pacemaker

atrial tachycardia
•Sudden, rapid firing of one irritable atrial focus
oFlutter
oFibrillation
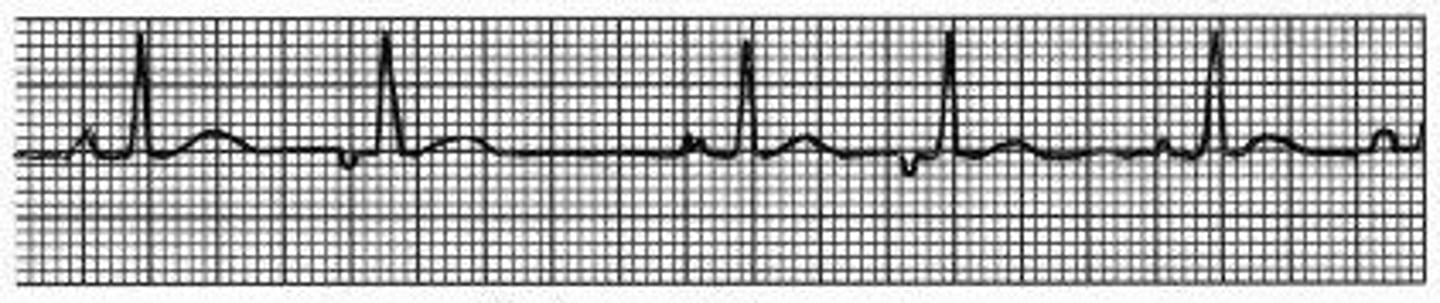
atrial flutter
•Rapid succession of identical, back-to-back atrial depolarization waves “flutter waves”
•Typically every 3rd or 4th wave depolarizes to ventricles
•“Saw tooth” pattern
atrial flutter

atrial fibrillation
•Many irritable atrial foci firing at same time
•Irregularly, irregular rhythm, no identifiable P waves
•Only small portion of atrium depolarized
atrial fibrillation

premature junctional contraction
•Premature stimulus that originates from an irritable junctional focus
•QRS slightly wider
•P wave inverted or short
premature junctional contraction

junctional tachycardia
oSudden rapid firing of irritable junctional focus
oP waves absent or possibly inverted
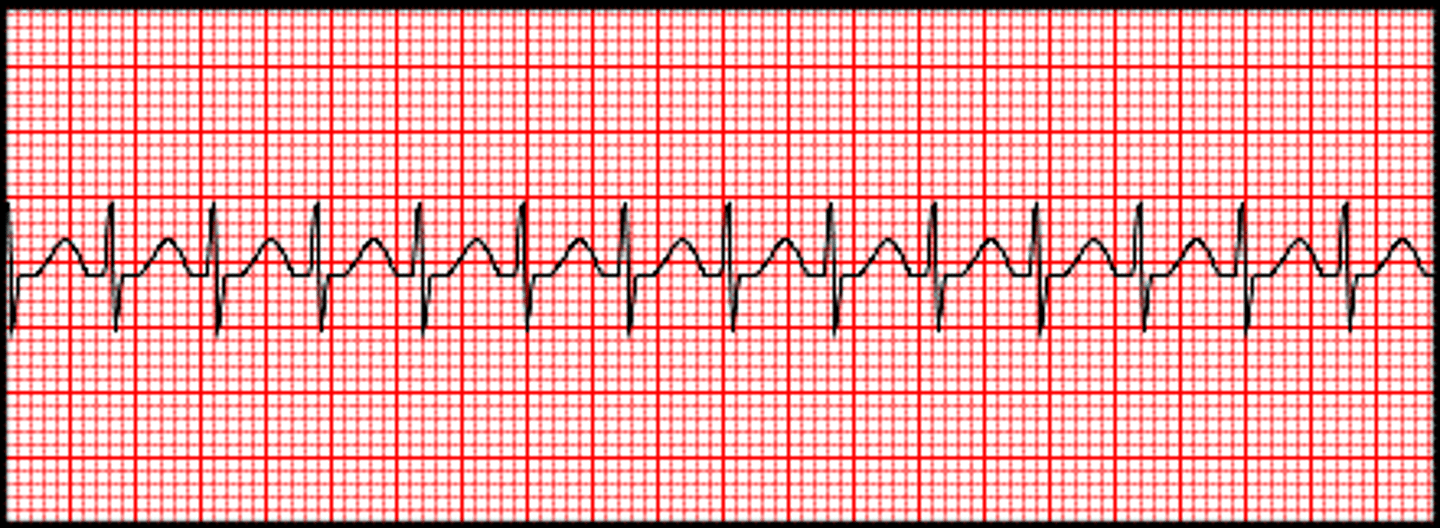
supraventricular tachycardia
•Tachycardic rhythm originating from above the ventricle
•Atrial or junctional
•Regular, narrow complex QRS, P waves not visible
SVT
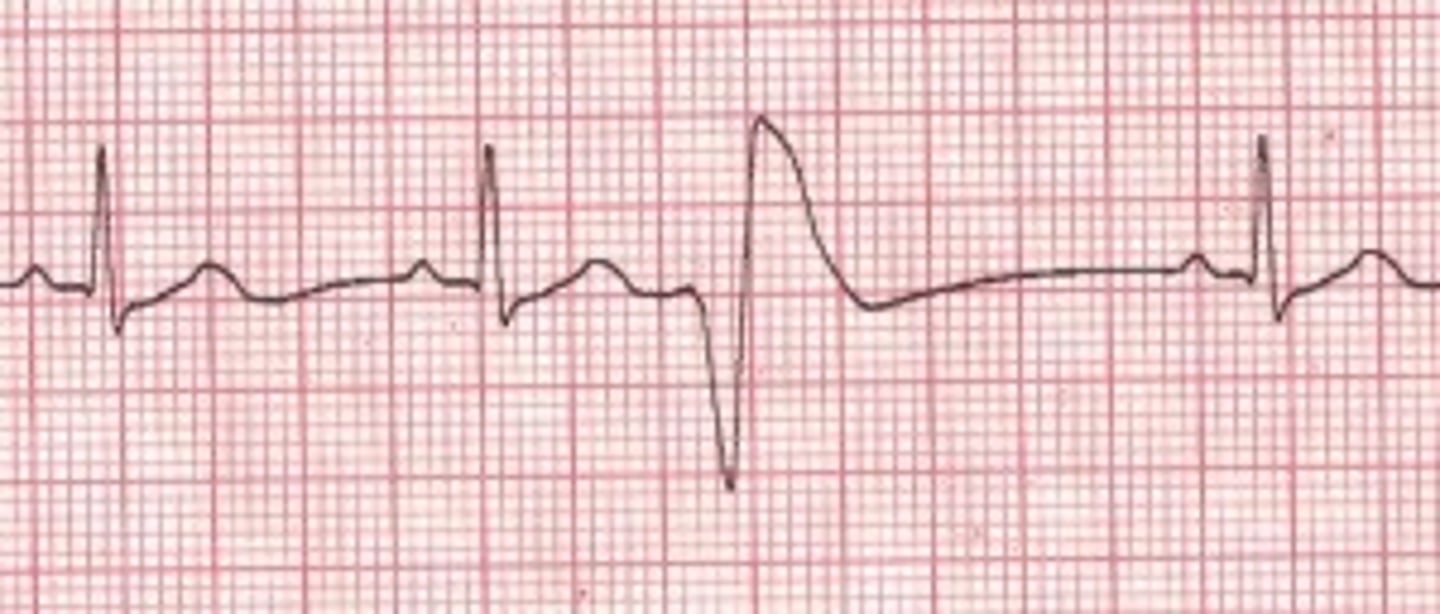
premature ventricular contraction
•Premature stimulus that originates from an irritable ventricular focus
•Wide QRS, increased amplitude
•Unifocal or multifocal
PVC
ventricular tachycardia
•Sudden rapid firing of an irritable ventricular focus
•AV dissociation
ventricular tachycardia
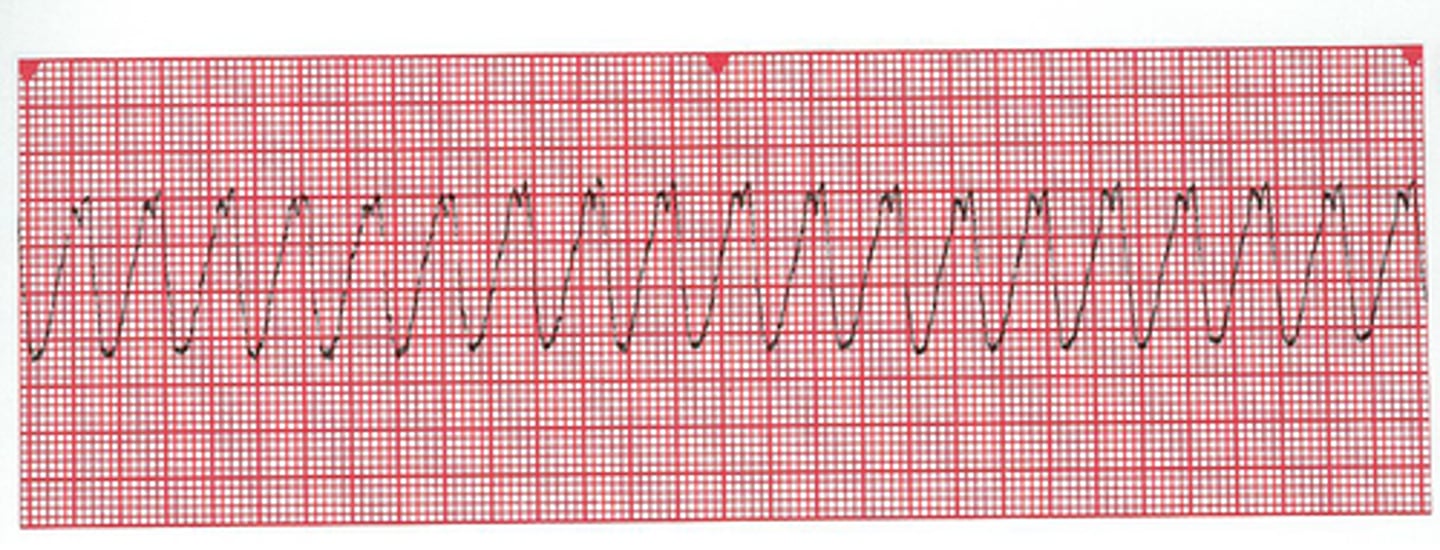
torsades de pointes
oPolymorphic VT
oCaused by hypokalemia, long QT syndrome