week 10
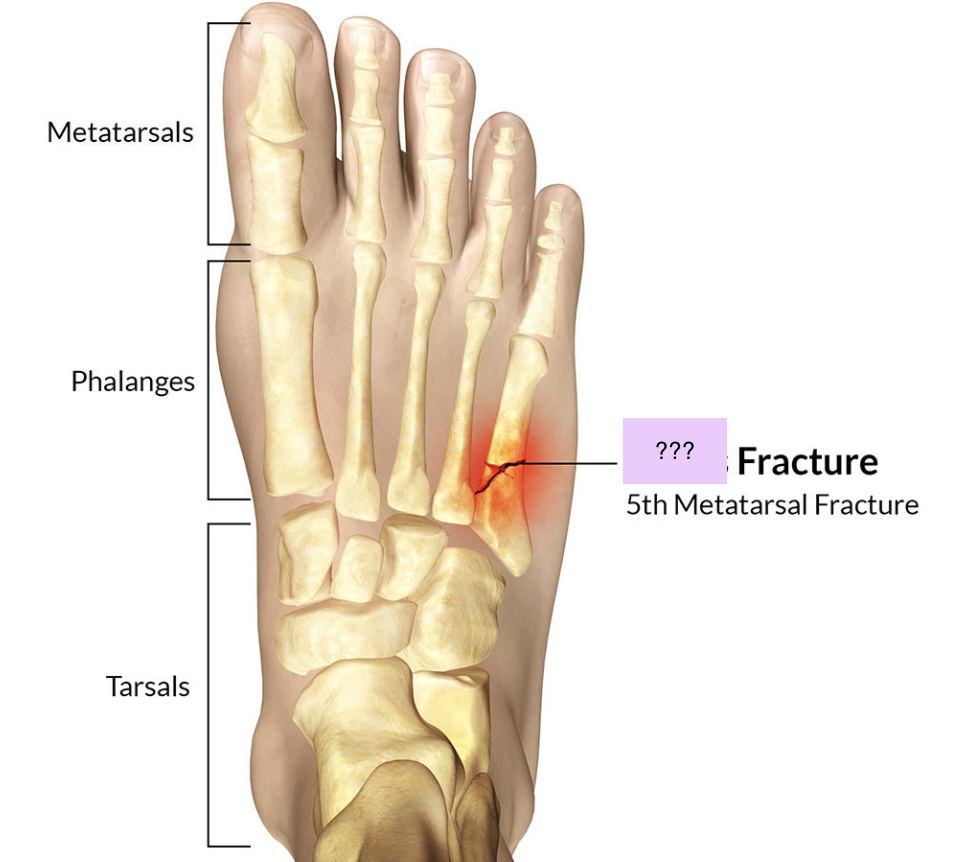
fracture
a break in a bone from force applied that exceeds its tensile or compressive strength
causes of bone fractures
Fractures caused by sudden injury
Fatigue or stress fractures
Pathologic fractures
complete fracture
bone is broken all the way through
incomplete fracture
bone is damaged but still in one piece
closed (simple)
Non-communicating wound between bone and skin
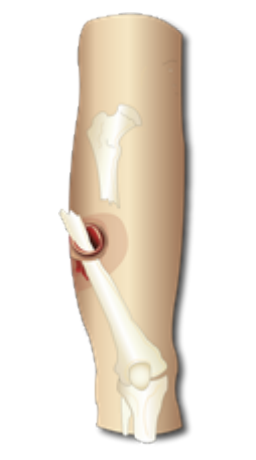
Open (compound)
Communicating wound between bone and skin
Comminuted
Three or more bone fragments
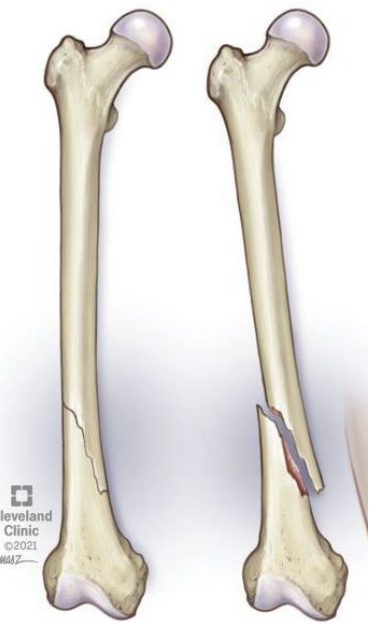
Oblique
Fracture line at an angle to long axis of bone
Transverse
Fracture line perpendicular to long axis of bone
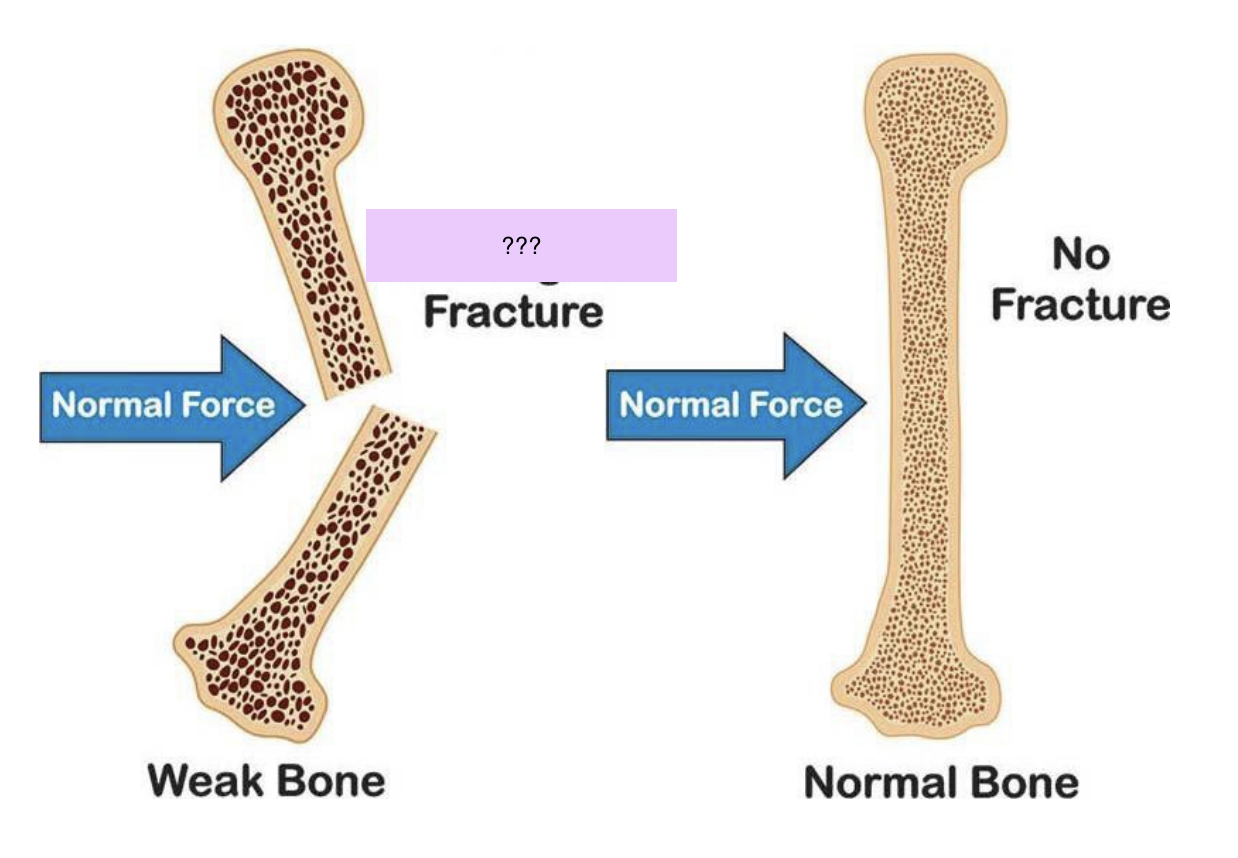
Pathological
Fracture at a point where bone has been weakened by disease (e.g. by tumours or osteoporosis)
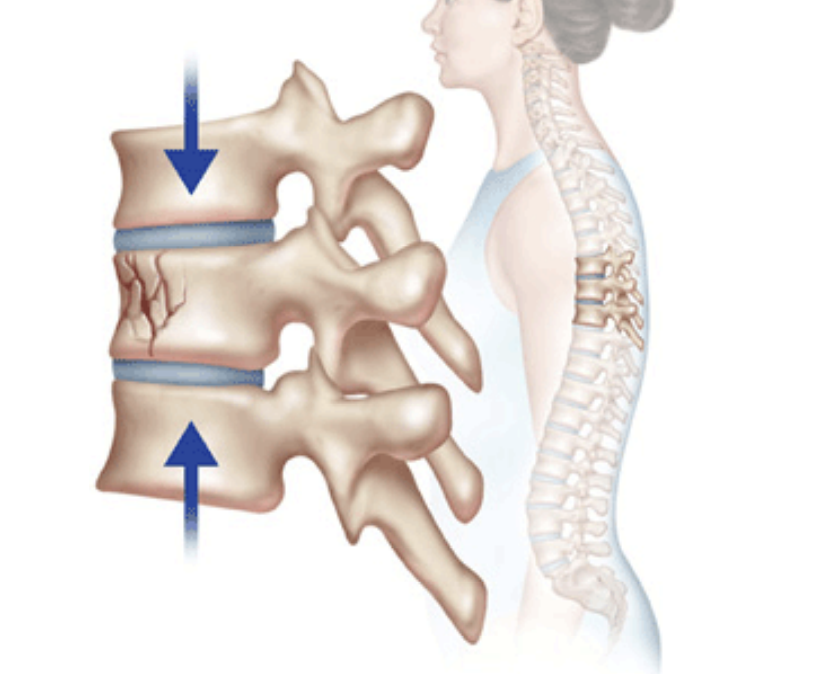
Compression
Fracture wedged or squeezed together on one side of bone
Displaced
Fracture with one, both or all fragments out of normal alignment
Greenstick
Incomplete
Break in one cortex of bone with splintering of inner bone surface; commonly occurs in children
Stress
Incomplete
Microfracture
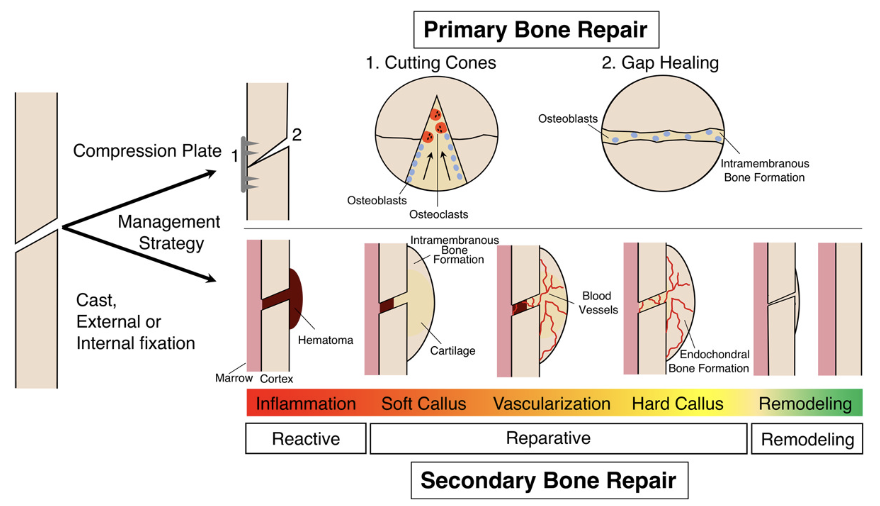
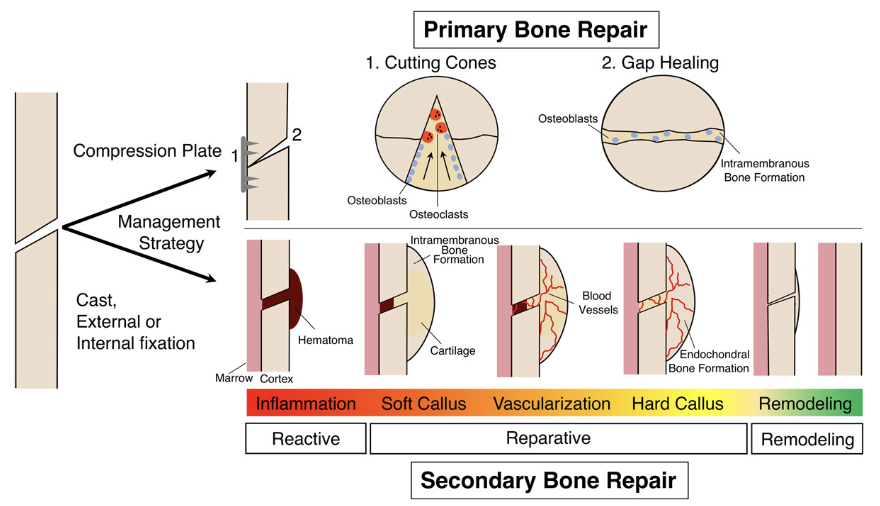
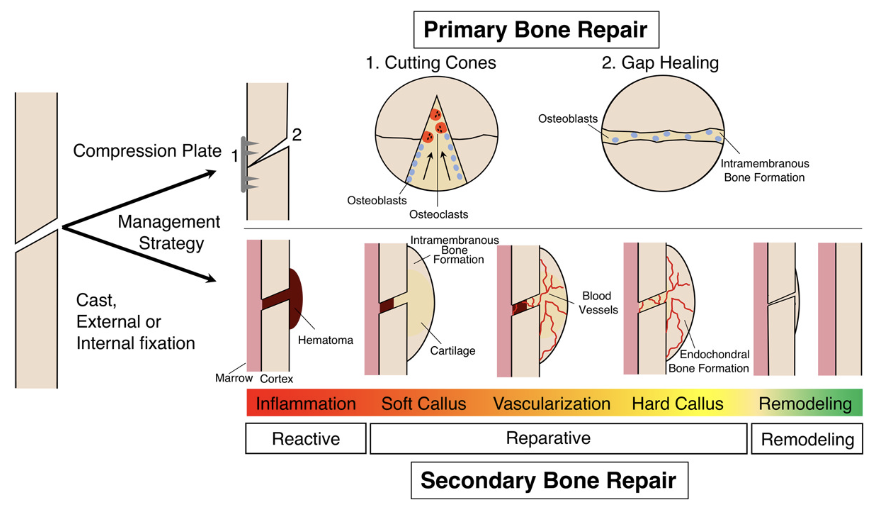
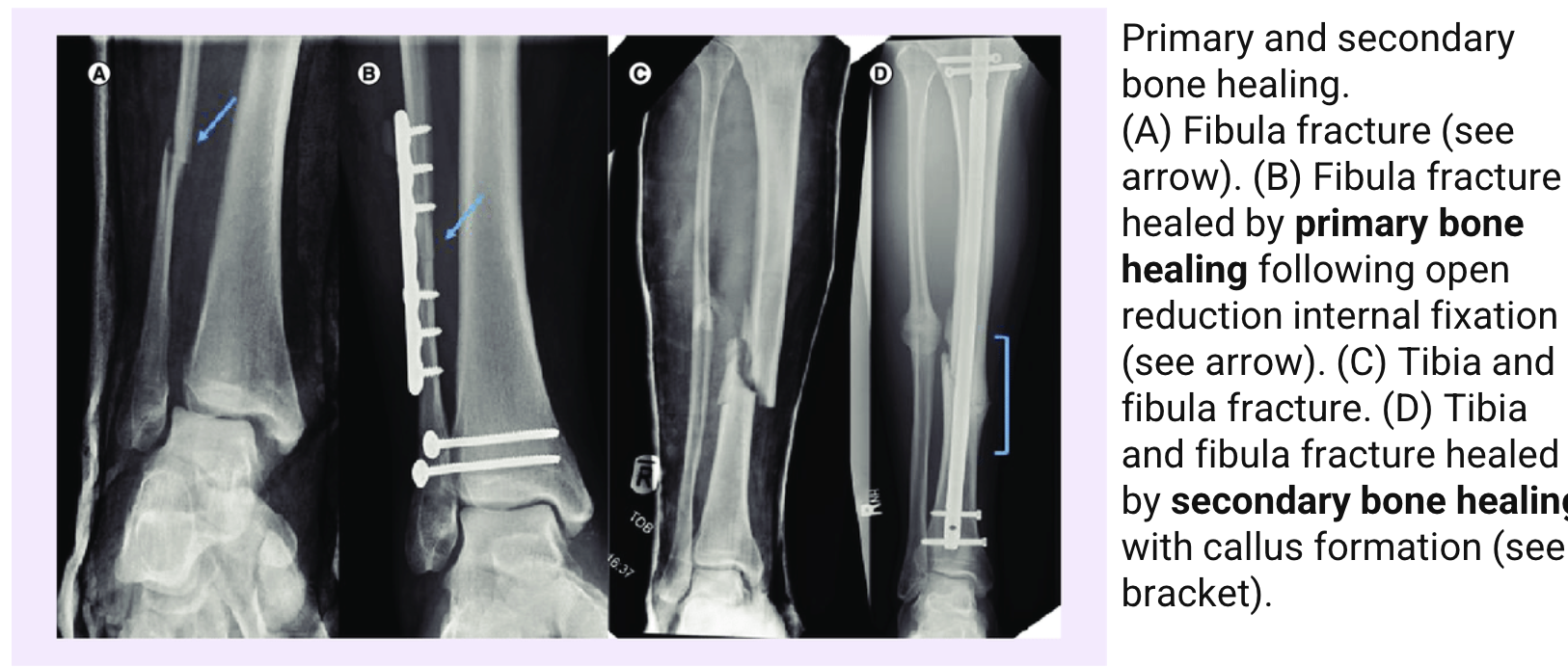
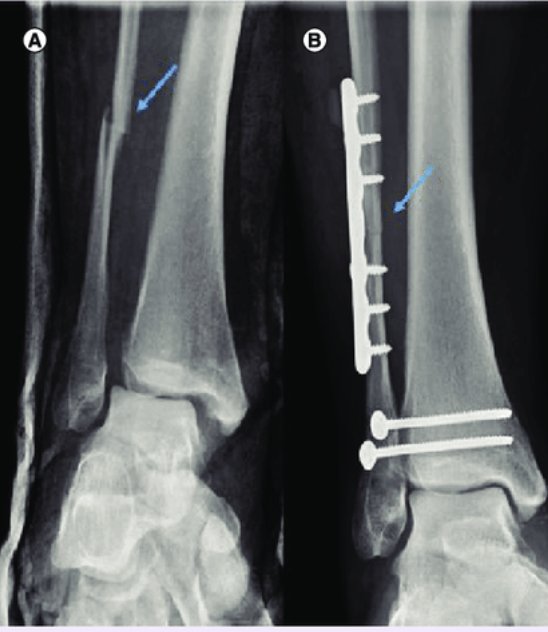
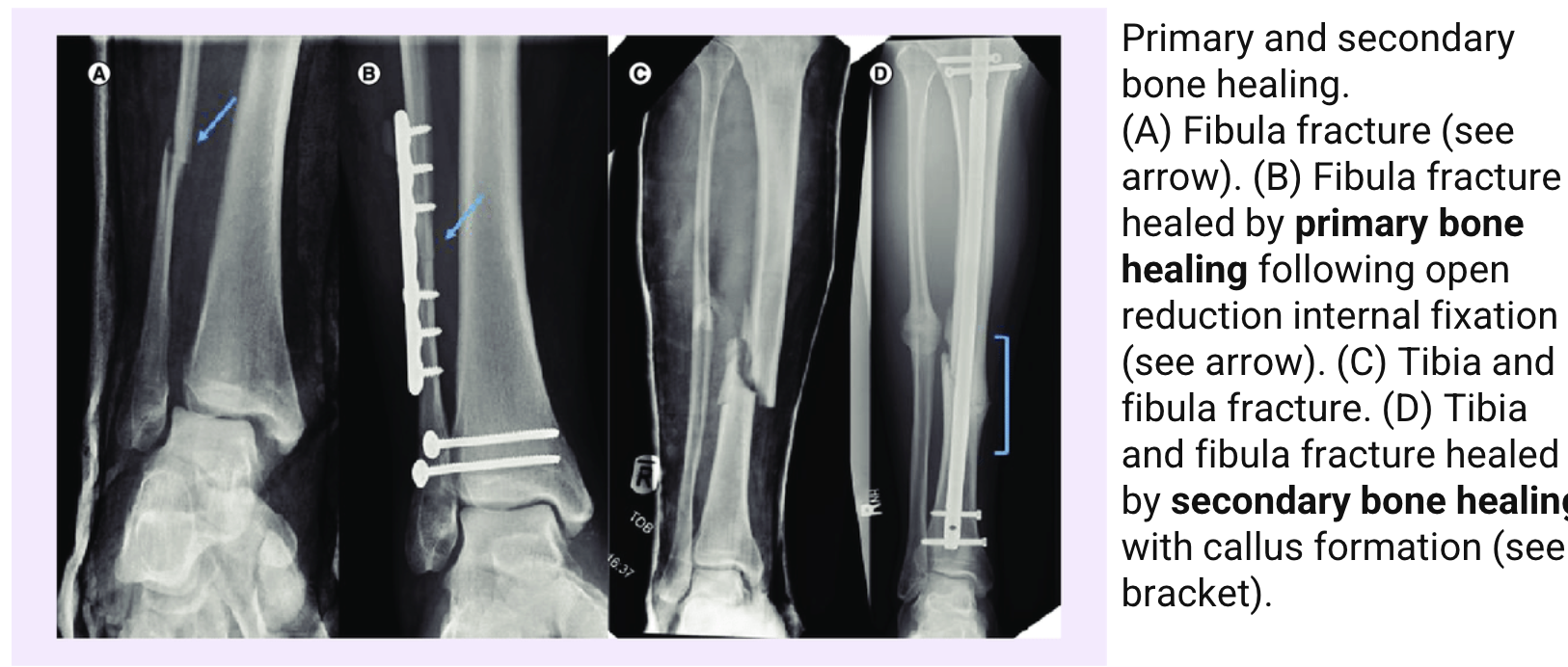
direct/primary bone healing
micro gap <1mm:
little to no callus formations
Haversian remodelling osteoblast/osteoclast activity
when bone ends are held close together → intramembranous bone formation
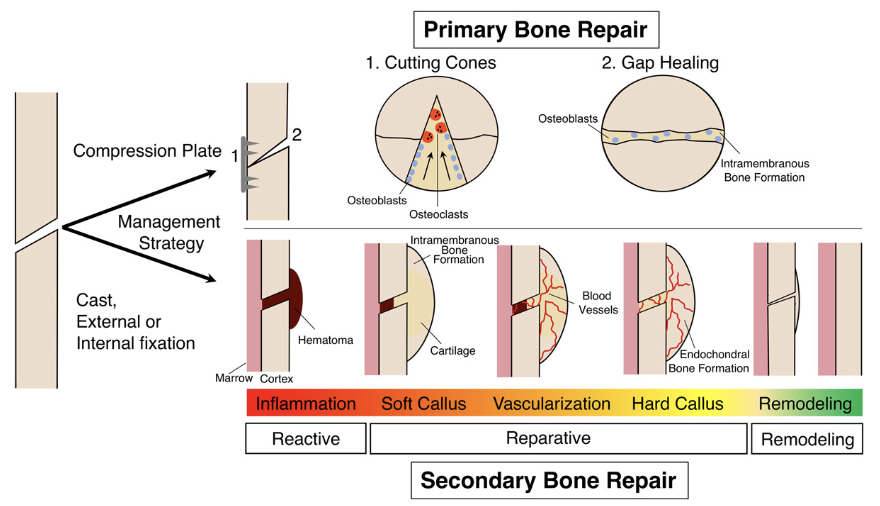
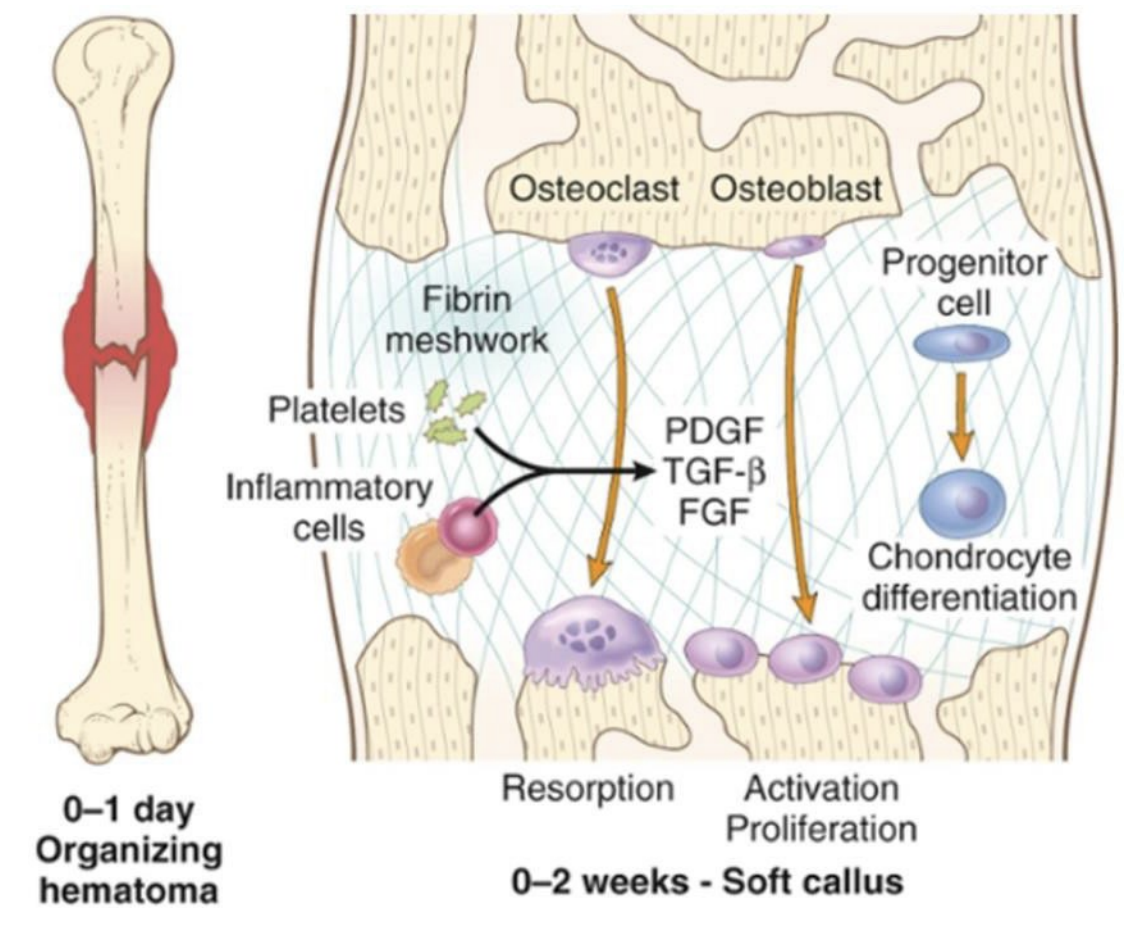
indirect/secondary bone healing
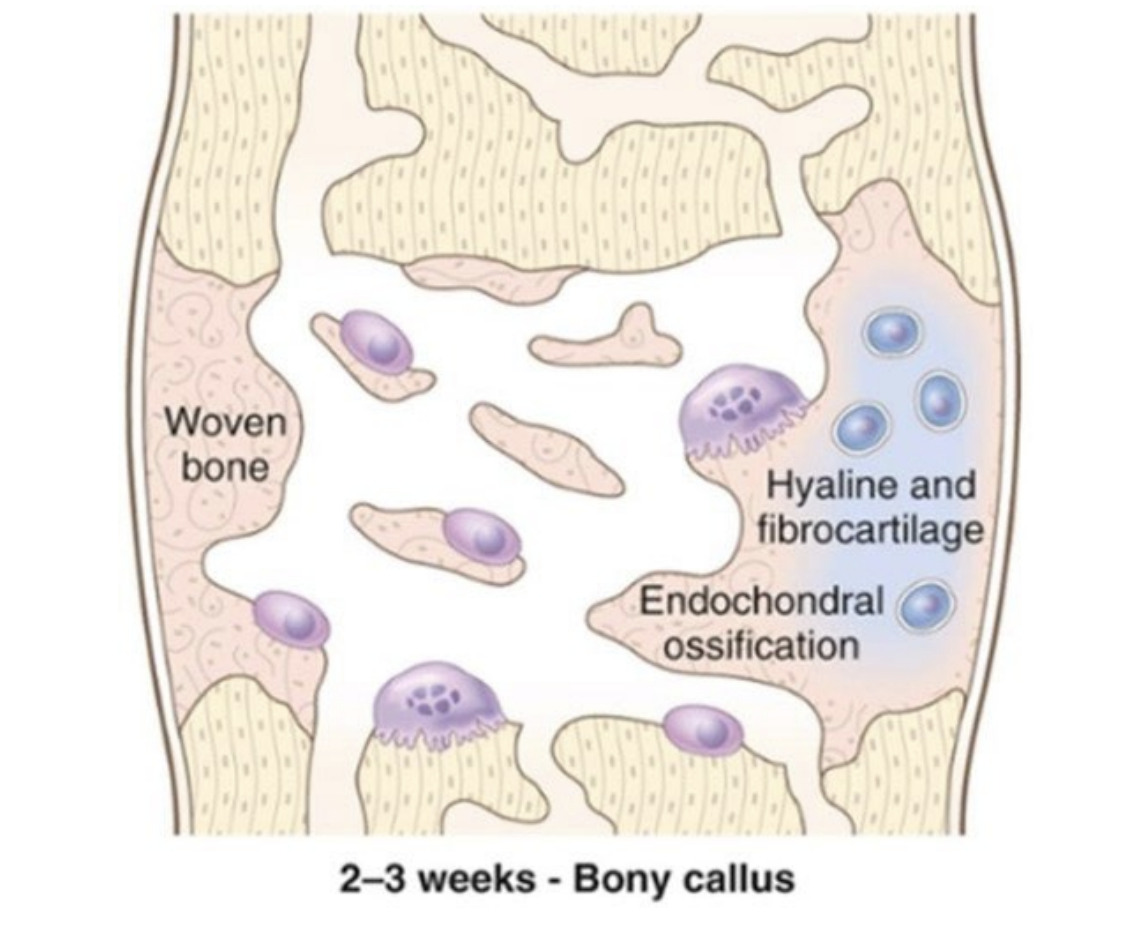
gap >1mm: callus formation
more common than direct healing and involves endochondral healing
heals in four phases:
Haematoma Phase
Inflammatory Phase
Reparative Phase
Remodelling Phase
fracture: phase of secondary healing?
Phases 1-2: haematoma and inflammatory phase
hours - days
(haema-toma=blood-cut: pool of clotted blood outside the blood vessel)
fracture: phase of secondary healing?
Phase 3 - reparative phase
days - weeks
fracture: phase of secondary healing?
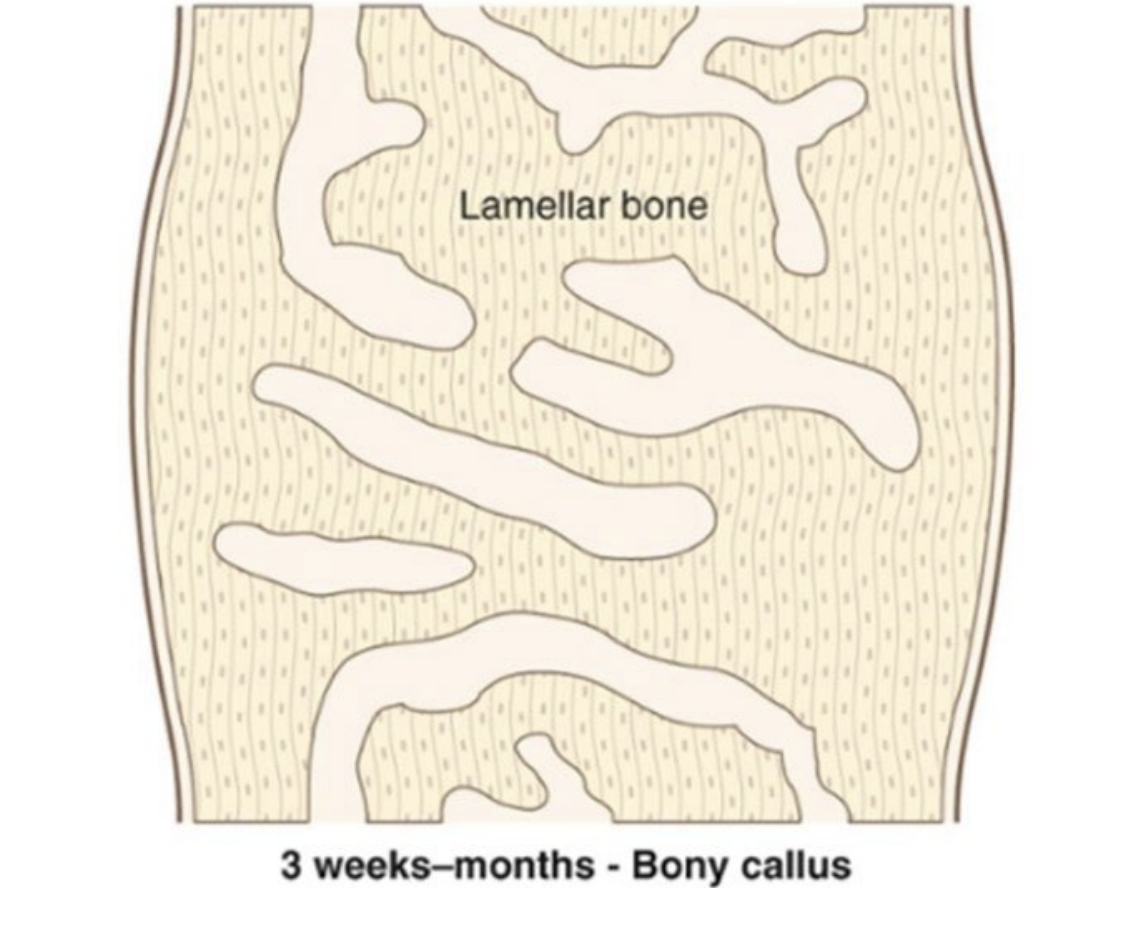
Phase 4 - remodelling phase
months - years
components of tissue repair
Cells
Cytokines & Growth factors (GF)
Extracellular matrix (ECM)
types of cells in tissues
labile
stable
permanent
labile tissues
high turnover and good proliferative capacity
continuous replacement by stem cell proliferation
e.g. skin
stable tissues
slow or limited proliferation rate
cells only proliferate when injured
e.g. liver
permanent tissues
non/minimally proliferative
terminally differentiated cells
not sufficient to replace lost tissue
e.g. cardiac muscle cells
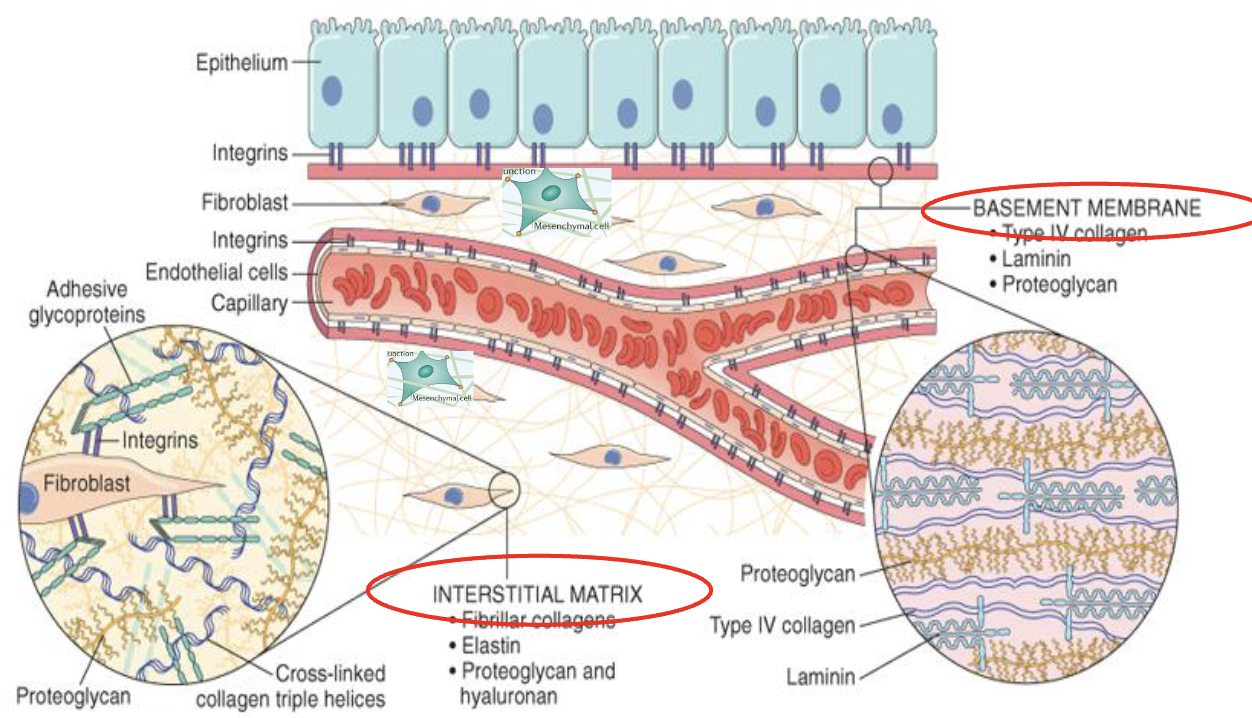
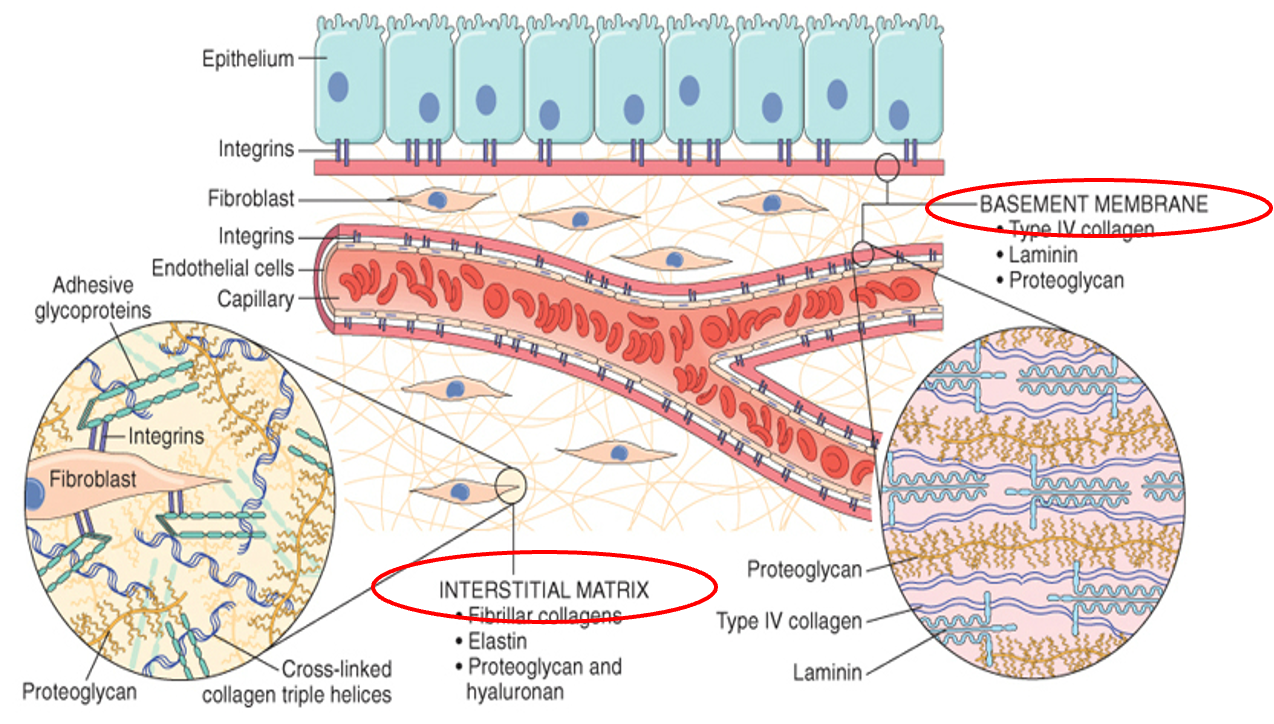
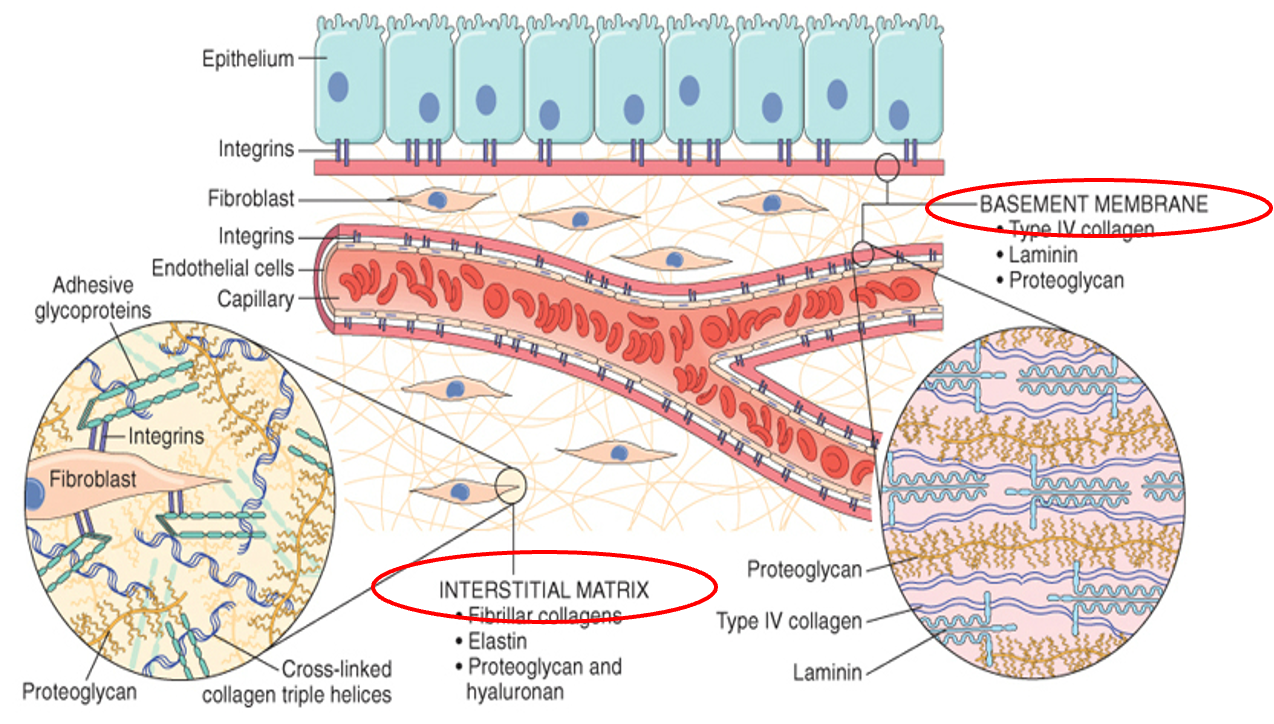
extracellular matrix
Intact or preserved ECM is important for regeneration otherwise healing occurs by scar formation (fibrosis)
2 basic components:
Interstitial matrix
Basement membrane
scaffold for tissue repair
reservoir of growth factors
Cross linking of collagen is Vitamin C dependent
interstitial matrix
amorphous gel-like structure suspending cell/tissue types
between epithelial and endothelial tissues
Loose or dense connective tissue
basement membrane
surface structure supporting tissues
holds epithelial and endothelial tissues
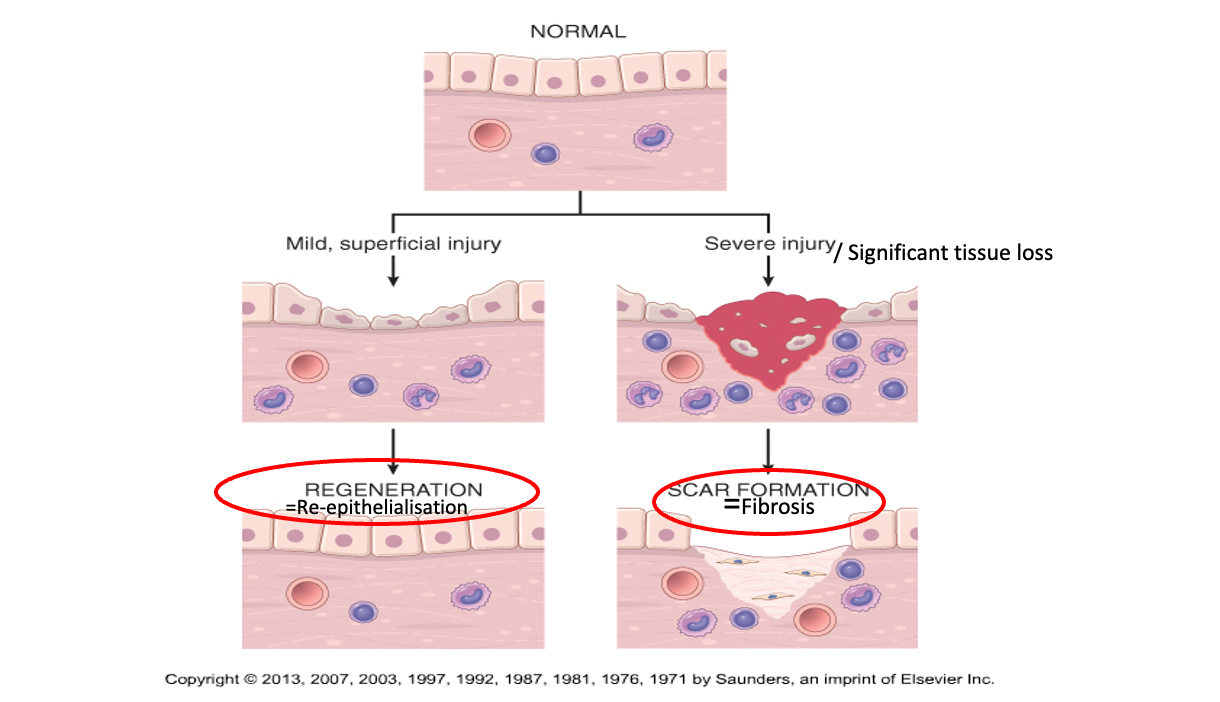
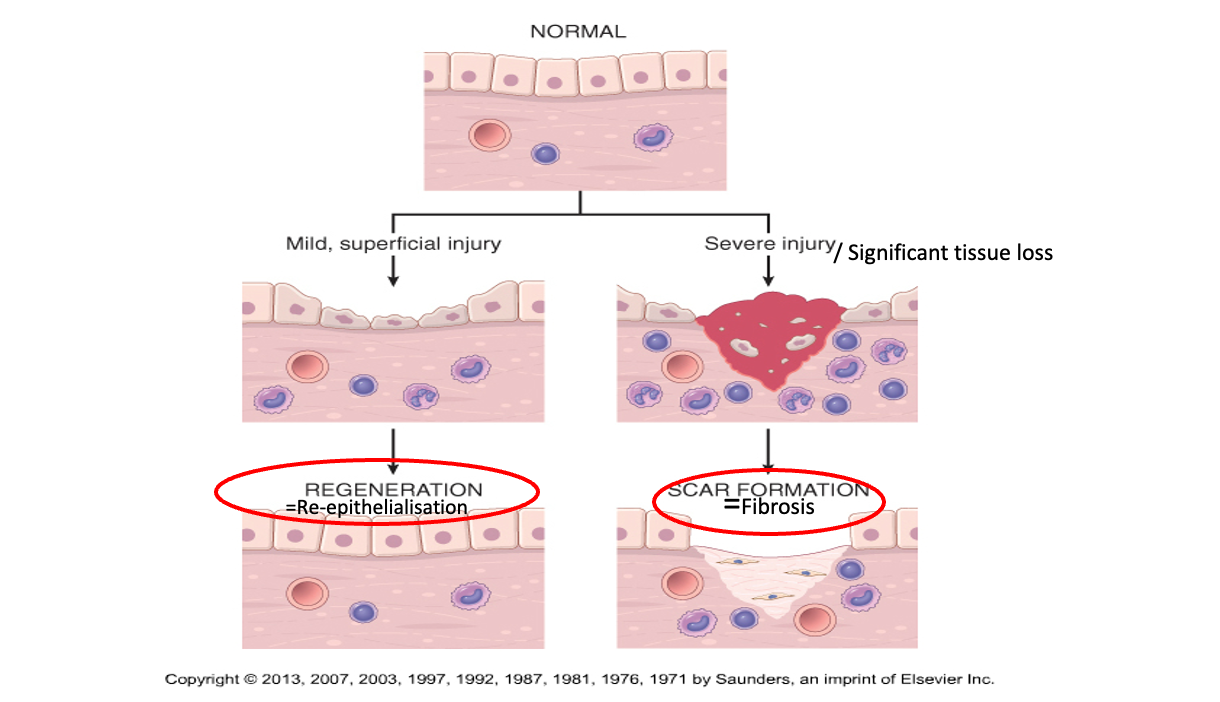
healing by regeneration/re-epithelialisation
Stem cells proliferate to replace the damaged cells
Labile cells, minor injury, clean/sutured cuts
No/minimal residual damage
e.g. skin, fetal tissue, GIT, endometrium, bone marrow
healing by scar formation
Stable or permanent cells, large defects,
contaminated wounds
Fibrous tissue to fill the defect: Scar formation/fibrosis
Enough structural strength but loss of function
e.g. liver, kidney, brain, muscle, bone
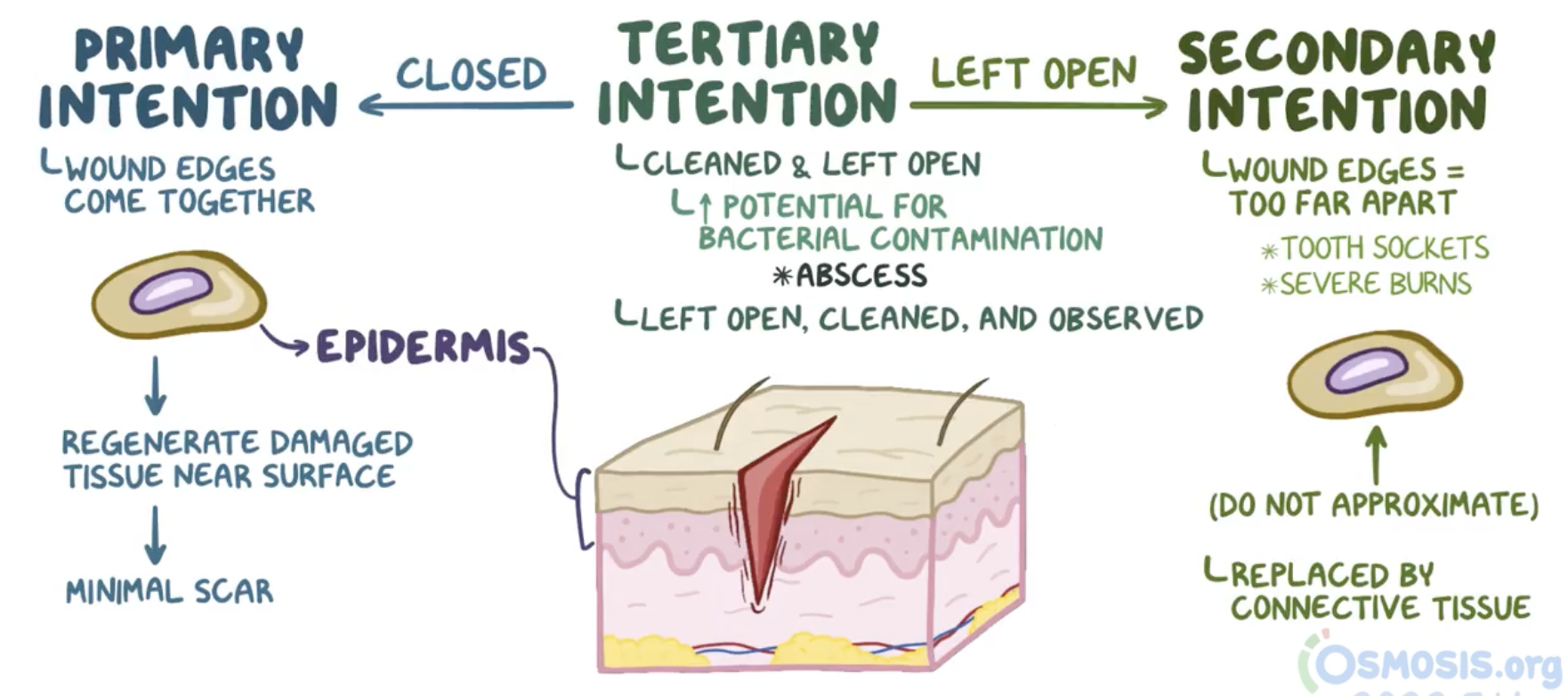
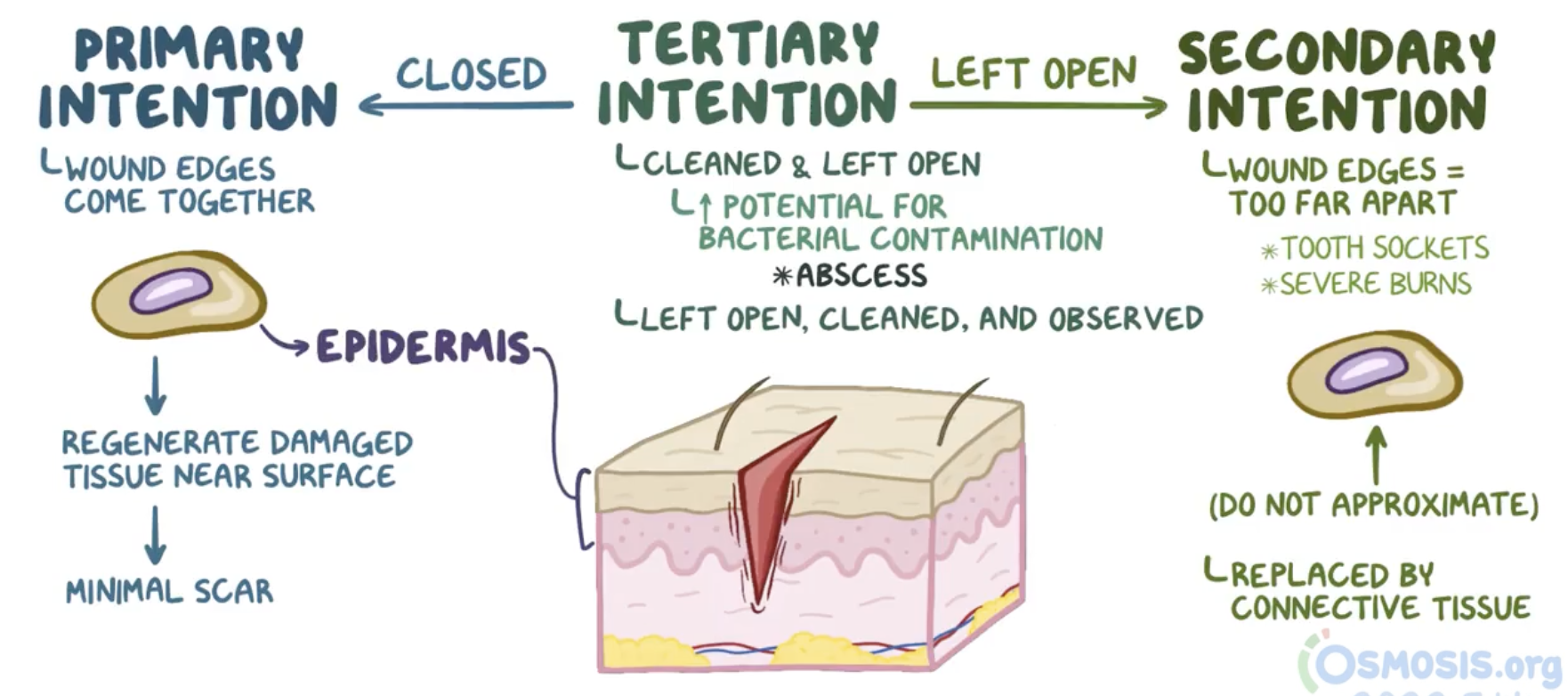
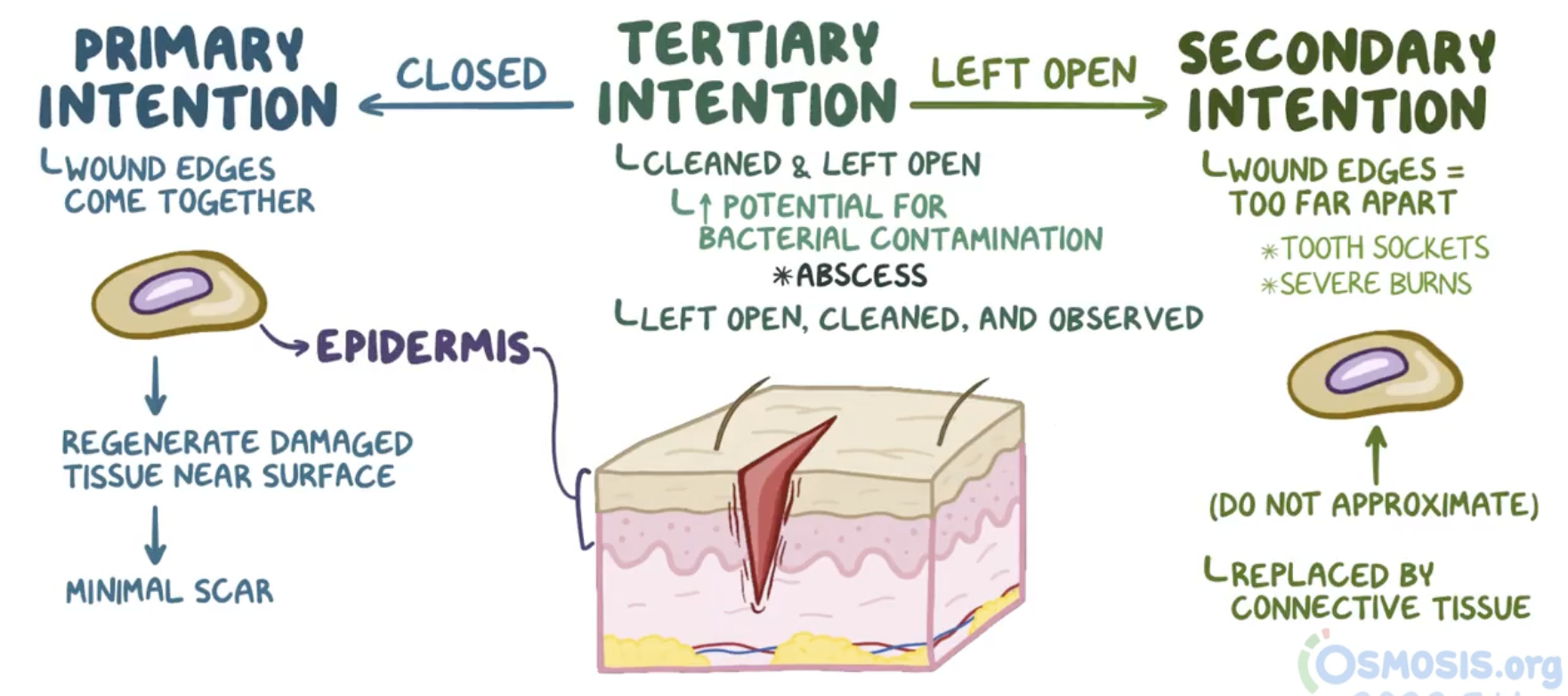
primary intention healing
Minor, clean, sharp cuts or sutured incisions
edges close together
Re-epithelialisation → scarring
e.g. superficial cuts, most surgical incisions
secondary intention healing
Large defects
Wound kept open to granulate, slow healing
more scarring → moderate re-epithelialisation
Packed with gauze/VAC/drains to enhance healing process
e.g. any -ectomy, tooth extraction sockets, compound fractures, venous ulcers, pressure sores
tertiary intention healing
defect too large and contaminated
medical intervention
delayed primary closure:
Wound is cleaned
edges debrided and kept open for 4-7 days
Secondary healing begins/granulation appears
surgically: edges brought closer
E.g.: Tissue grafting sites, highly contaminated/infected, ischaemic/necrotic, etc.
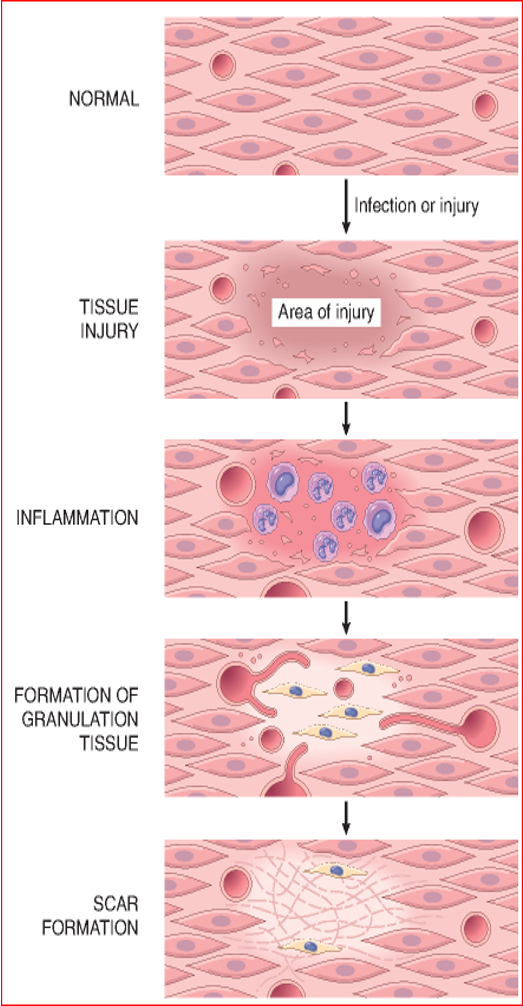
stages of wound repair (superficial, non-complicated wound)
Haemostasis Phase/tissue injury: day 0
Inflammatory Phase: days 1-2
Proliferative Phase: days 3-5
formation of granulation tissue
angiogenesis: formation of new blood vessels
maturation phase: 4-24 days
or
secondary intention: scar formation: day 7
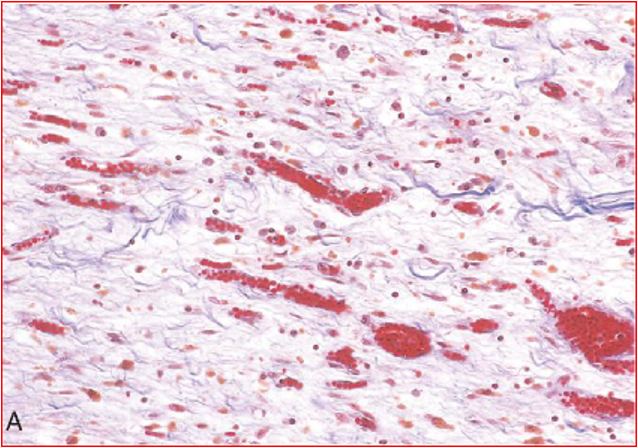
granulation tissue
Pink granular tissue at the wound base (floor)
Granularity due to new vessel buds
felt as knobs
blood flow → increased pink/red colour to tissue
New vessels are thin and fragile hence leaky
serum in oedematous loose ECM
Pink base with some serous ooze – moist wet wound = healthy
primary intention wound strengthening time period (when can I lift /go back to heavy work?)
10% strength - 1 week
80% strength - 3 months
secondary/tertiary intention wound strengthening time period (when can I lift /go back to heavy work?)
10% strength - months to a year
80% strength - many years to never
steroids and wound healing
inhibit the activity of matrix metalloproteinases (MMPs), enzymes critical for extracellular matrix (ECM) remodeling
leads to weak or delayed ECM repair/epithelialisation
wound healing depends on
Wound type
Cell/Tissue type: Proliferative capacity
Growth factors
Preservation of ECM
Healing factors
Nutritional status (important for collagen synthesis, e.g. vitamin c for collagen maturation and cross-linking)
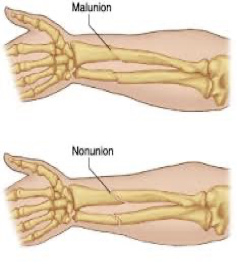
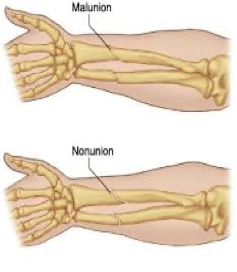
malunion
two broken edges at the ends of the bones are not aligned
bone heals in awkward position
nonunion
the bone fragments are not healing together
no replacement of lost bone - gap persists
day? stage?
inflammation
first couple of days
note: scab formation starts within first few days and persists until 3-5
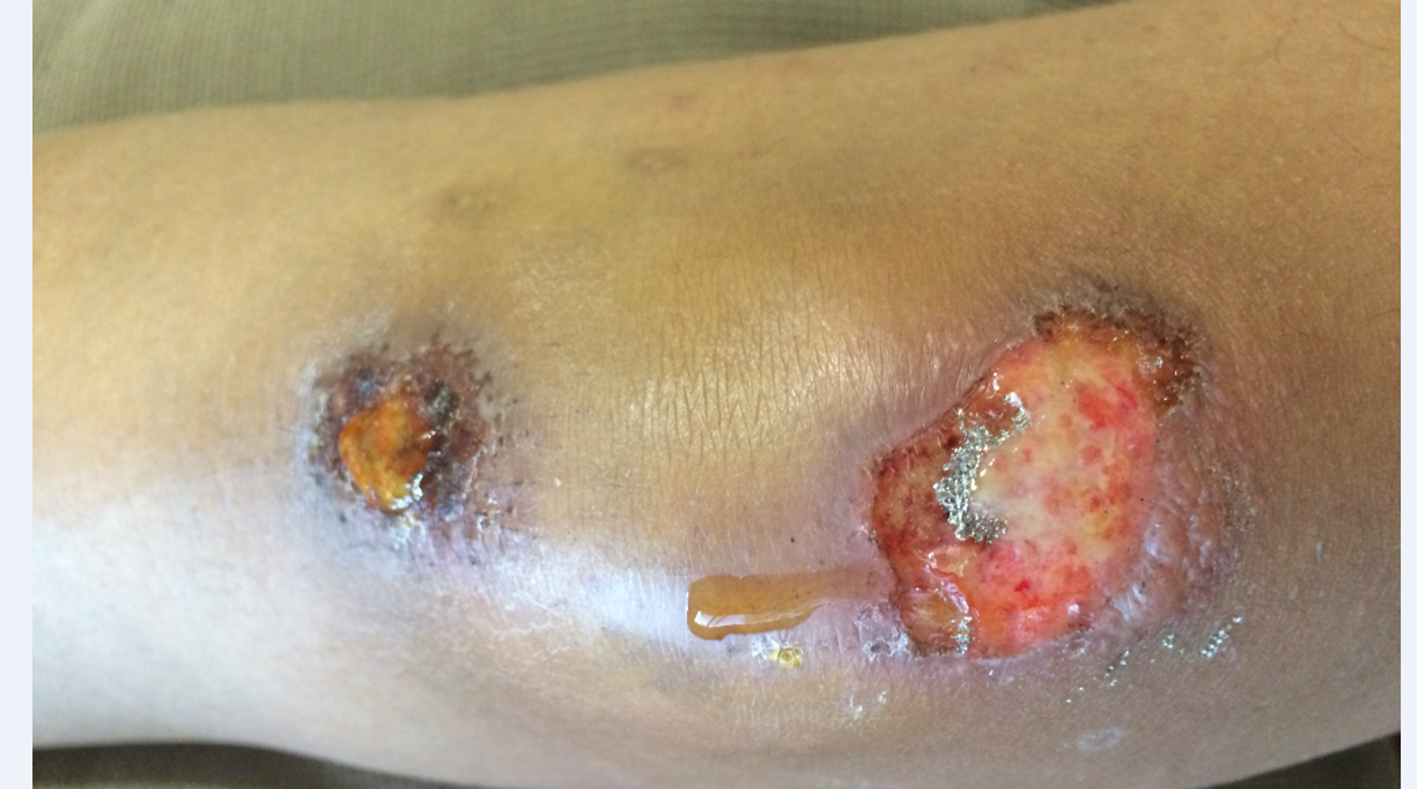
stage?
ulcer, serous discharge
proliferative: granulation tissue (little unhealthy)
stage? day?
scab is off
some swelling but not confined to injury site
maturation/scar formation:
granulation almost gone
start of re-epithelialisation
7 days or more
stage? day?
tissue stabilised
puckered border: scar has contracted
weeks-a month
type of healing
secondary bone healing
Hypertrophic scar
raised scar due to collagen overproduction
scar remains within the boundaries of the wound
keloid
raised scar due to collagen overproduction
scar extends outside the boundaries of the wound
scar formation stages
Laying of connective tissue on the granulation tissue/loose ECM scaffold
Myofibroblasts migrate and proliferate
Deposition of ECM
Inhibit collagen degradation
Cells: macrophages, mast cells and granulation tissue cells
Growth factors: TGF-β, PDGF, FGF-2 and
Cytokines: IL 1, IL-13
Remodelling of connective tissue: wound strengthening
Balance between MMPs (collagen degrader) and TIMPS (collagen degradation inhibitor) regulates repair process
hypertrophy
increase in cell size
metaplasia
change in cell type
hyperplasia
increase in cell number
atrophy
decrease in cell size or number
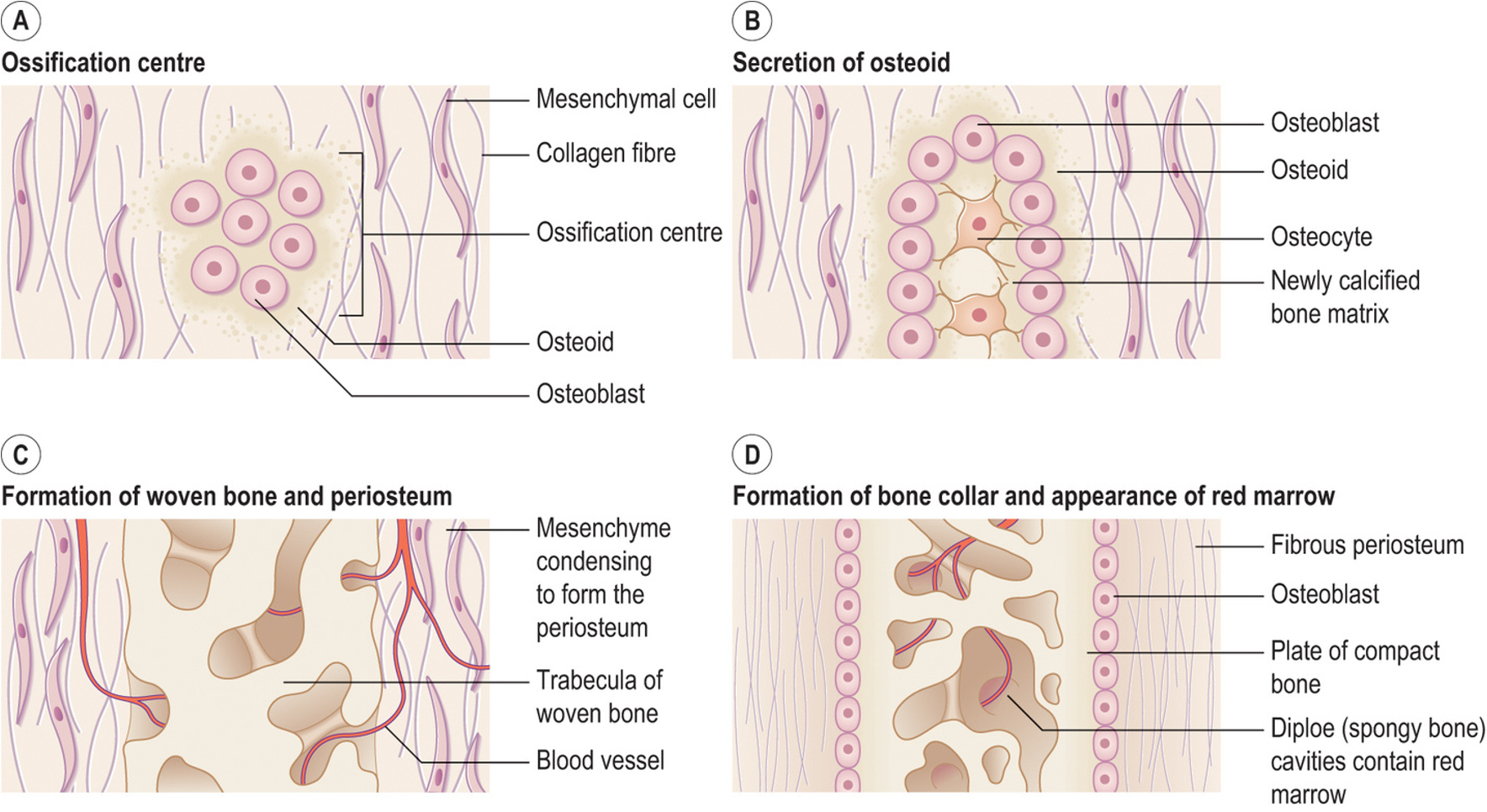
intramembranous bone formation stages
ossification centre formation
mesenchymal cells differentiate into osteoblasts
secretion of osteoid (matrix)
osteoblasts secrete osteoid
mineralised within days
trapped osteoblasts → osteocytes
formation of woven bone and periosteum
osteoid calcifies → forms trabeculae
vascularised mesenchyme condenses externally → periosteum
formation of bone collar and appearance of red marrow
Trabeculae deep to periosteum thickens, forming woven bone collar (later replaced by lamellar bone)
Spongy bone persist, vascular tissue becomes red marrow
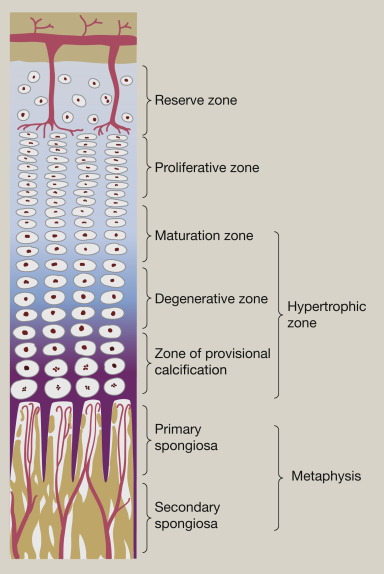
endochondral bone healing
indirect/secondary bone healing
interstitial growth from epiphyseal plate:
Zone of Resting (Reserve) Cartilage:
Chondrocytes are small, inactive, and serve as a reserve for future growth.
Zone of Proliferation:
Chondrocytes actively divide and form columns, increasing the length of the cartilage.
Zone of Hypertrophy:
Chondrocytes enlarge (hypertrophy), and their lacunae expand.
Zone of Calcification/Degeneration
The cartilage matrix becomes calcified, and the chondrocytes die, leaving spaces for bone-forming cells.
Zone of Ossification:
Osteoblasts invade the calcified cartilage and deposit bone matrix, converting cartilage into bone tissue.