CBSSA Form 31
1/403
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
404 Terms
Midsystolic click heard at fifth intercostal space left midclavicular line (apex)
Diagnosis: Mitral valve prolapse (MVP)
Pathology: Myxomatous degeneration leading to thickened leaflets, chordae tendineae rupture, or mitral annular disjunction.
Key Associations: Young females, Marfan syndrome, Ehlers-Danlos syndrome, adult polycystic kidney disease, systemic lupus erythematosus (SLE).
Fixed split S2 sound and low grade physiologic systolic ejection murmur
Diagnosis: Atrial septal defect (ASD)
Mechanism: Left to right shunt causing volume overload of the right atrium and right ventricle.
Crescendo decrescendo systolic murmur best heard at upper right sternal border radiating to carotids
Diagnosis: Bicuspid aortic valve with stenosis
Clinical Pearl: Typically presents early in adulthood.
Subtle diastolic murmur with risk for adult arterial thromboembolic disease (paradoxical emboli)
Diagnosis: Patent foramen ovale (PFO)
Mechanism: Failure of the fetal right to left shunt to close completely.
Holosystolic murmur best heard at left lower sternal border
Diagnosis: Tricuspid regurgitation
Key Associations: Severe pulmonary hypertension or infective endocarditis from intravenous drug use.
Patient acknowledges behavior is detrimental and wants to quit sometime in the next 6 months but feels ambivalent or indecisive
Stage of Change: Contemplation
Key Interviewing Technique: Motivational interviewing using open ended, nonjudgmental questions to help the patient explore reasons for wanting to change versus maintaining the habit.
Patient is not interested in changing behavior, does not see the habit as a problem, or denies having a problem
Stage of Change: Precontemplation
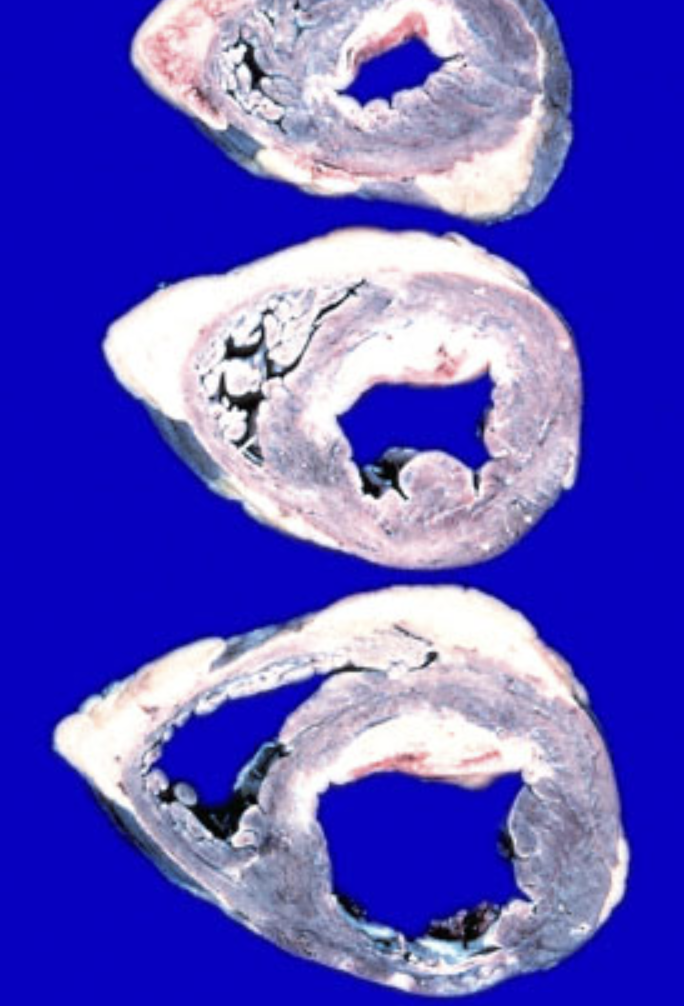
Autopsy of heart showing ventricular hypertrophy and large pale white areas of scar tissue or fibrosis
Diagnosis: Congestive heart failure resulting from repeated infarcts
Cellular Mechanism: Cardiomyocytes lack satellite cells and cannot regenerate after injury. Infarcted cardiac tissue heals via fibrosis (scar formation), which impairs contractility.
Contrast with Skeletal Muscle: Skeletal muscle contains quiescent satellite cells between the sarcolemma and basal lamina that proliferate via cytokines (interleukin 1, insulin like growth factor 1) to repair or form new myofibers.
Autopsy of heart showing right ventricular hypertrophy without significant left ventricular scarring
Diagnosis: Pulmonary stenosis
Mechanism: Chronic increased resistance and pressure overload against the right side of the heart.
Autopsy of heart showing a physical tear or defect in the interventricular septum, often with a thrombus in the left anterior descending artery
Diagnosis: Septal rupture
Clinical Consequence: Acute left to right shunt causing cardiogenic shock.
Effect of sinus tachycardia on the cardiac cycle
Key Relationship: Diastole is shortened more than systole.
Physiological Impact: Because tachycardia disproportionately cuts down diastolic time, ventricular filling time (preload) is significantly decreased. If the heart rate is too high, this can cause a drop in cardiac output and lead to heart failure.
Why the duration of systole remains relatively constant during normal sinus tachycardia
Mechanism: Ventricular systole depends on the active conduction time from the atrioventricular (AV) node through the His-Purkinje system to the ventricular myocytes. This electrical conduction pathway time is not significantly altered by a fast heart rate.
Condition or pathology that causes systole to be prolonged more than diastole
Causes: * Ventricular conduction delays (such as bundle branch blocks)
Increased ventricular afterload (such as severe hypertension or aortic stenosis), which forces the ventricles to pump longer to eject blood
Child with muscle cramping or fatigue during strenuous exercise (sprinting) but tolerates light exercise, showing flat venous lactate curve (no increase in lactic acid) with an increase in ammonia after exertion
Diagnosis: McArdle disease (Glycogen storage disease type V)
Defective Pathway: Glycogenolysis in skeletal muscle
Enzyme Deficiency: Skeletal muscle glycogen phosphorylase (myophosphorylase)
Clinical Consequence: Failure to hydrolyze 1,4-glycosidic bonds to liberate glucose-1-phosphate from glycogen. Leads to muscle breakdown, myoglobinuria (red wine colored urine), and elevated resting creatine kinase.
Infant with severe fasting hypoglycemia, hepatomegaly, increased serum lactate, increased triglycerides, and increased uric acid
Diagnosis: Von Gierke disease (Glycogen storage disease type I)
Defective Pathways: Gluconeogenesis and glycogenolysis in the liver
Enzyme Deficiency: Glucose-6-phosphatase
Infant with hepatosplenomegaly, failure to thrive, and accumulation of abnormally long, unbranched glycogen polymers (structurally unsound glycogen)
Diagnosis: Anderson disease (Glycogen storage disease type IV)
Defective Pathway: Glycogen synthesis branching
Enzyme Deficiency: Alpha-1,4-glucan branching enzyme (fails to create 1,6-glycosidic linkages)
Hypoketotic hypoglycemia, liver dysfunction, vomiting, lethargy, and seizures during periods of fasting or illness
Diagnosis: Medium-chain acyl-CoA dehydrogenase (MCAD) deficiency
Defective Pathway: Beta oxidation
Mechanism: Inability to break down fatty acids into acetyl CoA to drive ketone body synthesis and gluconeogenesis during fasting.
Hemolytic anemia triggered by oxidative stress (such as sulfa drugs, fava beans, or infections) showing Heinz bodies and bite cells on blood smear
Diagnosis: Glucose-6-phosphate dehydrogenase (G6PD) deficiency
Defective Pathway: Pentose phosphate pathway (hexose monophosphate shunt)
Mechanism: Decreased production of NADPH, leaving red blood cells vulnerable to oxidative damage.
Study design that identifies a group based on exposure status (such as oral contraceptive users vs tubal ligation) and follows them over time to measure the incidence of an outcome (such as cervical cancer)
Design: Cohort study
Key Metric: Relative risk (compares incidence of disease between exposed and unexposed groups). Can be prospective or retrospective.
Study design that identifies a group of individuals with a disease and compares them to a matched group of individuals without the disease to look back at past exposure history
Design: Case control study
Key Metric: Odds ratio (estimates the odds of exposure in cases compared to controls)
Study design that simultaneously measures both the exposure and the outcome of interest in a population at a single specific point in time
Design: Cross sectional study
Key Metric: Prevalence (provides a snapshot of the population, cannot establish temporal relationships or causality).
Experimental study design where patients are randomly assigned to an intervention or control arm and followed forward to evaluate efficacy
Design: Randomized clinical trial (RCT)
Clinical Value: Randomization minimizes selection bias and confounding, making it the gold standard for establishing a direct cause and effect relationship.
Descriptive study design that details the clinical course, presentation, and characteristics of a small collection of consecutive or nonconsecutive patients with a specific disease
Design: Case series
Clinical Value: Useful for generating hypotheses and characterizing rare conditions, but lacks a control group and cannot establish causation.
Acute episode of fever, cough, chills, and shortness of breath starting several hours after baling and storing moldy hay on a farm, with symptoms resolving within a few days
Diagnosis: Hypersensitivity pneumonitis (specifically Farmer's lung)
Pathophysiology: Dysregulated type three (immune complex) and type four (delayed hypersensitivity) immunologic response to inhaled dust and mold spores (such as thermophilic actinomycetes).
Chronic Presentation: Repeated exposure leads to a subacute or chronic form presenting with progressive dyspnea, fatigue, weight loss, and interstitial fibrosis on lung biopsy.
Hypersensitivity reaction to a pulmonary fungal infection characterized by worsening asthma, eosinophilia, transient pulmonary infiltrates, and high IgE levels
Diagnosis: Allergic bronchopulmonary aspergillosis (ABPA)
Key Association: Occurs almost exclusively in patients with pre-existing asthma or cystic fibrosis. Can lead to bronchiectasis.
Occupational lung disease in textile workers exposed to cotton, hemp, or flax mill dust, often presenting with chest tightness that is characteristically worse on the first day back to work after a weekend (Monday chest tightness)
Diagnosis: Byssinosis
Mechanism: Direct alveolar injury and histamine release caused by bacterial endotoxins in the cotton dust, rather than a true sensitized hypersensitivity reaction.
Idiopathic interstitial lung disease where alveolar septa are heavily thickened by an infiltration of macrophages, highly associated with tobacco smoking
Diagnosis: Desquamative interstitial pneumonia (DIP)
Key Distinction: Despite the name "desquamative," the cells filling the alveoli are intra-alveolar macrophages, not shed epithelial cells.
Gradual onset of dyspnea, cough, and fatigue where the alveolar spaces become filled with a gelatinous, proteinaceous, PAS positive surfactant material
Diagnosis: Pulmonary alveolar proteinosis (PAP)
Mechanism: Defect in macrophage clearance of surfactant, often due to autoantibodies against granulocyte-macrophage colony-stimulating factor (GM-CSF).
Distinguish between Community, Clinical, Primary, Secondary, and Tertiary health interventions
Community Intervention: Targets an entire population or group in a specific setting (such as a city-wide tax on sugar-based beverages, or school-wide nutrition programs) to influence decision-making at a broad municipal or organizational level.
Clinical Intervention: Takes place directly within a healthcare setting between a provider and an individual patient (such as an office visit for counseling, screening, or medical treatment).
Primary Intervention: Aims to prevent a disease or condition from occurring in the first place (such as encouraging healthy diets to prevent obesity, or giving vaccines).
Secondary Intervention: Focuses on early detection and screening of a disease while it is still subclinical or asymptomatic (such as screening an obese population for silent hypertension or early stage diabetes to catch it before complications arise).
Tertiary Intervention: Focuses on managing, slowing, or ameliorating an already established, symptomatic disease to prevent further complications or disability (such as treating a patient with known diabetes with medications to prevent macrovascular damage).
Low back pain radiating down left posterior thigh, decreased pinprick sensation at lateral foot, and weakness rising on left toes
Diagnosis: S1 radiculopathy
Expected Exam Finding: Achilles tendon hyporeflexia (Achilles reflex is mediated by S1 and S2 nerve roots).
Anatomy: Often caused by herniation of the L5-S1 intervertebral disc.
Presence of gastrocnemius muscle atrophy in a patient with lumbar radiculopathy
Clinical Significance: Indicates a chronic, long-standing nerve root compression rather than an acute or subacute presentation.
Radiculopathy is a lower motor neuron lesion because it affects the nerve root, which contains peripheral motor axons after they leave the spinal cord.
Radiculopathy findings:
LMN weakness in a myotomal pattern
Hyporeflexia/areflexia at the affected root
Flaccid tone early
Atrophy/fasciculations if chronic
Sensory loss/paresthesias in a dermatomal pattern
Radicular pain shooting down the limb
UMN lesion
damage to neuron/pathway before the anterior horn cell or cranial nerve motor nucleus
LMN lesion
damage to the anterior horn cell, cranial nerve nucleus, peripheral nerve, root, or neuromuscular unit
Spinal Cord Lesions
Brainstem Lesions
Anterior Horn Cells Vs Costicospainal Tract
Anterior Horn Cells: LMK
Corticospinal Tract: UMN
Crop duster spill + abdominal pain, salivation, wheezing, diaphoresis, bradycardia, muscle weakness -> Diagnosis and Treatment?
Organophosphate poisoning (e.g., Parathion, Malathion, Fenthion)
Mechanism: Irreversible AChE inhibition -> massive ACh buildup at muscarinic and nicotinic receptors
Treatment: Atropine (blocks muscarinic symptoms like wheezing/salivation) + Pralidoxime/2-PAM (regenerates AChE to fix nicotinic muscle weakness)
How does Carbaryl toxicity differ from Organophosphate poisoning?
Carbaryl is a carbamate insecticide that causes reversible/transient AChE inhibition -> results in shorter duration and milder cholinergic symptoms.
Crop duster chemical exposure + severe lung injury/pulmonary fibrosis and multiorgan failure but NO cholinergic symptoms -> Agent?
Paraquat (herbicide that causes toxicity via free radical production; lacks the DUMBBELSS/nicotinic symptoms of organophosphates)
Granulomatosis with Polyangiitis
GPA is a systemic necrotizing vasculitis that presents with c-ANCA, upper/lower respiratory tract issues (nasal ulcers, hemoptysis), and renal involvement (hematuria/glomerulonephritis).
Patient with ulnar deviation, swan neck deformities, and subQ nodules on forearms -> What is the underlying diagnosis?
Rheumatoid arthritis (RA).
What is characteristically found on pleural fluid analysis in an RA-associated pleural effusion?
Exudative fluid with critically LOW glucose levels (often less than 30 mg/dL) due to high metabolic activity and impaired transport.
Patient with classic Rheumatoid Arthritis deformities + history of being raised in a coal mining community + diffuse fibronodular lung infiltrates -> Diagnosis?
Caplan syndrome (Rheumatoid Arthritis combined with Pneumoconiosis).
Rheumatoid Arthritis (RA) -> Diagnosis, presentation, key genotype, and core pathophysiology/treatments?
Key Presentation: Symmetric arthritis of wrists/hands (swan neck, ulnar deviation), painless nodules on extensor surfaces, and extra-articular manifestations like exudative pleural effusions (characteristically critically LOW glucose, elevated LDH).
Genotype Association: HLA-DR4.
Core Pathophysiology: Tumor necrosis factor (TNF) is the central driver. It activates macrophages and neutrophils, increasing their cytotoxic effects and endothelial adhesion molecule expression to promote migration into peripheral tissues.
Biologic Treatments: TNF-alpha inhibitors (Adalimumab, Etanercept, Infliximab).
Non-Biologic DMARDs: Methotrexate, Hydroxychloroquine, Sulfasalazine.
Polymyalgia Rheumatica (PMR) -> Core presentation, key lab markers, associated condition, and treatment?
Muscle pain and stiffness in the proximal joints/muscles (shoulders, hips, neck) in older adults, often accompanied by weight loss or fever.
Lab Markers: Elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels.
Crucial Association: Highly associated with Giant Cell Arteritis (temporal arteritis), which can cause permanent blindness.
First-line Treatment: Low-dose systemic corticosteroids (prednisone), which typically results in rapid, dramatic symptom relief.
Middle-aged woman + pruritus (itchy skin with excoriations), scleral icterus, elevated Alk Phos, and antimitochondrial antibodies -> Diagnosis and associated complication?
Diagnosis: Primary Biliary Cholangitis (PBC).
Pathophysiology: Autoimmune destruction of intrahepatic/intralobular bile ducts.
Complication: Cholestasis -> malabsorption of lipids and fat-soluble vitamins (A, D, E, K), leading to deficiencies like Vitamin D deficiency (causing low bone mineral density).
Match the following vitamin deficiency symptoms to their correct water-soluble vitamin:
Peripheral neuropathy, sideroblastic anemia, glossitis
Scurvy (petechiae, perifollicular hemorrhage, poor wound healing)
Megaloblastic anemia without neurologic deficits
1) Vitamin B6 (pyridoxine)
2) Vitamin C (ascorbic acid)
3) Folic acid (Vitamin B9)

Patient taking ciprofloxacin for cystitis develops a thick, white vaginal discharge and pruritus -> Diagnosis and mechanism?
Diagnosis: Candida albicans vulvovaginitis
Mechanism: Antibiotic therapy wipes out normal bacterial vaginal flora (Lactobacillus) -> loss of colonization resistance allows opportunistic Candida overgrowth.
Key Features: Normal vaginal pH (less than 4.5), pseudohyphae and budding yeast on KOH prep.
Treatment: Oral fluconazole or topical azoles (clotrimazole, miconazole).
Match the classic vaginal discharge characteristics to the correct organism:
Green, frothy, malodorous discharge with cervical erythema (strawberry cervix)
Thin, watery or mucopurulent discharge with cervical motion tenderness
Painful vesicles that progress to shallow ulcers with an erythematous border
1) Trichomonas vaginalis (motile trichomonads on wet mount)
2) Chlamydia trachomatis or Neisseria gonorrhoeae
3) Herpes simplex virus (HSV-2)
Sinusitis/nasal ulcers + otitis media + lung granulomas/vasculitis + hematuria/proteinuria -> Diagnosis and targeted cell type?
Granulomatosis with Polyangiitis (GPA / Wegener)
Targeted Cell Type: Neutrophils (c-ANCA autoantibodies target proteinase 3 within neutrophil cytoplasm)
Classic Triad: Upper respiratory (sinuses/ears/nose) + Lower respiratory (lung nodules/hemoptysis) + Renal (rapidly progressive glomerulonephritis)
Why is targeting Endothelial cells incorrect for Granulomatosis with Polyangiitis (GPA)?
While GPA causes inflammation of the blood vessels (vasculitis), the autoantibodies (c-ANCA) directly target antigens inside neutrophils (specifically proteinase 3), not the endothelial cells lining the vessel walls.
Match the following cell types to their high-yield board functions/associations:
Basophils
Fibroblasts
Plasma cells
1) Basophils: Mediate allergic responses (similar to mast cells); bind IgE
2) Fibroblasts: Synthesize collagen and extracellular matrix; critical for wound healing and scar formation
3) Plasma cells: Terminally differentiated B cells that mass-produce immunoglobulins (antibodies)
Trichophyton Mentagrophytes
Dermatophyte that causes superficial infection of the skin
Scalp: Tinea Capitis
Trunk/Extremities: Tinea Corporis
Nail: Tinea Unguium
Groin: Tinea Cruris
Foot: Tinea Pedis
Loa Loa
Parasitic Worm passed to human from deerflies and is native to west and central africa
Itchy, Nonpainful swellings commonly involving the skin surrounding joints as well as eye lids
Malassezia Furfur
KOH preparation of a skin scraping is diagnostic and will show fungal spores and short hyphae along the edges of epidermal cells
Patient with acromegaly has persistent elevated IGF-1 levels despite radiation and octreotide therapy -> Next step medication mechanism of action?
Dopamine-2 (D2) receptor agonism (e.g., Cabergoline, Bromocriptine).
Why it works: D2 agonists can paradoxically decrease growth hormone (GH) secretion from a GH-secreting pituitary adenoma when somatostatin analogs (like octreotide) fail.
Why are inhibitors of 11-beta-hydroxylase and 17-alpha-hydroxylase wrong for treating persistent acromegaly?
11-beta-hydroxylase inhibition: Mechanism of metomidate/metyrapone; used to treat adrenocortical tumors/Cushing syndrome by blocking cortisol synthesis.
17-alpha-hydroxylase / 17,20 lyase inhibition: Mechanism of abiraterone; used to treat metastatic prostate cancer by decreasing androgen production.
Neither pathway regulates growth hormone or IGF-1.
Match the high-yield endocrine mechanism of action to its correct drug:
Inhibits thyroid peroxidase (TPO)
Serotonin (5-HT3) receptor antagonist
1) Propylthiouracil (PTU) or Methimazole (used for hyperthyroidism) 2) Ondansetron (strong antiemetic; has no endocrine function)
Large, painful, inflamed skin lump (carbuncle) -> What layer of skin is affected, and what is its embryologic precursor?`
Affected Layer: Dermis (a carbuncle is a cluster of infected hair follicles deep in the dermis, typically caused by Staphylococcus aureus).
Embryologic Precursor: Dermatome (the part of the somite that gives rise to the dermis, connective tissue, and blood vessels of the skin).
Match the somite/embryologic precursors to their correct adult structures:
Myotome
Sclerotome
Syndetome
1) Myotome: Gives rise to skeletal muscle.
2) Sclerotome: Gives rise to bone, vertebrae, and cartilage.
3) Syndetome: Gives rise to tendons.
Patient with progressive loss of peripheral vision, bitemporal hemianopia, and a pituitary mass -> What surgical approach is used, and which sinus must be traversed via the nose?
Surgical Approach: Transsphenoidal resection.
Sinus Traversed: Sphenoid sinus (the most posterior paranasal sinus, located directly inferior to the hypophyseal fossa/sella turcica).
Match the paranasal sinus to its high-yield surgical or anatomical border:
Bordered superiorly by the hypophyseal fossa
Bordered superiorly and posteriorly by the anterior cranial fossa
Bordered superiorly by the orbit and medially by the nasal cavity
1) Sphenoid sinus (pathway for transsphenoidal pituitary surgery)
2) Frontal sinus
3) Maxillary sinus
1 pound of body fat equals how many kilocalories (kcal)?
Approximately 3500 kcal.
Asthma patient given a leukotriene receptor antagonist (e.g., Montelukast) -> What type of receptor does this drug block?
Receptor Type: G protein-coupled receptor (GPCR).
Mechanism: Blocks CysLT1 receptors on bronchial smooth muscle -> prevents cysteinyl leukotriene (C4, D4, E4) binding -> decreases bronchoconstriction, airway edema, and inflammation.
Why is Protein kinase wrong for the mechanism of a leukotriene receptor antagonist?
Protein kinase receptors (like receptor tyrosine kinases) work via auto-phosphorylation and are typically utilized by growth factors and insulin, not leukotrienes.
Match the high-yield signaling receptor type to its classic board example:
Nuclear receptor
Ligand-gated ion channel
Voltage-gated ion channel
1) Nuclear receptor: Steroid hormones, thyroid hormone, Vitamin D (lipid-soluble ligands altering gene transcription).
2) Ligand-gated ion channel: Nicotinic ACh receptor (responds to chemical binding to allow ion flux).
3) Voltage-gated ion channel: Axonal sodium channels (responds to changes in membrane potential to propagate action potentials).

Photosensitive facial rash + proximal muscle weakness (climbing stairs/combing hair) + papules on dorsal hand joints -> Diagnosis and primary occult association?
Dermatomyositis.
Key Cutaneous Signs: Gottron papules (pink/purple papules on MCP and PIP joints), Heliotrope rash (periocular swelling/rash), and Shawl sign (poikiloderma on upper back/chest).
High-Yield Association: Occult malignancy/Cancer (especially internal adenocarcinomas like ovarian, lung, or gastric cancer as a paraneoplastic syndrome). Always requires age-appropriate cancer screening.
Key Autoantibodies: Anti-Jo-1 (associated with interstitial lung disease), Anti-Mi-2, and Anti-SRP.
Why is Renal failure / Systemic Lupus Erythematosus (SLE) incorrect for a patient presenting with Gottron papules and proximal muscle weakness?
SLE causes a malar rash that characteristically SPARES the nasolabial folds, and its hand rash affects the skin between the joints (interphalangeal spaces), whereas dermatomyositis directly involves the skin over the joints (Gottron papules). While SLE causes lupus nephritis leading to renal failure, it does not typically present with profound symmetric proximal muscle weakness.
Why do female participants achieve higher blood alcohol concentrations and increased intoxication compared with male participants receiving an equivalent dose of ethanol?
Primary Reason: Decreased gastric/hepatic alcohol dehydrogenase (ADH) activity (less first-pass metabolism of ethanol).
Secondary Reason: Relatively LOWER proportion of total body water in females -> lower volume of distribution -> higher blood alcohol concentration.
Why is a genetic polymorphism of Aldehyde Dehydrogenase (ALDH) incorrect for explaining elevated blood alcohol levels?
ALDH is a downstream enzyme that metabolizes acetaldehyde into acetate. A dysfunctional polymorphism here causes an accumulation of acetaldehyde (leading to vasodilation, flushing, and nausea), but it does NOT alter the upstream blood alcohol concentration.
ICU patient with severe acute illness (e.g., sepsis, pneumonia) + low total T3 and T4, but NORMAL TSH and normal free T4 -> Diagnosis?
Euthyroid sick syndrome (Nonthyroidal illness syndrome).
Pathophysiology: Critical illness and proinflammatory cytokines alter peripheral deiodinase activity -> decreased peripheral conversion of T4 to T3, and increased conversion of T4 to reverse T3 (rT3).
Clinical Note: Patients are clinically euthyroid. Treatment targets the underlying acute illness; thyroid supplementation is NOT indicated.
Why is Hypothyroidism or Antithyroid antibodies (Hashimoto) incorrect for an ICU patient with low T3/T4 and normal TSH/free T4?
Hypothyroidism / Hashimoto: Would present with an ELEVATED TSH (in primary disease) and clinical symptoms of low thyroid hormone (weight gain, cold intolerance, bradycardia).
A family history of Hashimoto is a distractor; normal TSH and free T4 in the setting of acute critical illness points directly to Euthyroid sick syndrome.
15-year-old girl with BMI 16, pulse 42, bradycardia, hypotension, cachexia, dry skin, laxative use, and intense fear of weight gain -> Underlying diagnosis and its core, most specific feature?
Diagnosis: Anorexia Nervosa (binge-eating/purging type).
Core Specific Feature: Intense fear of gaining weight (or behavior that interferes with weight gain) + distorted body image.
Key Distinction: Low body weight (BMI less than 18.5) is required for Anorexia. If BMI were normal or elevated with the same purging behaviors, it would be Bulimia Nervosa.
Why is a "sense of lack of control over eating" wrong as the most consistent/specific finding for Anorexia Nervosa?
While a loss of control can occur during binges in the binge-eating/purging subtype of Anorexia, it is a defining characteristic of Bulimia Nervosa and Binge Eating Disorder. An intense fear of gaining weight is more universal, core, and specific to Anorexia Nervosa.
Left foot clumsiness + left leg tingling + decreased fine touch, vibration, and proprioception in left lower extremity (normal strength and reflexes) -> Spinal cord lesion location?
Location: Dorsal funiculus on the left at T8.
Pathophysiology: Symptoms isolate to the Dorsal Column-Medial Lemniscus (DCML) tract, which carries fine touch, vibration, and proprioception.
Key Anatomy: DCML fibers travel IPSILATERALLY in the spinal cord and do not decussate until the medulla. Left-sided symptoms mean a left-sided spinal cord lesion.
Vertebral Level: A lesion at C2 would involve the upper extremities as well. A lesion isolated to the lower extremity must be in the lower thoracic or lumbar spine (e.g., T8).
Why are lesions of the anterolateral funiculus wrong for a patient with decreased vibration/proprioception and normal strength?
The anterolateral funiculus contains the spinothalamic tract (pain/temperature, which decussates 1-2 levels above entry) and parts of the corticospinal tract.
A lesion here would cause contralateral pain/temperature loss or ipsilateral weakness and altered reflexes, not a pure loss of vibration and proprioception.
5-year history of inability to conceive + bilateral soft lobulated masses + semen analysis shows sperm count of 0.8 million/mL + ultrasound shows increased scrotal temperature -> Diagnosis and underlying structure affected?
Diagnosis: Varicocele.
Structure Affected: Dilated veins of the pampiniform plexus.
Mechanism of Infertility: Increased venous pressure and blood pooling causes elevated scrotal temperature -> impairs temperature-sensitive spermatogenesis.
Key Exam Finding: Vermiform (bag of worms) feel on palpation; does NOT transilluminate.
Why is Obstruction of the ductus deferens incorrect for a patient with bilateral soft lobulated masses and increased scrotal temperature?
Ductus Deferens Obstruction: Secondary to scarring from STIs (e.g., Chlamydia, Gonorrhea) or Cystic Fibrosis. It causes azoospermia (zero sperm) or severe oligospermia, but it presents with normal or firm epididymides, normal testicular temperatures, and NO soft, lobulated scrotal masses.
Why do varicoceles occur much more commonly on the left side than the right side?
The left gonadal vein drains into the left renal vein at a 90-degree angle, causing higher hydrostatic resistance and pressure. The right gonadal vein drains directly into the low-pressure inferior vena cava (IVC) at an acute angle, making right-sided varicoceles rare (isolated right varicocele warrants evaluation for a retroperitoneal mass).
Patient falls from a ladder and presents with multiple ecchymoses -> Activation of the vascular endothelium most directly increases the concentration of what factor?
* Factor: von Willebrand factor (VWF).
Mechanism: Endothelial damage triggers the immediate release of VWF from endothelial cells (Weibel-Palade bodies) and platelet alpha-granules. VWF binds to exposed subendothelial collagen and tethers platelets via the Gp1b receptor to initiate primary hemostasis.
Premature newborn (30 weeks) + maternal type 1 diabetes + respiratory distress (grunting, retractions) + chest X-ray showing uniform reticulogranular densities -> Diagnosis and direct cause of hypoxemia?
Diagnosis: Neonatal Respiratory Distress Syndrome (NRDS).
Direct Cause of Hypoxemia: Atelectasis (alveolar collapse).
Pathophysiology: Insufficient surfactant production by type 2 pneumocytes -> increased alveolar surface tension -> widespread alveolar collapse (atelectasis), which prevents proper gas exchange.
Maternal Diabetes Risk Factor: High fetal insulin levels (due to maternal hyperglycemia) inhibit cortisol, delaying surfactant synthesis.
Type 1 pneumocytes
Thin cells responsible for gas exchange, not surfactant production. Their hyperplasia is rare and does not cause the diffuse alveolar collapse and decreased compliance characteristic of NRDS.
Neonatal pneumonia
While it causes respiratory distress, it would typically present with a localized lobar consolidation on X-ray, fever, and positive blood or sputum cultures, all of which are absent in this patient.
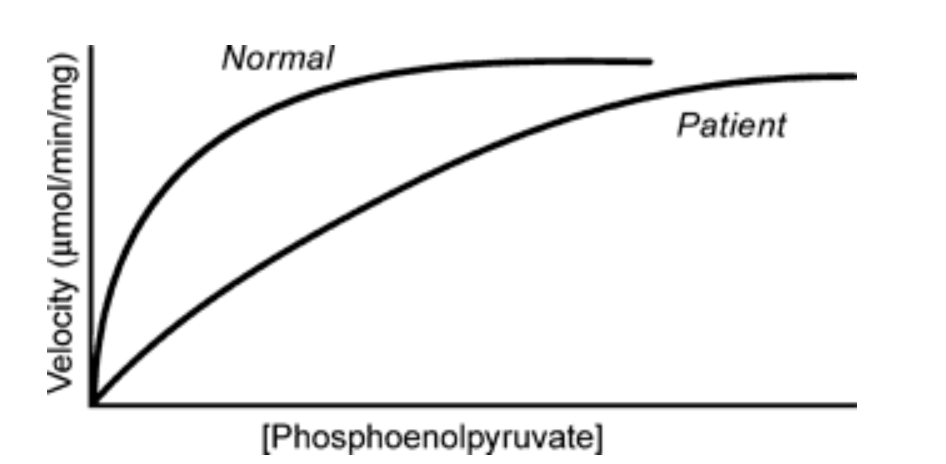
Patient with hemolytic anemia has a pyruvate kinase (PK) enzyme curve that shifts to the right but reaches the same max velocity -> What is the kinetic mutation?
Mutation: Increased Km (Michaelis constant), which means decreased substrate affinity.
Graphical Proof: The patient curve is shifted right, meaning a HIGHER concentration of phosphoenolpyruvate (PEP) is required to reach half-Vmax. The peak height (Vmax) remains identical to normal.
RBC Impact: Defective PK -> decreased ATP production -> RBCs lack energy to maintain ion pumps -> cellular swelling, lysis, and chronic hemolytic anemia.
Why are a decrease in enzyme synthesis, an increase in degradation, or a mutation decreasing Vmax wrong for this curve?
All of those scenarios would lower the total amount of functional enzyme, which mathematically decreases Vmax (lowers the curve peak). Because the patient's curve eventually reaches the exact same plateau height as the normal curve, Vmax is unchanged.
Match the regulators of Pyruvate Kinase to their high-yield effects:
Fructose-1,6-bisphosphate
ATP and Alanine
1) Fructose-1,6-bisphosphate: Strongly upregulates PK (feed-forward activation).
2) ATP and Alanine: Strongly downregulate PK (signaling high cellular energy/building blocks).
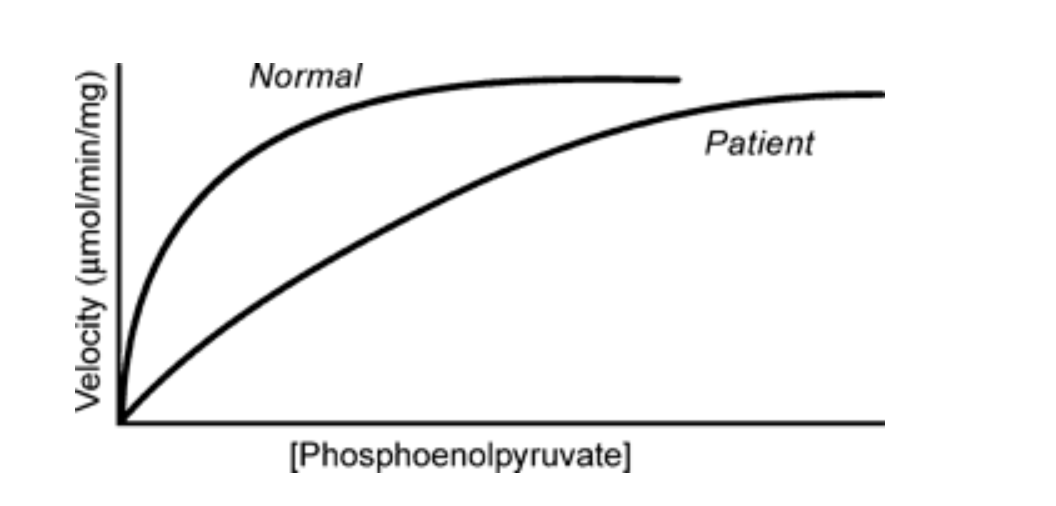
Why is the presence of a noncompetitive inhibitor wrong for this enzyme curve?
Noncompetitive inhibitors bind to an allosteric site and decrease Vmax while keeping Km unchanged. This curve shows an increased Km with an unchanged Vmax, which describes a competitive inhibitor mechanism or an affinity-altering mutation.
Pregnant woman at 36 weeks with BP 160/100, proteinuria, thrombocytopenia, and elevated creatinine -> Diagnosis and classic placental histology?
Diagnosis: Preeclampsia with severe features
Placental Histology: Acute atherosis of decidual vessels (fibrinoid necrosis of spiral arteries with lipid-laden macrophages and inflammatory cells)
Pathophysiology: Abnormal remodeling of maternal spiral arteries by cytotrophoblasts -> placental ischemia -> release of antiangiogenic factors -> widespread maternal endothelial dysfunction
Match the high-yield placental pathology to its classic board presentation:
Acute chorioamnionitis
Chronic villitis
Placenta accreta
1) Acute chorioamnionitis: Maternal fever, leukocytosis, uterine tenderness; caused by ascending bacterial infection
2) Chronic villitis: Maternal inflammatory cells invading chorionic villi; associated with TORCH infections or immune-mediated graft-vs-host response
3) Placenta accreta: Severe postpartum hemorrhage and inability to detach placenta; villi attach directly to or invade the myometrium due to a defective decidual layer
62-year-old man + pancytopenia + massive splenomegaly + lymphocytes with cytoplasmic projections and tartrate-resistant acid phosphatase (TRAP) positivity -> Diagnosis, key driver mutation, and first-line treatment?
Diagnosis: Hairy cell leukemia (HCL)
Driver Mutation: V600E somatic mutation in the BRAF gene (leads to constitutive BRAF signaling and cell survival)
First-line Treatment: Cladribine (a purine analog that resists degradation by adenosine deaminase)
Key Exam Clue: Causes a "dry tap" on bone marrow aspiration due to extensive marrow fibrosis; lacks lymphadenopathy (unlike CLL).
Why is Chronic Lymphocytic Leukemia (CLL) the wrong diagnosis for a patient with TRAP-positive lymphocytes containing cytoplasmic projections?
CLL classically presents with striking leukocytosis (lymphocytosis), whereas HCL characteristically causes pancytopenia.
On a peripheral smear, CLL shows fragile "smudge cells" (ruptured lymphocytes) rather than cells with hair-like cytoplasmic projections. CLL is also highly associated with generalized lymphadenopathy, which is typically absent in HCL.
Match the leukemia/lymphoma to its classic high-yield peripheral blood smear finding:
Hairy cell leukemia
Chronic lymphocytic leukemia (CLL)
Acute myelogenous leukemia (AML)
1) Hairy cell leukemia: Differentiated B cells with thin, hair-like circumferential cytoplasmic projections.
2) CLL: Small, mature-looking lymphocytes with smudge cells (crushed/ruptured cells).
3) AML: Myeloblasts with pink/red rod-like cytoplasmic inclusions (Auer rods formed by fused azurophilic granules).
Son has ADPKD with elevated creatinine, but father has ADPKD with normal creatinine -> What genetic mechanism explains this difference in disease severity?
Mechanism: Variable expression (variable expressivity).
Definition: Patients with the exact same genetic mutation show a spectrum of different phenotypic severities or clinical features.
Key Distinction: ADPKD has complete penetrance (everyone with the mutation gets cysts), but variable expression determines how bad the disease gets or how fast renal function declines.
Why is Decreased penetrance the wrong genetic mechanism for an ADPKD family where some members have normal renal function?
Penetrance is an all-or-nothing concept (does the patient show signs of the disease or not?).
Because the father has cystic kidneys on ultrasound, he completely penetrates the disease phenotype. The fact that his creatinine is normal while his son's is high is a variation in severity (expression), not penetrance.
Match the high-yield genetic terms to their classic definitions:
Pleiotropy
Anticipation
Heteroplasmy
Pleiotropy: One single gene mutation causes multiple, seemingly unrelated phenotypic traits (e.g., PKU causing fair skin and intellectual disability).
2) Anticipation: Disease severity increases or presents at an earlier age with each subsequent generation (classic in trinucleotide repeat disorders like Huntington).
3) Heteroplasmy: Presence of both mutated and normal mitochondrial DNA within a single cell, dictating the severity of mitochondrial inherited diseases.
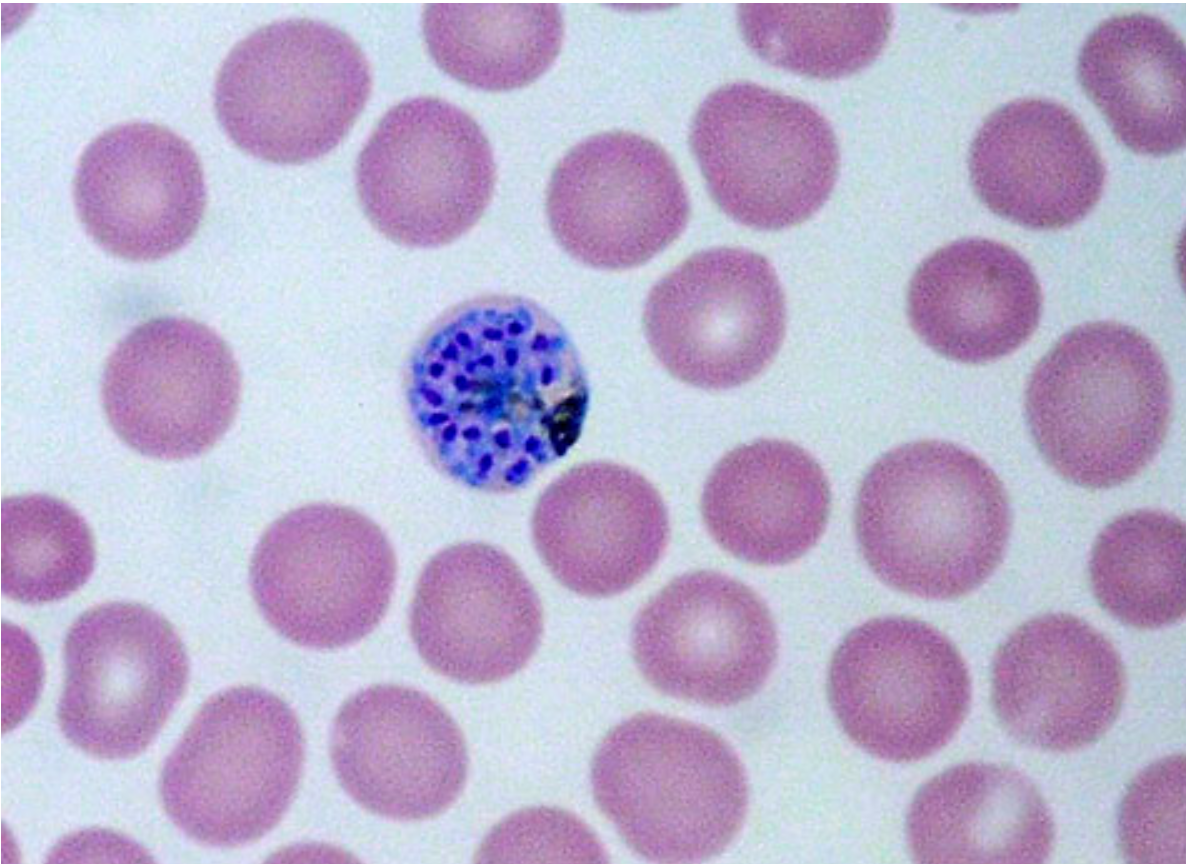
Patient with cyclic fever/chills after travel to Mexico + blood smear showing intraerythrocytic ring forms/schizonts -> Vector and causal genus?
Vector: Female Anopheles mosquito
Causal Genus: Plasmodium (Malaria)
High-Yield Management: Southern Mexico travel points toward Plasmodium vivax. Must add Primaquine to Chloroquine regimen to eradicate latent hypnozoites in the liver and prevent relapse. G6PD deficiency screening is mandatory before starting Primaquine to avoid severe hemolytic anemia.
Why is Sandfly incorrect for a patient with cyclic fevers and intraerythrocytic inclusions?
Sandflies transmit Leishmania protozoa.
Visceral leishmaniasis (Kala-azar) causes spiking fevers, hepatosplenomegaly, and pancytopenia.
Amastigotes would be found inside macrophages (Leishman-Donovan bodies), not inside red blood cells.
Match the vector to its classic board-tested disease and pathogen:
Kissing bug (Reduviid bug)
Tsetse fly
Body louse
1) Kissing bug: Chagas disease (Trypanosoma cruzi); causes dilated cardiomyopathy, megacolon, megaesophagus.
2) Tsetse fly: African sleeping sickness (Trypanosoma brucei); causes painful bite, lymphadenopathy, and CNS reversal of sleep-wake cycle.
3) Body louse: Epidemic typhus (Rickettsia prowazekii); causes rash spreading outward from trunk, sparing palms/soles.
Crohn disease patient on a monoclonal antibody develops fever, night sweats, weight loss, and a right apical cavitary lung lesion -> Targeted cytokine and primary function disrupted?
Target: Tumor necrosis factor-alpha (TNF-alpha)
Medications: Infliximab, adalimumab, certolizumab
Disrupted Function: Granuloma formation and maintenance. Blocking TNF-alpha causes existing granulomas to sequestering Mycobacterium tuberculosis to break down, leading to reactivated latent TB.