random tidbits from readings--msk
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
most common form of juvenile idiopathic arthritis
asymmetric oligoarticular
difference between polyarticular and oligoarticular arthritis?
polyarticular involve 5 or more joints
oligoarticular involves 4 or fewer joints
with a PCL sprain what exercise would be MOST INAPPRORIATE to perform?
hamstring exercise
Achilles tendonitis is seen in patients with the following EXCEPT
foot supination
all of the following are appropriate s/s someone may have a RTC tear, EXECPT which of the following?
pain over lateral epicondyle of humerus
what nerve is affected with ape hand deformity
median n.
describe ape hand deformity
wasting of thenar eminence
thumb falls back in line with fingers
bc of extensor muscs
pt unable to flex or oppose thumb
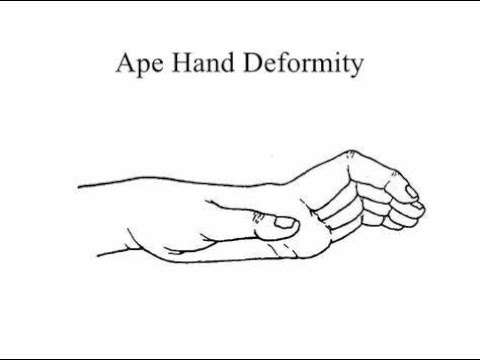
ape hand deformity
bishop’s hand or benediction affects what nerve
primarily high median n.(at level of elbow or forearm) or could be ulnar nerve
common cause is fracture from FOOSH at distal humerus
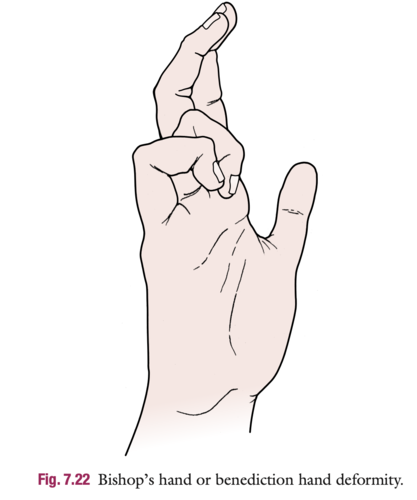
hand of benediction or bishop’s hand deformity
describe bishop’s hand or benediction
hyperextension of MCP joint
flexion of IP joint
seen when trying to make a fist (inability to flex index or middle finger)
(if ulnar nerve involvement: wasting of hypothenar muscles, interossei, and 2 medial lumbrials)
describe the meniscus vascular zones
outer third (red zone)
good blood supply and heals well
middle third (red-white zone)
limited blood supply
inner third (white zone)
avascular, heals poorly
McMurray’s test: what forces applied to test MEDIAL meniscus?
valgus stress + ER
as you extend the knee
McMurray’s test: what forces applied to test LATERAL meniscus?
varus stress + IR
as you extend the knee
what is the “golden rule of collateral testing”
at 30 deg of knee flexion, the posterior capsule is slack
thus isolating the collateral ligament
at 0 degs (full knee extension), you are stressing the collateral ligaments PLUS the capsule PLUS possibly the cruciate ligaments
(if you find more laxity at 0 deg,,, think MULTI-ligamentous or capsular involvement)
squinting patella (inward facing kneecaps) results from:
femoral anteversion
foot pronation
VMO weakness
tight medial retinaculum
frog-eyed patella (patella outward facing) results from:
femoral retroversion
patella alta (high kneecaps)
genu varum
PFPS is characterized by
anterior/retropatellar pain
pain aggravated by deep knee flexion
squats, stairs, prolonged sitting (movie goer’s sign)
think females and athletes
precautions for ACL
knees must never move past toes in squats
avoid quadriceps strengthening between 60-90 deg of flexion
aka no deep squats
avoid knee extension 45-30 in OKC for first 6-12 weeks
MOI for ACL
Planted foot + tibial ER + hypertension
What is the terrible triad?
Injury to MCL, ACL, and medial meniscus
(Knee collapses into valgus with rotation while foot is planted)
LAPS protocol for ACL
L- Lachmens Test
A-anteriorl drawer test
P- pivot shift
S-slocums test
Grade 1 ligament tear
Minimal pain
Minimal laxity
Grade 2 ligament tear
Moderate to severe pain
Moderate laxity
Grade 3 ligament tear
Little to no pain
High laxity
Which meniscus attaches to MCL making it more prone to injury?
Medial meniscus
MOI of meniscus
Compression
Rotation
Flexion
(Twisting on a loaded, bent knee)
Pain with compression + rotation during Apley’s may indicate what injury
Meniscus injury
Pain with distraction + rotation may indicate what
Ligament injury
Clarke’s sign tests for what
PFPS
What is Clarke’s sign?
Apply downward pressure on superior patella
Ask pt to contract quad
(+): retropatellar pain or crepitus
McConnell’s Test purpose
PFPS
McConnell’s test
isometric resisted knee extension at different angles
Whenever discover pain= repeat contraction but add medial patellar mobilization
If relieved pain with this then can provide taping and test is POSITIVE
For PFPS what OKC AND CKC angle to avoid
OKC: avoid last 30° of extension
CKC: limit 60-90° of flexion
Where is point tenderness for jumpers knee (patellar tendinitis)
Inferior pole of the patella
What limitations are often seen in people with Jumper’s knee (patellar tendinitis)
Decreased ankle DF
Decreased quad flexibility
What type of exercise has strong evidence for tendon healing
Isometric exercises
IT band friction syndrome symptoms
Sharp lateral knee pain at 30° flexion
-pain with repetitive motion (cycling) or climbing/descending stairs
Noble compression test purpose
Assess friction syndrome for IT band
Noble Compression test
apply pressure over the lateral femoral epicondyle
Extend knee from 90° of flexion
(+) pain around 30° of flexion
Osteochondritis dissects (ocd) involves what and affects who
involved subchondral bone
Can separate and become necrotic
Affects 10-20 y/o
bones are developing and growing
Wilsons’s test
For OSTEOCHONDRITIS DISSECANS
pt extend knee against resistance from 90° while keeping tibia IR
if pain around 30°, have pt ER foot
(+): if pain relieved when ER at 30° flexion
Hughstons plica test
Moving knee through flexion and extension while applying IR to tibia and medial glide to patella
(+): popping of plica band
Following TKA, ambulation without an AD is only recommended once:
Full knee extension is achieved
Adequate strength of quads and hip are present
Why have hinged brace at 0° for PCL injury
Gravity will cause tibia to sag posteriorly
How long to maintain all postural drainage positions
5-10 min
What are the most common fractures seen in ppl with severe osteoporosis
Vertebral compression fx
Colles wrist fx
Hip fx
Severe osteoporosis criteria
T-score below -2.5
Presence of one or more fragility fractures
Small (<= 1 cm) RTC tear requires how long immobilized
1-2 was in sling
(Can remove for exercise POD1)
Medium to large (1-5 cm) RTC tear requires how long immobilized
Sling/abduction orthotics for 3-6 weeks
(Remove for exercise POD1-2)
Massive (> 5cm) RTC tear requires how long immobilized
Sling/abduction orthotics for 4-8 weeks
Remove for exercise POD1-3
claw fingers (aka intrinsic MINUS) hand involve what nerve
ulnar n. (can also affect median n.)

(ulnar) claw hand
claw hand characteristics
hyperextension at MCP
flexion at IP
loss of ABD/ADD in all 4 fingers
(loss of intrinsic muscle and overaction of extensors)
drop-wrist deformity affects what nerve
radial n.
(often from humeral shaft fx or compression at axilla)

wrist drop deformity (saturday night’s palsy)
wrist drop deformity characteristics
inability to extend the wrist

dupuytren's contracture
dupuytren's contracture characteristics
contracture of palmar fascia
fixed flexion of MCP and PIP
usually in ring or pinky
men>women

mallet finger
mallet finger characteristics
distal phalanx in flexion at rest
mallet finger caused by rupture or avulsion of
extensor tendon at distal phalanx
boutonniere deformity
boutonniere deformity characteristics
extension of MCP and DIP
flexion of PIP
boutonniere deformity is the result of a rupture of the __________
central tendinous slip of the extensor hood
boutonniere deformity most common after
trauma or in RA

swan neck deformity
swan neck deformity characteristics
extension of PIP
flexion of MCP and DIP
swan neck deformity due to contracture of what
intrinsic ma or tearing of Volar plate
(common in RA)
trigger finger (aka tenovaginitis stenosans) usually occurs
in 3rd or 4th finger
trigger finger (aka tenovaginitis stenosans) is the result of
-thickening of flexor tendon sheath (Notta’s nodule)
(sticking of tendon when pt attempts to flex finger—when finger “let’s go” a snap occurs)
-low inflammation of proximal flexor tendon
trigger finger (aka tenovaginitis stenosans) most often associated with
RA and is worse in the morning

trigger finger
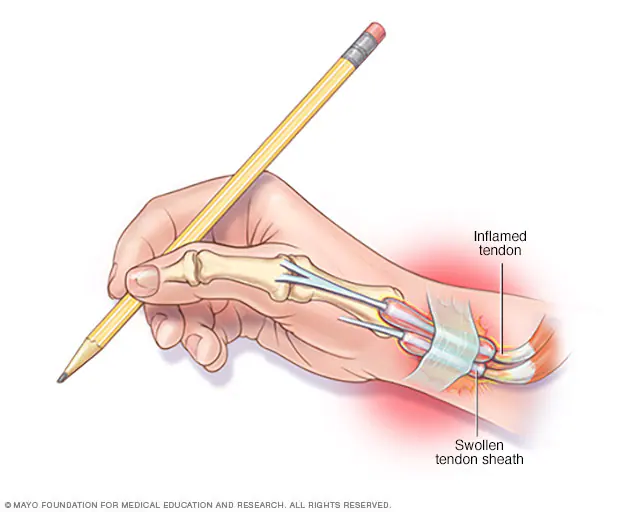
de quervain’s tenosynovitis
de quervain’s tenosynovitis is the inflammation of
the extensor pollicis brevis (EPB)
and
abductor pollicis longus (APL)
(at 1st dorsal compartment)
de quervain’s tenosynovitis commonly seen during
pregnancy
de quervain’s tenosynovitis positive for
pain at anatomical snuffbox
swelling
decreased grip and pinch strength
(+) Finkelstein’s test
carpal tunnel syndrome is the compression of
median n.
common in pregnancy, DM, RA
positive Tinel’s sign
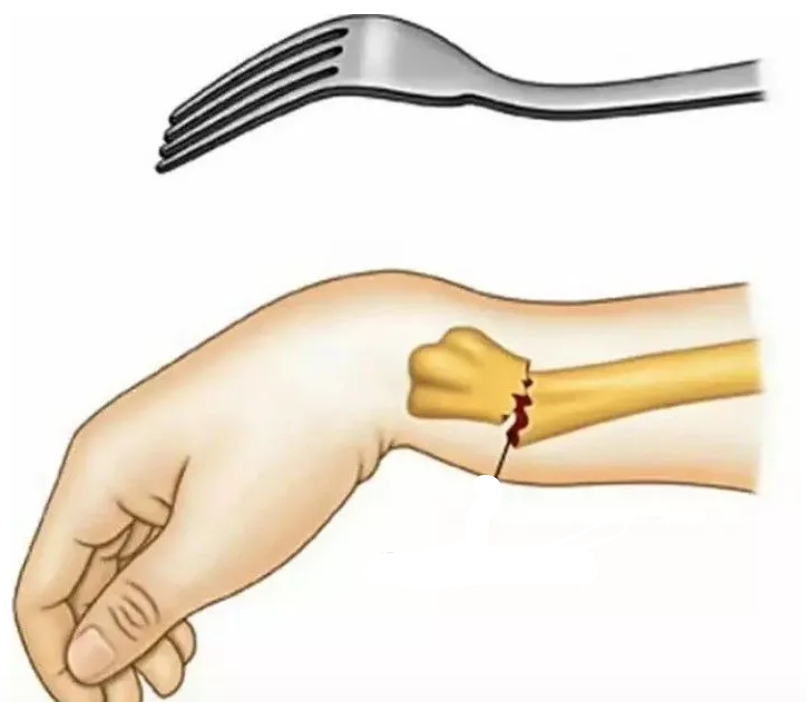
colles fracture
colles fracture: ______displacement of the distal fragment of the radius
dorsal
smiths fracture: ____displacement of the distal fragment of the radius
volar
what is a chronic degenerative condition of the ECRB ; characterized by painful passive wrist FLEXION and active wrist EXTENSION
lateral epicondylitis (tennis elbow)
lateral epicondylitis special tests
cozen’s test
mill’s test
maudsley’s test
what is the degenerative condition of the pronator teres and flexor carpi radialis ; characterized by painful passive wrist extension and active wrist flexion?
medial epicondylitis (golfer’s elbow)
describe supracondylar fracture
fracture at distal humerus
common in kids (FOOSH)
AIN (from median n.) and brachial artery at risk
requires ORIF
complications of supracondylar fracture
Volkmann’s ischemic contracture
gun stock deformity (cubital varus)
MALUNION!
describe nursemaid’s elbow (pulled elbow)
usu 2-3 y/o
how?
longitudinal traction on extended elbow
slippage of annular ligament over head of radius
radial n. can be injured
position of arm with nursemaid’s elbow after slippage
arm at side with hand pronated
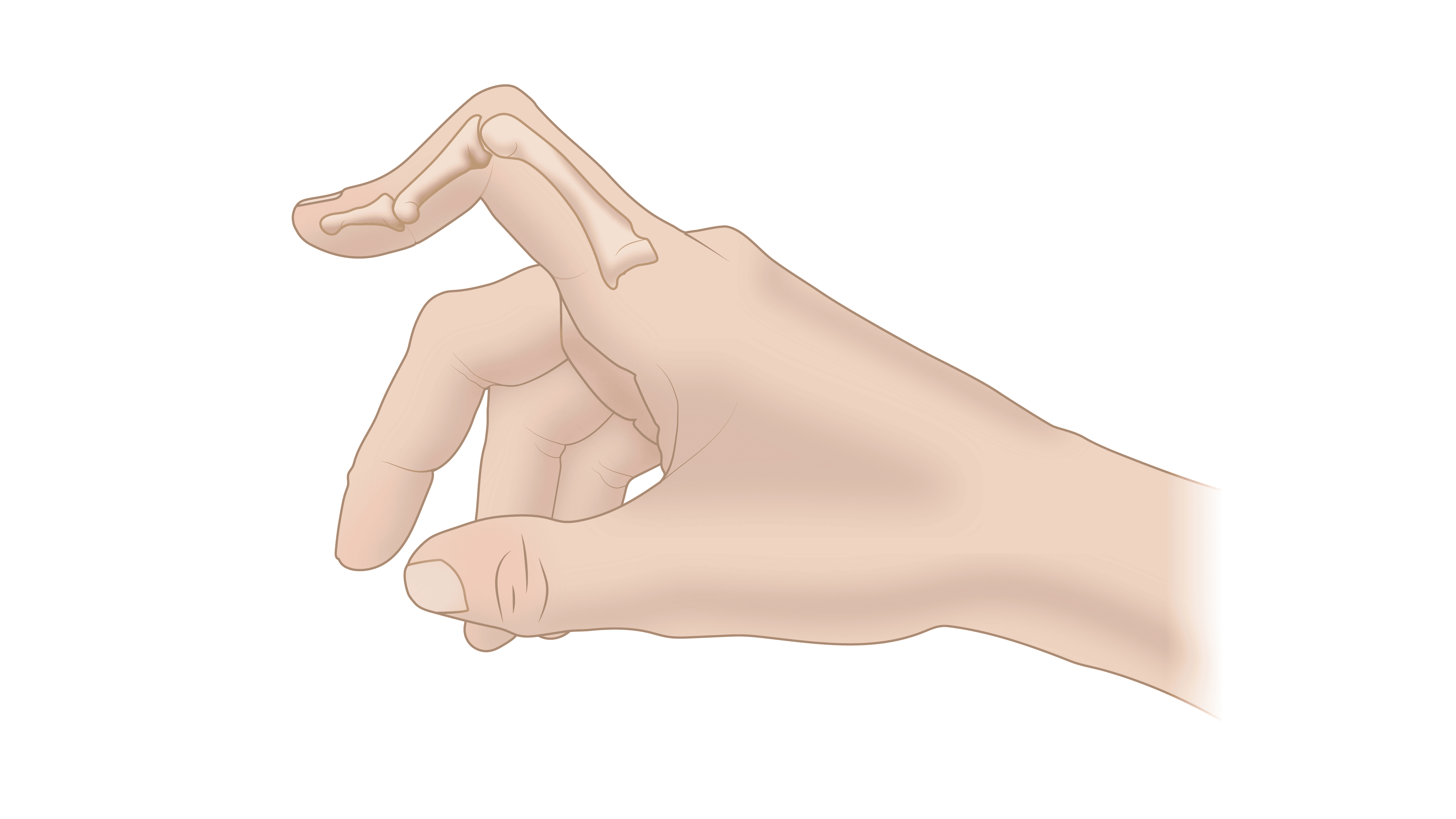
AIN (anterior interosseous nerve) syndrome
weakness of FPL and FDP (index finger)
weakness of pronator quadratus
(see weird “OK” sign)
biceps tendon rupture (distal)
swelling and ecchymosis (bruising)
palpable gap in biceps tendon
WEAK elbow flex and supination
myositis ossificans
bone forms inside of muscle
(common in brachialis from trauma or aggressive stretching)
avoid stretching, massage, resistive exercises, heat
brachialis strain
pain on ANTERIOR distal part of arm
painful resisted elbow flexion with forearm PRONATED
thoracic outlet primary sites for compression or entrapment
interscalene triangle
brachial plexus in between anterior and middle scalene
stretch scalene
costcoclavicular space
between the clavicle and first rib
mobilize 1st rib
axillary interval
between pec minor and coracoid process
stretch pec minor
arterial s/s of TOS
cool and pale extremity
venous s/s of TOS
swelling
mottled discoloration
neurological s/s of TOS
numbness
tingling
weak grip
loss of intrinsics/dexterity