Ch 3 Prenatal Development and Birth
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
what does prenatal development begin and end with
begins at conception (process of fertilization of egg by a sperm and ends with birth
how long does development take
38 to 40 weeks (~9 months)
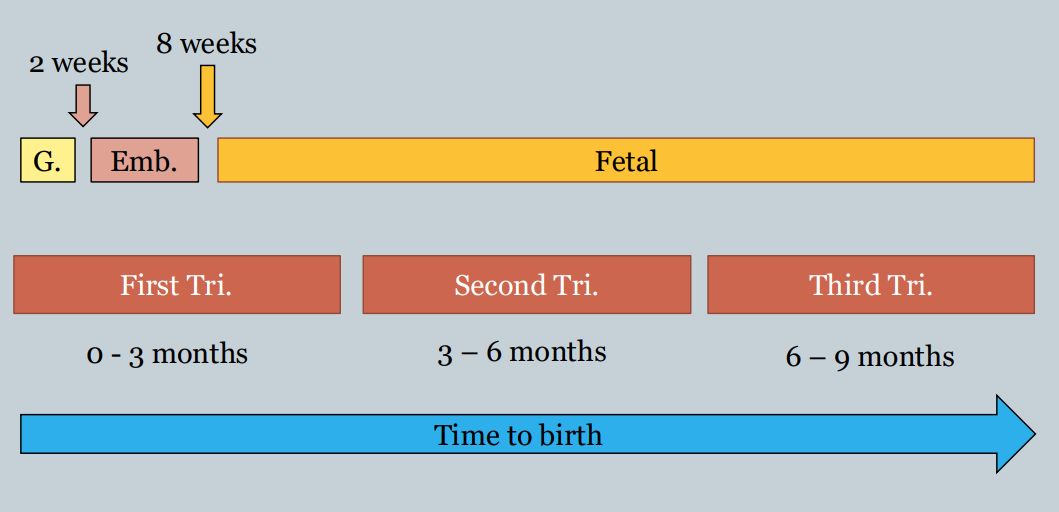
three periods
germinal (0-2 weeks)
embryonic (2-8 weeks)
fetal (8 weeks - birth)
germinal period(0-2 weeks)
creation of fertilized egg = zygote
beginning of cell division and differentiation starts to take place
as cell division continues, the mass of cells that will eventually develop into the embryo (called the blastocyst)
blastocyst is surrounded by the trophoblast, outer layer of cells that will later provide nutrition and support for the embryo
attachment of zygote to the uterine wall
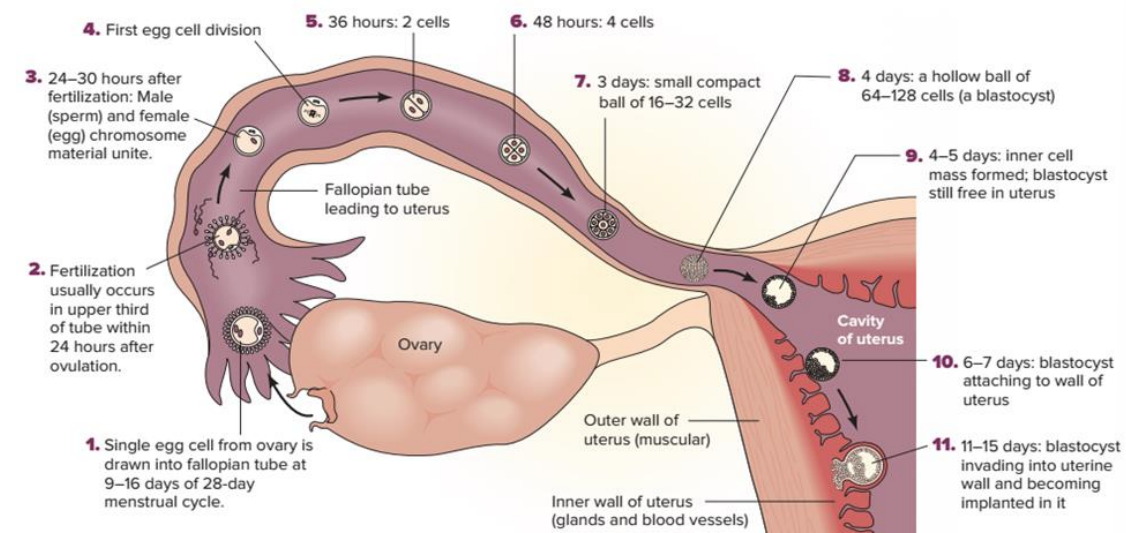
embryonic period (2-8 weeks)
begins once blastocyst attaches to uterine wall (called embryo)
cell differentiation further into bodily systems
life support system for cells start of form (ex. placenta, umbilical cord)
organs first start to form (organogenesis)
organs appearing in the embryonic period
day 21: eyes begin to appear
day 24: heart starts to form clearly
week 4: arm and leg buds emerge, blood vessels appear
weeks 5 to 8: arm and legs further develop, face starts to form
just over an inch long by the end of the embryonic period
fetal period (8 weeks - birth)
referred to as a fetus
facial features and limbs become more easily distinguished
arms, legs, head move spontaneously
sex can be identified in most cases (~3 months)
mother can start to feel movement (~5 months)
around 6 months, fetus has some chance of survival outside of the womb (considered viable)
lungs not fully mature
continues growing through 9 months)
born at average 8lbs and 20 inches long (in the US)
the three trimesters
prenatal development period is divided into 3 equal-length parts
not the same as prenatal periods
fetal period begins towards the end of the first trimester
viability begins at the end of the second trimester
teratogen
any agent w/ potential to negatively affect development during prenatal period
physical birth defects
altered brain formation
influence cognitive or behavioral functioning
may not immediately apparent at birth
influence of teratogens vary by:
dose: greater the dog (such as the drug), greater the effect
genetic susceptibility: some people may be more vulnerable to particular teratogen based on their genetics
timing of exposure
timing of teratogen exposure continued
can be more vulnerable at different points of development
germinal period > may prevent implantation into uterine wall
embryonic period > structural defects in various organs
fetal period > how well organs function, stunted growth
embryonic period generally most vulnerable period
organogenesis/ risk of structural defects of organs at its greatest
examples of teratogens: prescriptions/ nonprescription drugs
antibiotics
certain antidepressants
certain hormones supplements
diet pills
high doses of aspirin
psychoactive drugs
drugs which act on the nervous system to alter states of consciousness, modify perception, or change mood)
caffeine
alcohol
nicotine
cocaine
marijuana
heroin
caffeine
common in many people’s diet
mixed results on extent of effects
some data to suggest related to lower birth among babies
US FDA recommends pregnant women avoid or consume sparingly
nicotine
smoking effects prenatal development, birth complications, and postnatal development
lower birth (implicated in as many as 25% of infants born with low birth weight
fetal death, respiratory problems in baby (and later as adolescent)
risk factor for development of ADHD
not limited to just tobacco cigarettes (e-cigarettes also contain nicotine)
23% of adolescent and 15% of adult pregnant women report having smoked in past month
cocaine
quickly crosses placenta to reach fetus to harm development
low birthweight, neurological/cognitive impairments
impaired motor development, slowed rate of growth, learning disabilities, externalizing behavior problems
marijuana
low birth weight
alter brain development (lower intelligence in children)
heroin
child themselves exhibit withdrawal symptoms (ex. tremors, irritability, abnormal crying, disturbed sleep, impaired motor control)
continued behavior problems during childhood
attention deficits
alcohol
fetal alcohol syndrome (FAS) brought on my alcohol use during pregnancy resulting in facial abnormalities, deformities, heart defects, intellectual disabilities, and learning problems
general recommendation: no amount of alcohol is safe
maternal diseases and infections can also cause damage during birth
genital herpes (if passed through birth canal)
HIV/AIDS (although may be born not infected at all)
variety of other infectious disease
maternal diet and nutrition
embryo or fetus depends completely on mother for nutrition
malnutrition in mother:
developing embyro/fetus needs those nutrients to develop properly
children born to malnourished mothers more likely to be born malformed
obesity in mother:
increased risk of hypertension (high blood pressure), diabetes, respiratory problems, complications during pregnancy or birth
adolescent mothers
mortality rate for children double that of mothers in their 20s
may be tied to SES or decision making?
least likely age group to obtain proper prenatal care from clinics
women 35 years and older
increased risk of some disorder (ex. down syndrome)
tied to increased risk of mother’s eggs possessing genetic anomaly that disrupts typical prenatal development
risk increases for low birth weight preterm delivery, fetal death
risk rises over time
emotional states and stress
mother’s emotional states may influence fetus as well
altering mother’s physiology
influencing mother’s behavior
chronic anxiety/stress
increased blood pressure, stress hormones
cognitive problems, emotional problems, ADHD, language delays
harmful coping methods
mother may be more llkely to engage in harmful behaviors to cope
ex. substance use/teratogens
paternal factors
exposure to lead, radiation, certain pesticides
may cause abnormalities in sperm
may lead to miscarriage or certain diseases in child
smoking in fathers
exposure to chemical that may lead to abnormalities in sperm
second-hand exposure for mother/fetus
age of father:
risk of fetus seem to increase as fathers’ age reaches 40+
rates of autism, schizophrenic disorders
relationship with mother
supportive or conflictual?
prenatal care
scheduling several visits for regular medical checkup
screen for manageable conditions/treatable diseases
educational services for parents-to-be:
nutrition information
benefits of low-level exercise
provide information about pregnancy/process of childbirth
childbirth
in the us, 98% of childbirths take place in hospital
range of options for method of delivery, most of which are hotly debated
medication to reduce pain in childbirth
birthing process often involves great pain to mother
concern about higher dosages and possible negative effect on the fetus
may reduce mother’s ability to push fetus out (ex. sedation, numbness)
individual differences in sensitivity to certain meds (mother and child)
tricky to make decisions (as both the parents and medical care provider)
natural childbirth and pain reduction
push for non-medication based ways to reduce pain during birth
breathing techniques, relaxation techniques, husband or other trusted individual as coach during birth to help promote relaxation
Cesarean delivery
medical procedure where baby is surgically removed from mother’s uterus by incision in her abdomen
generally not recommended as the default (~32% of births in US)
performed when complications arise during birthing process
ex. mother unable to push, baby’s head too large, baby in breech position
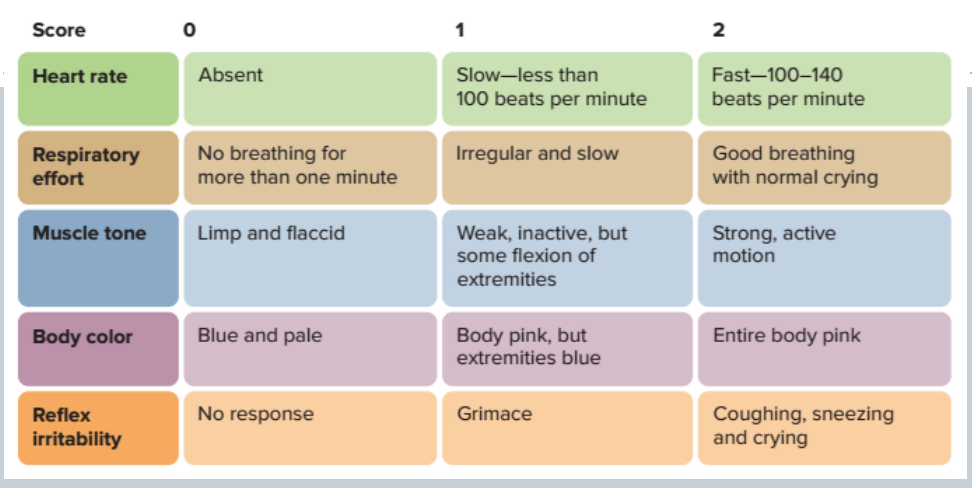
assessing newborn
apgar scale: widely used tool used to assess health of newborn babies at one and five minutes after birth
assessment of: heart rate, respiration, muscle, body color, reflex irritability
depending on infant’s score, condition classified as either good, signs of developmental difficulties, or emergency situation
Apgar scale
5 categories
higher the score, the better
the total score is then summed up across all 5 categories to assess overall status of the newborn
infant size and health
low birht weight (,5 pounds, 8 oz)
very low birth weight infants (<3 pounds, 4 oz)
extremely low birth weight infants (<2 pounds)
preterm infants: born three weeks or more before expected full-term pregnancy ( prior to 37 weeks gestation)
small for date infants have birth weight below normal, considering how far along pregnancy is compared to other babies at same gestational age
ex. baby weighs less than 90% of all other babies at same gestational age
risk factors: nutrition, substance use, stress, maternal age, low access to prenatal care, low SES/ poverty
lower birth weight/earlier the preterm delivery > higher risks
viability
developmental disorders
important statistics
human have been giving birth a long time
risks to pregnancy are generally very low for healthy adults
majority babies are born at full-term, healthy, and happy
97% of babies are born in the US without any kind of major defect
many defects (webbed toes, some heart defects) are treatable
postpartum period
the period after childbirth/delivery that lasts for about six weeks (or until mother’s body has returned to nearly pre-pregnant state)
requires some physical, emotional, and psychological adjustments for parents
focus has generally been on mother, but more research and acknowledgement being given to experience of father in recent times
postpartum period: physical adjustments
lack of energy/exhuastion/fatigue
loss of sleep
can lead to increased stress, conflict with partner
undermine confidence in own ability to adjust to life with baby
postpartum period: emotional/psychological adjustments
“postpartum blues” (“baby blues”) are common feelings of sadness parents may feel two to three days following birth of their child
reported by ~70% of new mothers
may come and go
generally resolves on its own w/o intervention in one or two weeks
postpartum depression
involves a major depressive episode following birth/delivery of a child
feelings of sadness, anxiety, or despair lasting a period of at least two weeks that are severe enough to impair daily functioning
experienced by ~10-14% of new mothers
typically occurs about four weeks after birth/delivery
can last for several months without treatment
risk factors for postpartum depression
History of clinical depression
Depression or anxiety during pregnancy
Neuroticism (trait disposition to experience negative affects)
Low self-esteem
Postpartum blues
Having a poor marital relationship
Low levels of social support
exercise and treatments may aid
postpartum period with faterh
fathers also undergo adjustment during the postpartum period
may also experience depression
~5% report symptoms of depression in first two weeks following delivery
increased odds if mother also develops postpartum depression
feelings of neglect in the relationship/ mother always prioritizes baby over father
depression in both parents can impair the bonding process with their child during postpartum period
early bonding
time period shortly following birth can be a special time of bonding between parents and newborn (emotional and physical)
concern among that there is a critical period for bonding in first few days following birth of baby, where newborn must have close contact with mother to develop optimally
research suggests skin contact with parent during first days of life is not critical, however, hospitals should strive to allow parents to interact with their newborns as much as possible
kangaroo care
kangaroo care
skin-to-skin contact between baby and parent, where baby is held upright against the parent’s bare chest
takes 2-3 hours per day
becomes more commonplace in the US hospital system
benefits:
helps stabilize infants heartbeat, temperature, breathing
healthy weight gain in preterm infants
decreased risk of mortality in low-birth-weight infants