BILD 2 Midterm 4
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
How is pressure involved in the movement of water & nutrients in plant xylem & phloem?
Xylem
Water moves from roots → leaves
No pumps in the roots
Transpiration at the leaves lowers pressure, so water evaporates through stomata
Very low pressure in the leaves causes water to be pulled upward from higher pressure in the roots
Movement occurs because of a pressure gradient created by evaporation at the top
Phloem
Sugar is actively loaded into phloem at source cells in the leaves
High sugar concentration draws in water by osmosis, increasing pressure
At sink tissues (roots/storage), sugar is unloaded
Water leaves, lowering pressure
Sugar moves from high pressure (source) to low pressure (sink)
How is pressure involved in the movement of blood in vertebrates?
The heart acts as a pump
During ventricular systole, contraction increases pressure in arteries
Blood flows from high pressure (ventricles/arteries) to lower pressure (capillaries → veins → atria)
Pressure gradually decreases along pathway: Arteries → Arterioles → Capillaries → Venules → Veins
Ventricles generate the most pressure because they have thicker muscle walls
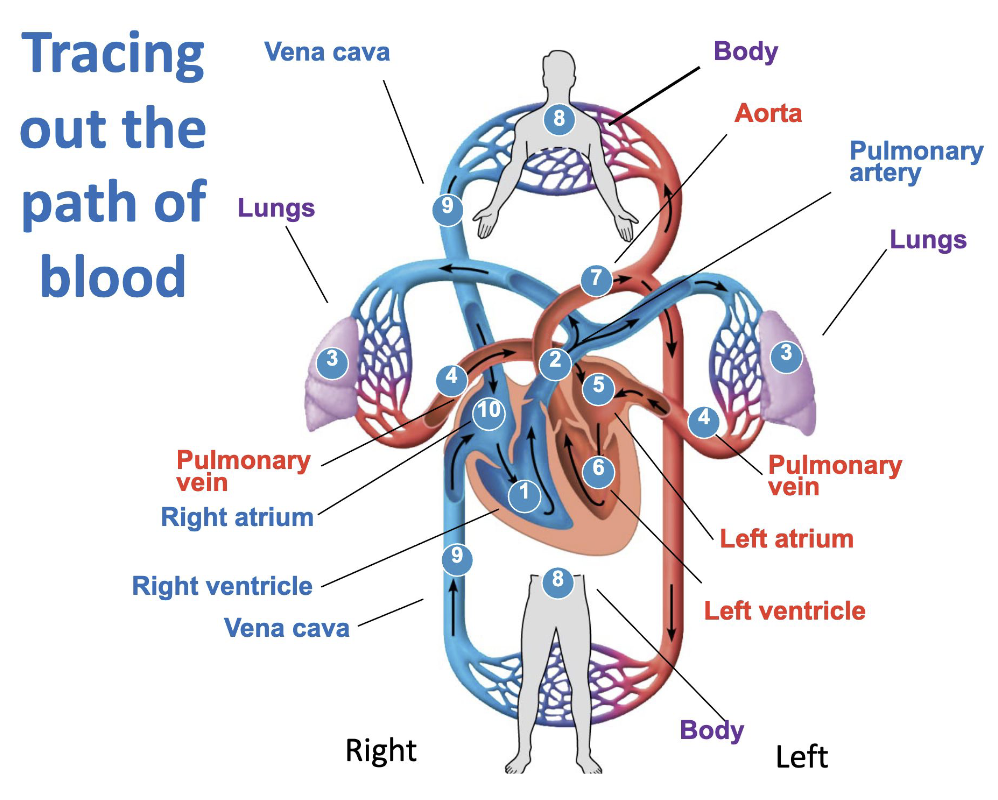
How does blood flow through the four chambers of the heart, the great vessels, lungs, and the blood vessels?
Blood passes the heart twice
Body to heart (Systemic circuit) (deoxygenated)
Body capillaries → Venules → Veins → Vena cava → Right atrium
In heart to lungs (Pulmonary circuit)
Right atrium → Right ventricle → Pulmonary artery → Lung capillaries → Pulmonary veins → Left atrium → Left ventricle
Heart to body (System circuit) (oxygenated)
Left ventricle → Aorta → Arteries → Arterioles → Capillaries
Arteries → Arterioles (Away from heart)
Veins → Venules (Toward heart)
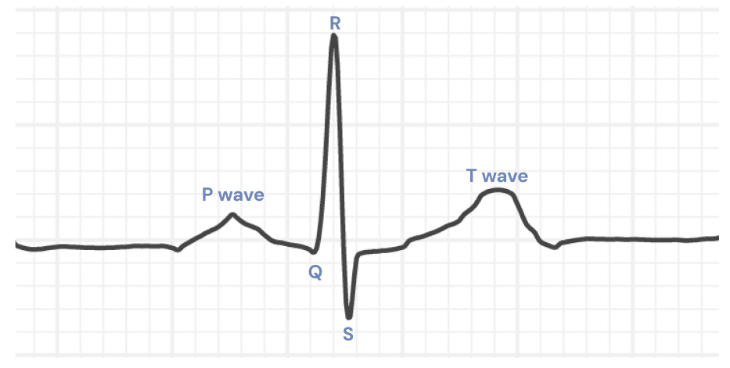
Draw out the ECG associated with heart beat and describe what is occuring during each section of the graph.
P wave
Atrial contraction
Generated by the SA node
Atrial depolarization occurs
QRS
Ventricular contraction
T wave
Ventricular relaxation
What are the components of the circulatory system?
Fluid in which materials are transported (blood)
A pump to move the fluid around (heart)
Vessels to provide controlled paths (veins, arteries, capillaries)
What are the roles of the veins, venules, capillaries, arterioles, & arteries?
Veins: Carry blood toward the heart
Venules: Connect capillaries to veins
Capillaries: Allow for exchange of O2/CO2, nutrients, & waste
Arterioles: Control blood flow into capillaries & help regulate blood pressure
Arteries: Carry blood away from the heart
What is the cardiac cycle, & what it its order?
Cardiac cycle: One complete phase of pumping & filling
Contraction phase is systole
Relaxation phase is diastole
Order:
Atrial & ventricular diastole
Atria & ventricles are relaxed, & blood is returning to the heart
Atrial systole (ventricular diastole)
Atria contract, ventricles are still relaxed
Ventricular systole (atrial diastole)
Ventricles contract
Pushes blood to the next structure
What happens if the SA node is destroyed?
The AV node becomes the pacemaker, and there are no P waves
What happens if the atria do not depolarize normally?
Atrial contraction is abnormal or absent
Ventricles still contract, but rhythm may be slower
How does the electrical signal travel in the heart?
Sinoatrial node: Pacemaker
Spreads to atria
Spreads to atrioventricular node
Spreads down the septum
Spreads out to both ventricles
What are the differences between systolic & diastolic blood pressure?
Systolic blood pressure
Arterial blood pressure during ventricular contraction
It is the higher number in a blood pressure reading because ventricular contraction generates the greatest pressure
Pumping pressure
Diastolic pressure
Arterial blood pressure during ventricular relaxation
It is the lower number because the heart is not actively contracting, so arterial pressure falls
Resting pressure
What are cross-sectional & total cross-sectional area, & what is the pattern in the body?
Cross-sectional area: The area of a vessel if you slice it & look at the opening
Total cross-sectional area: The sum of all vessels at that level
Pattern in the body:
Small in aorta (one large vessel)
Larger in arteries
Largest in capillaries (because there are millions of them)
Decreases again in veins
Capillaries have the greatest total cross-sectional area
How is velocity related to total cross-sectional area? What is the pattern of blood velocity & why?
Total cross sectional area & velocity are inversely related
If total cross-sectional area increases → velocity decreases
If total cross-sectional area decreases → velocity increases
Pattern:
Highest near heart (aorta, arteries)
Decreases dramatically in capillaries
Increases somewhat again in veins (but not as high as arteries)
Cause:
Pressure (higher pressure → faster velocity)
Total cross-sectional area (lower area → Faster velocity)
How is pressure related to total cross-sectional area? What is the pattern of blood pressure?
Pattern:
Highest in aorta & arteries
Gradually decreases through arterioles
Much lower in capillaries
Lowest in veins & vena cavae
Cause:
Pressure is generated by ventricular contraction
As blood moves through vessels, energy is lost due to:
Stretching of vessel walls
Friction within vessels
Pressure steadily declines with distance from heart
What are pressure, total area, & velocity like in the aorta, capillaries, & veins?
Aorta
High pressure
Low total area
High velocity
Capillaries
Lower pressure
Highest total area
Lowest velocity
Veins
Very low pressure
Lower area than capillaries
Moderate velocity
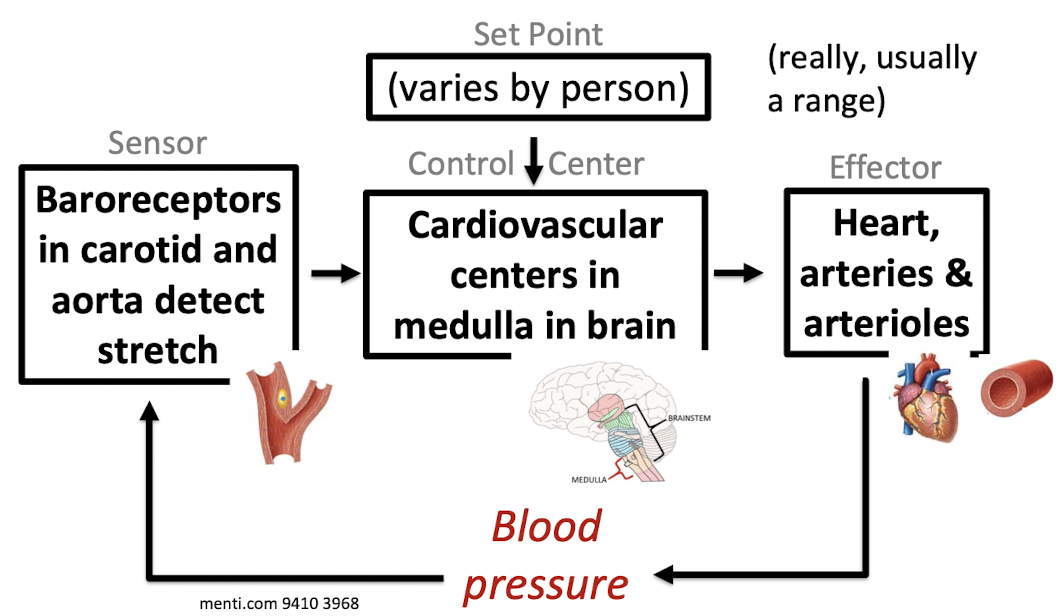
How is blood pressure controlled homeostatically?
If blood pressure is low, heart rate increases & arteries & arterioles constrict, making blood pressure rise
If blood pressure is high, heart rate decreases & arteries & arterioles relax, making blood pressure fall
How do changes in body posture affect homeostatic control of blood pressure?
When a person stands up suddenly:
Gravity pulls blood downward
Less blood returns to the heart
Arterial blood pressure falls
Homeostatic response:
Baroreceptors detect less stretch
Signal sent to medulla
Effectors respond:
Heart rate increases
Arteries & arterioles contrict
Result:
Blood pressure rises back toward the set point
If this reflex did not occur → Dizziness or fainting
How do changes in baroreceptor function affect homeostatic control of blood pressure?
Typically, when blood pressure increases:
Baroreceptors detect increased stretch
Medulla decreases heart rate
Arteries relax (vasodilation)
Blood pressure falls toward normal
If baroreceptors cannot detect stretch:
Changes in blood pressure are not sensed properly
The medulla does not adjust heart rate or vessel diameter appropriately
Blood pressure becomes unstable
Standing up could cause prolonged drops in pressure
If baroreceptors reset to a higher set point, like in chronic hypertension:
High blood pressure is treated as acceptable
Homeostatic correction does not occur
Hypertension (high blood pressure) persists
How will blood pH levels change when the kidney reabsorbs bicarbonate ions? When bicarbonate ions are secreted?
Reabsorption
From filtrate back to blood
Adds bicarbonate back to the blood
Blood pH increases (becomes more basic)
Occurs when body needs to correct low blood pH
Secretion
From blood to filtrate
Removes bicarbonate from the blood
Blood pH decreases (becomes more acidic)
Occurs when body needs to correct high blood pH
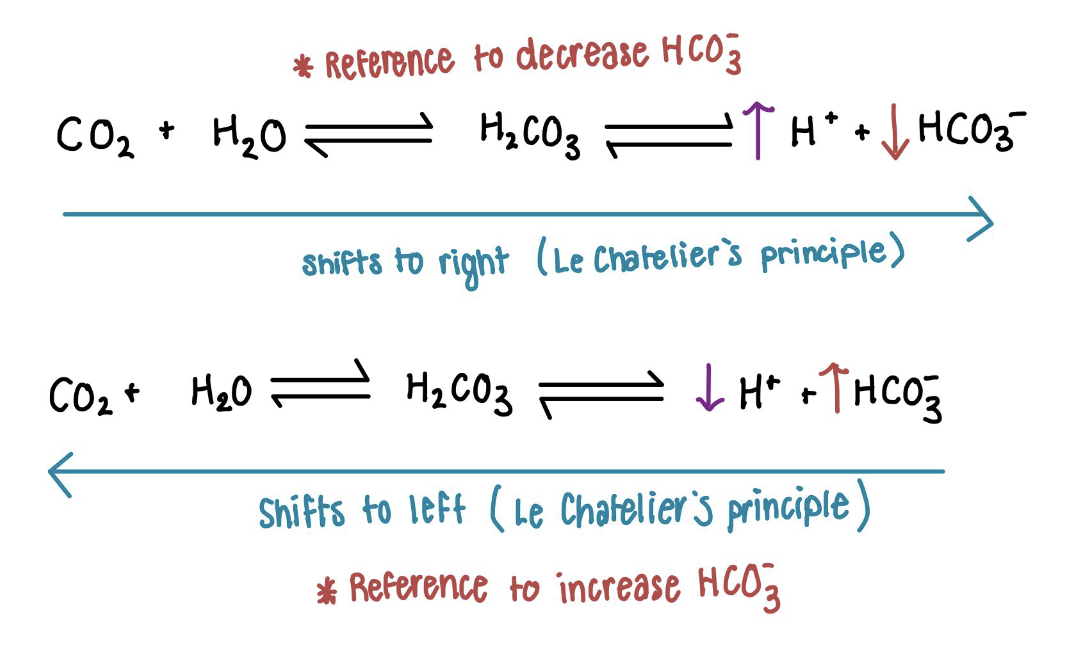
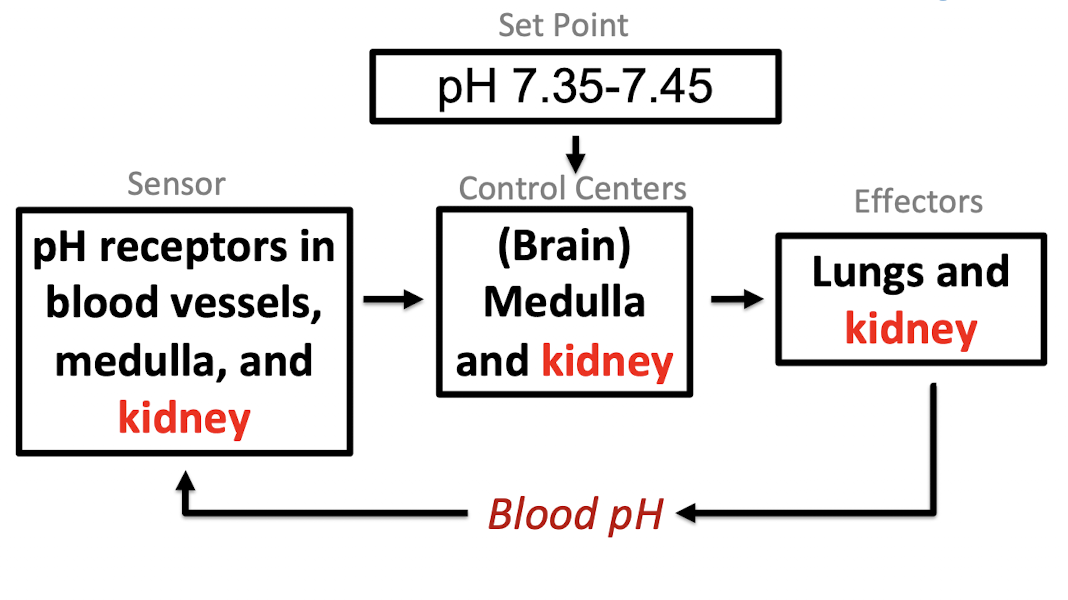
Map out how blood pH is homeostatically controlled.
Map out the creation, processing, & path of filtrate in the human kidney.
Glomerulus: Blood pressure forces arteriole blood through slits to make the filtrate. Small things like water, ions, & sugars can go through the filter, but not cells or proteins.
Proximal tubule
Filtrate has been made, so things can go back into the blood
Glucose, amino acids, water, sodium, & bicarbonate are reabsorbed by blood
Most of the reabsorption is done here
The filtrate ends isosmotic
Descending nephron loop
Water leaves filtrate & is reabsorbed into the blood
Filtrate ends hyperosmotic
Ascending nephron loop
Sodium is reabsorbed into the blood
Extracellular fluid in medulla is salty
Actively pumps salt out
Filtrate ends hyposmotic
Distal tubule
Water is reabsorbed if there is ADH, and sometimes bicarbonate is reabsorbed
Filtrate ends hyposmotic without ADH, isosmotic with ADH
Collecting duct
Water is reabsorbed if there is ADH because the ADH inserts aquaporins into the membrane, which allow water to flow out because the medulla fluid is saltier
Sometimes sodium & bicarbonate are reabsorbed into the blood
Bicarbonate is sometimes secreted into the filtrate
Filtrate ends hyposmotic without ADH or hyperosmotic with ADH
What happens when glomerular filtrate rate is low? High?
Low GFR
Waste products stay in tubule too long & move back into the body
Too much fluid is retained in blood
Filtration stops & wastes/excess fluids remain in blood
High GFR
Important materials flushed out with urine before they’re recovered
Too much fluid loss
Damage to glomerular capsule & kidney failure
How do the kidneys control GFR?
Myogenic mechanism
Smooth muscle around the arteriole detects stretch & controls the arteriole’s size
High blood pressure stretches the arteriole → arteriole constricts → less blood in kidney → GFR lower
Low blood pressure → arteriole is not stretched → more blood in kidney → GFR higher
Local; only affects the glomeruli
Controls how much blood reaches the glomeruli
More blood flow → higher GFR
Controlling the renin-angiotensin-aldosterone system
Global; affects the whole body
Controls the blood pressure of all the body’s blood
Higher blood pressure → higher GFR
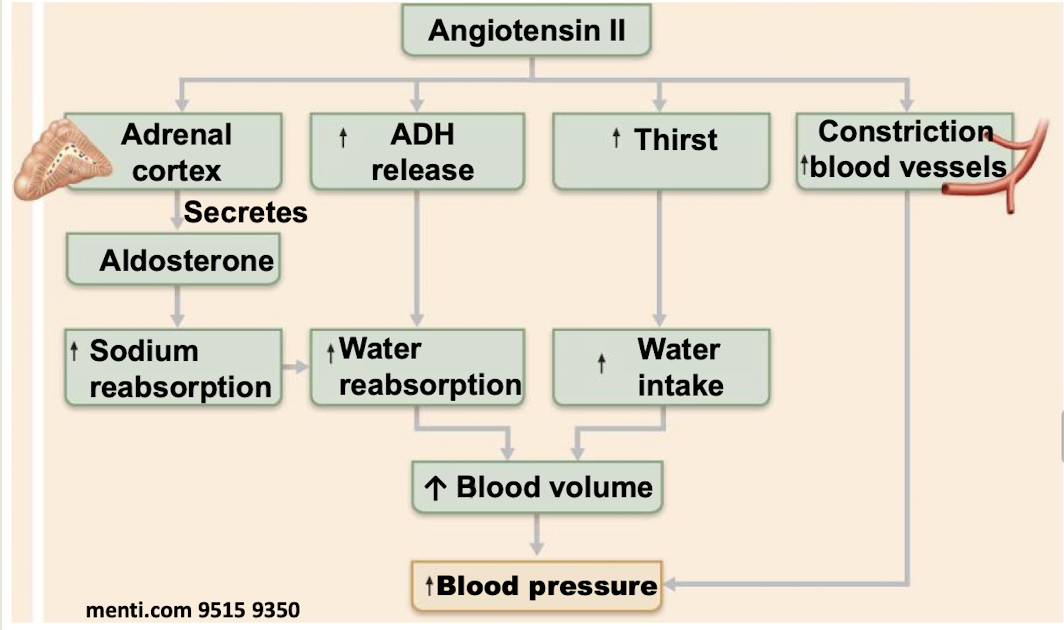
How do changes in the renin-angiotensin-aldosterone system affect blood volume & pressure?
Low GFR causes the release of the hormone renin
Renin causes the formation of angiotensin I
Angiotensin I turns into hormone angiotensin II
Angiotensin II causes the adrenal glands to release the hormone aldosterone
Aldosterone increases the reabsorption of sodium in the distal tubule & collecting duct, making the blood saltier
Blood pressure & volume increase because the increased salt concentration in the blood attracts more water through osmosis
What are the different types of osmolarity?
Hyperosmotic → Concentrated
Isosmotic
Hyposmotic → Dilute
How do the functions of the distal tubule & collecting duct change with & without ADH?
With ADH: Water is reabsorbed from the filtrate into the urine
In the distal tubule, filtrate stays hypotonic & ends isotonic
Fluid around the collecting duct is very salty, so filtrate goes from isotonic to hypertonic
Without ADH: Water is not reabsorbed & stays in the filtrate
In the distal tubule, filtrate starts & ends hypotonic
In collecting duct, filtrate starts & ends hypotonic
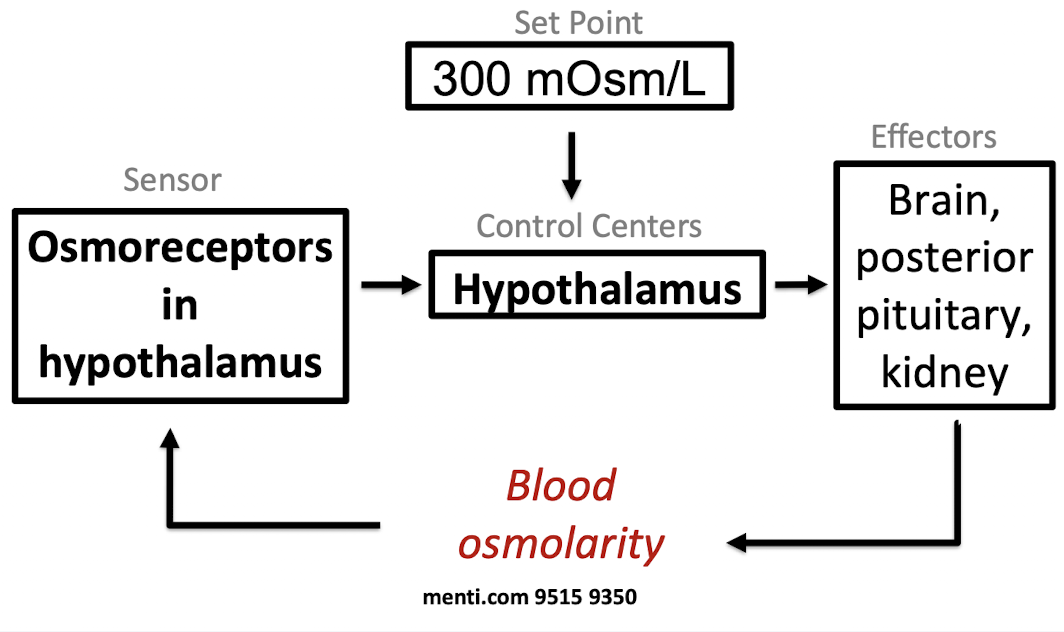
How is blood osmolarity homeostatically controlled? Map it out.
When osmolarity is high:
Hypothalamus contacts other parts of the brain, to create a feeling of thirst
Hypothalamus tells the posterior pituitary to release more of the hormone anti-diuretic hormone (ADH)
When osmolarity is low:
Hypothalamus tells the posterior pituitary to release less of anti-diuretic hormone (ADH)
Map out the effects of angiotensin II.
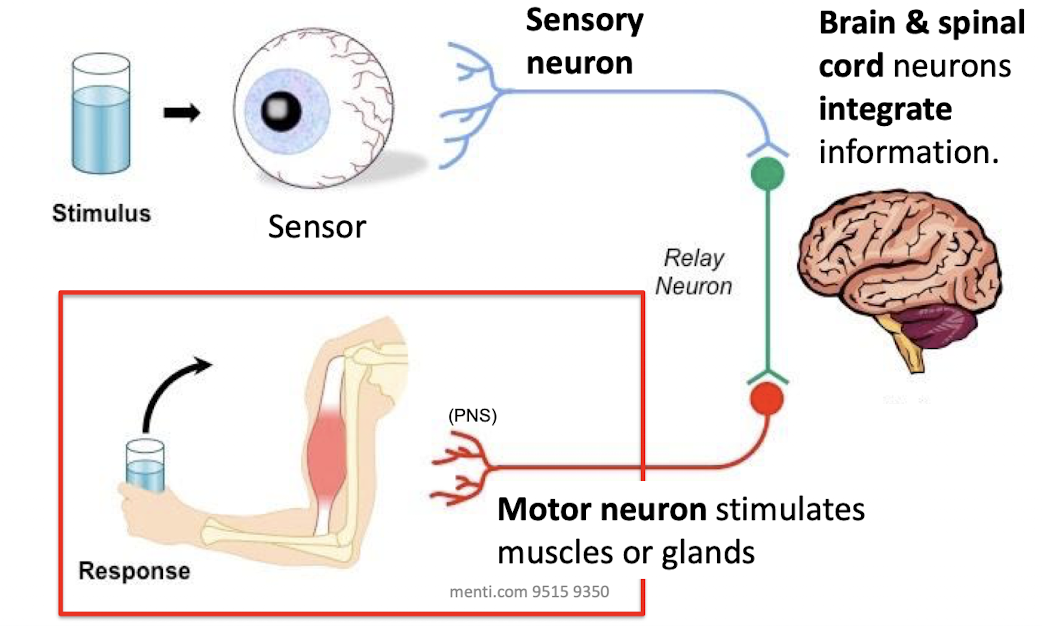
Map out the flow of information in the nervous system.
What are the different types of muscle? What are sarcomeres & do they have sarcomeres?
Skeletal
Attached to bones
Voluntary movement
Have sarcomeres
Cardiac
Walls of the heart
Involuntary movement
Have sarcomeres
Smooth
Walls of hollow, visceral organs
Involuntary movement
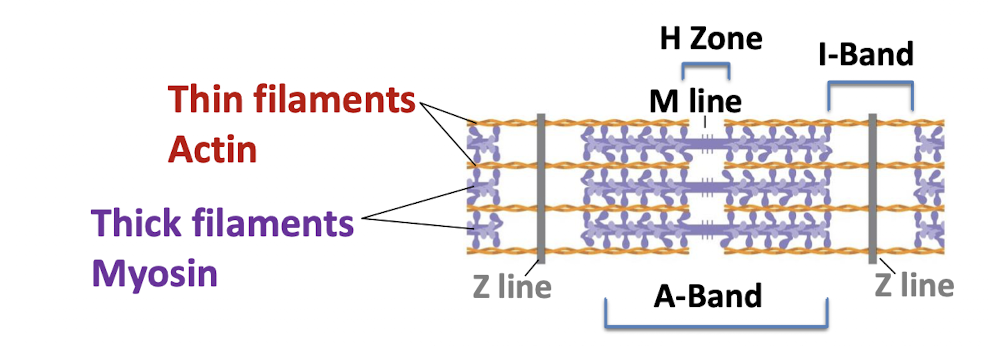
How do thin filaments, thick filaments, and Z lines move during muscle contraction?
During contraction, thick & thin filaments slide together lengthwise
Thin filaments (actin) slide toward the center of the sarcomere
Thick filaments (myosin) stay in the same position
Z lines move closer together as the sarcomere shortens
What are the steps of skeletal muscle fiber contraction?
Neuron has an action potential, which activates the neuromuscular junction
In the neuromuscular junction:
The action potential in the neuron opens voltage-gated calcium channels
Calcium influx into the neuron causes the release of acetylcholine
Acetylcholine binds to its receptor on the muscle fiber, opening a channel that lets in sodium
Acetylcholine is broken down in the cleft by acetylcholinesterase
The muscle has an action potential, and the signal propagates to the rest of the muscle
Muscle contracts using cross bridge cycling
How is muscle contraction influenced by calcium?
Without calcium
Myosin heads cannot bind to actin because tropomyosin is bound to actin and is in the way
With calcium
Ca2+ binds to troponin
Troponin moves tropomyosin off the actin binding sites so the actin & myosin can form cross bridges
Myosin head turns & pulls thin filaments to contract
ATP binding to the myosin detaches the cross bridges
Energy from ATP hydrolysis moves myosin back into the initial state
What are the differences between the sympathetic & parasympathetic nervous system?
Parasympathetic
Rest & digest
Promotes maintenance functions & conserves body energy
Promotes low blood pressure, low heart rate, & digestion
Sympathetic
Fight or flight
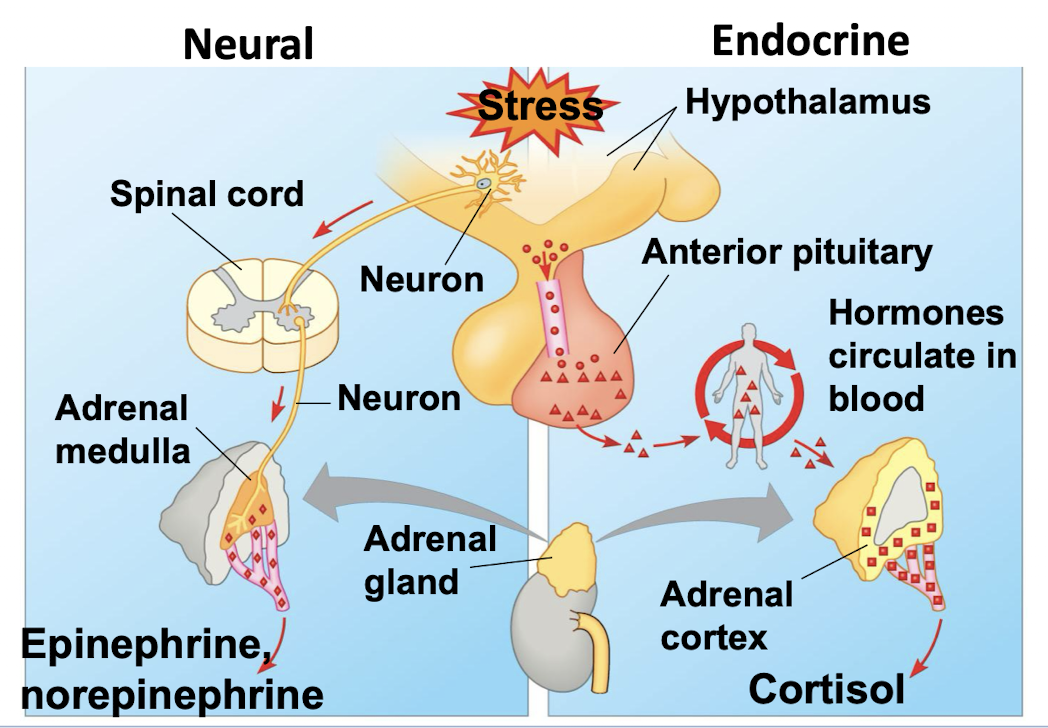
Release epinephrine & norepinephrine
Increase heart rate
Increase blood pressure
Vasoconstriction
Increase blood sugar
What are the two parallel stress pathways?