Psychological Interventions Lecture 10
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
Persistant Depressive Disorder
Duration > 2 years
More physical and psychological symptoms
More psychosocial problems
More suicide attempts
Longterm care
More (childhood)trauma
> 20%of depressions becomes persistent
In specialistic mental health care higher percentages (>50%)
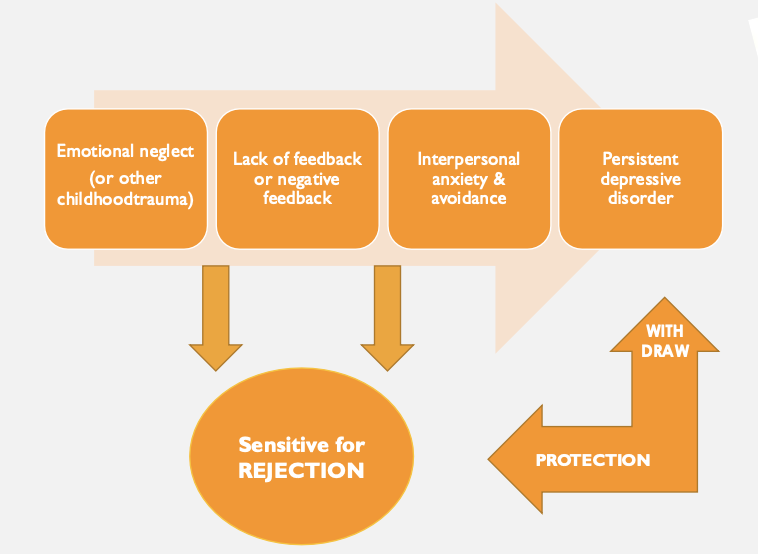
Childhood Trauma (before age of 16) in people with Persistent Depressive Disorder
Emotional neglect (people often don’t know)
Psychological abuse
Physical abuse
Sexual abuse
CBASP Meta analysis (Negt e.a. 2016)
CBASP > CAU (usual care)
CBASP = AD (medication)
CBASP + AD > AD
Theory of CBASP
People with chronic mental disorders:
Think and talk in a global terms
Have a strong focus on themselves
Find it hard to mentalize
Have a hard time verbalizing their feelings
Feel like a playball of life (no sense of control)
People are unaware that their primitive verbal thought and behavior patterns serve to keep them perceptually disconnected from the environment → Unresponsive to environmental consequences and feedback
→ Make people feel hopeless and helpless about their situaton → makes it hard to look for help
Developmental Model Piaget
Persistently depressive patients function on a ‘preoperational’ level:
difficulty in understanding others' perspectives
not aware they can influence and change their own reality
see no connection between what they do and the effects of it
Goal CBASP
CBASP teaches the patient to move from a ‘preoperational’ level to an ‘operational’ level of functioning: the patient becomes aware of their own role in an interaction and the possibility to change this role.
Replace disconnectedness with perceived-functionality expectancy set and empathy
‘Everything you do has effect’
Transference Domains
Intimacy / closeness
Expressing emotional needs
Making mistakes
Expressing negative emotions
Transference Hypothesis
Therapist and patient formulate these hypotheses based on past experiences
E.g. if I express negative emotions, than my therapist will find me difficult
Impact Message Inventory
To be completed after a few sessions
Recognize the patient's behavior
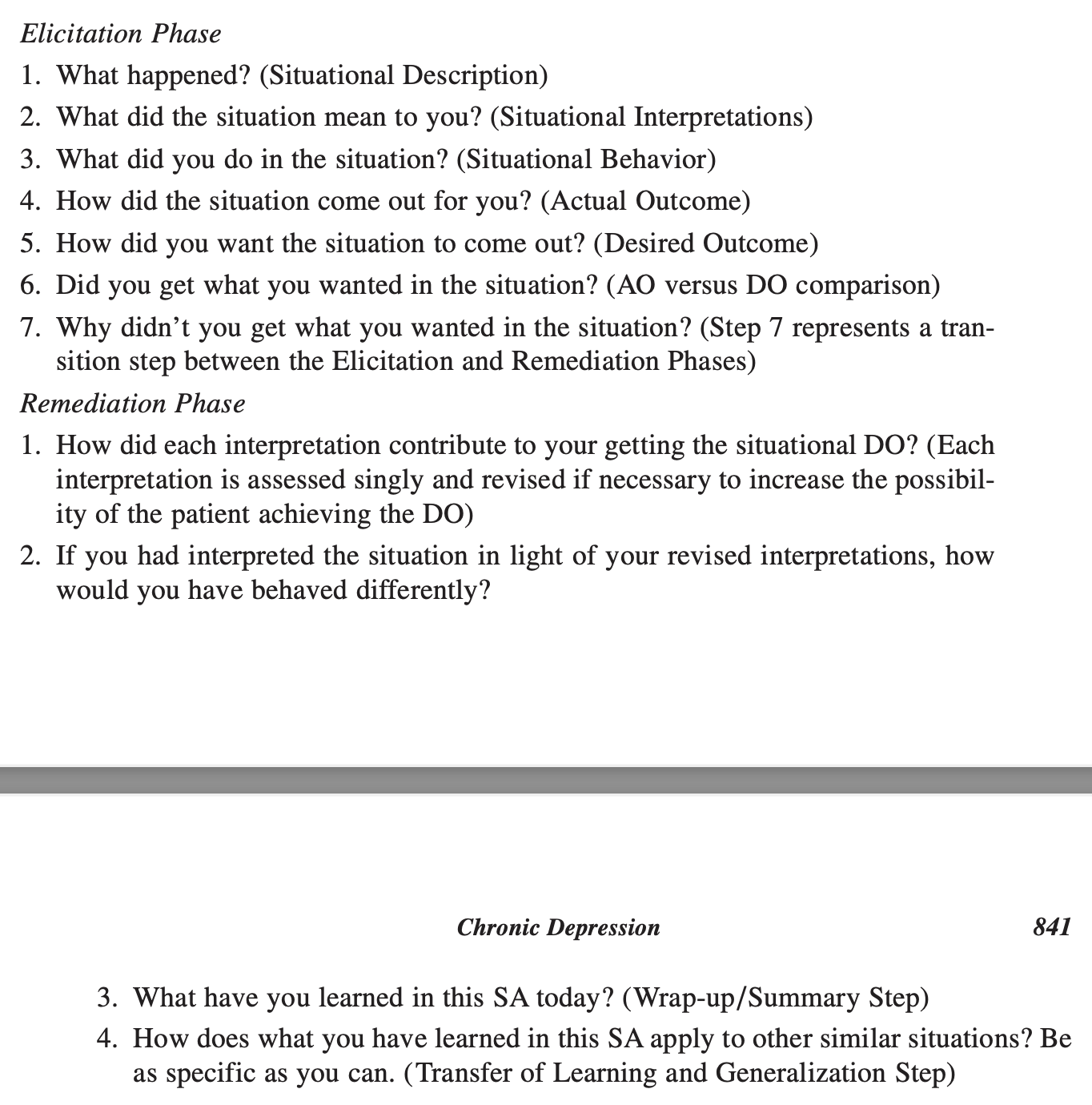
Situational Analysis
Most important technique of intervention phase
Goal: Recognize the consequences of interpersonal behavior
Focus on a concrete problematic situation with an interaction
A form with several steps/questions to help patients become more aware of their thoughts and behavior and how it affects the outcome of the situation
To teach them how to think and act differently in order for them to get what they want
To gain control over social situations
Exercise consists of elicitation phase and remediation phase
Interpersonal Discrimination Exercise
Goal: Learn to recognize new interpersonal experiences
The therapist identifies a “hot-spot situation,” for example based on a Situational Analysis (SA)
How would your mother/father have reacted in a similar situation?
How did I react? What did you notice about me? What did I say?
What is the difference between my reaction and that of your mother/father?
If I react differently, what does that mean for the relationship between us?
Are there others who would react in a similar way like me?
Disciplined Personal Involvement
Goal: Identify the consequences of the patients behavior
Recognize the interpersonal impact of the patients behavior on the therapist and explain the consequences of the behavior
Pay attention to alternative (more functional) behaviors and it’s impact
Optimal Therapist Role Characteristics
Able to enact a Disciplined Personal Involvement clinical role with the patient
Able to implement an acquisition-learning approach to therapeutic administration
Able to adhere to the standards of CBASP technique administration
Able to implement several facilitative interpersonal skills.
Able to enact a Disciplined Personal Involvement clinical role with the patient
The therapist is a real, genuine person with the patient instead of acting distant or “robotic.”
The therapist pays attention to how the patient affects them emotionally.
They use their own reactions carefully to help the patient learn healthier relationships.
The therapist creates a safe relationship, especially for patients with trauma or abuse histories.
“I will relate to you honestly and safely, so you can learn that relationships do not always have to be harmful.”
Able to implement an acquisition-learning approach to therapeutic administration
CBASP sees therapy as a learning process.
The therapist acts like a teacher:
Patients learn how relationships work.
Patients learn how their behavior affects others.
Patients practice new ways of thinking and acting.
“If patients learn new interpersonal skills, their depression becomes more manageable.”
Able to adhere to the standards of CBASP technique administration
Good therapists know how to properly use the main CBASP tools, such as:
Significant Other History (SOH)
Interpersonal Discrimination Exercise (IDE)
Situational Analysis (SA)
These techniques help patients:
feel safe with the therapist,
understand consequences of their behavior,
and break old unhealthy patterns.
Able to implement several facilitative interpersonal skills, such as
patience,
authenticity,
handling silence,
managing anger,
pacing therapy at the patient’s speed,
staying calm during difficult emotions,
and maintaining good communication control.