NURS 471 Critical Care Week 2: Ch. 4 Cardiac Dysrhythmias
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
Properties of Cardiac Cells
automaticity, excitability, conductivity, and contractility.
Automaticity
is the ability of pacemaker cells to spontaneously initiate an impulse; normally this belongs to the SA node, AV junction, and Purkinje fibers.
Excitability
is the ability of cardiac cells to respond to an electrical stimulus.
Conductivity
is the ability to transmit the impulse from cell to cell.
Contractility
is the ability of cardiac muscle cells to shorten in response to electrical stimulation.
P wave
represents atrial depolarization.
PR interval/segment
reflects conduction delay through the AV node, which allows time for ventricular filling.
Normal PR Interval
0.12-0.20 seconds (3-5 small boxes)
An interval greater than 0.20 second suggests first-degree AV block.
QRS Complex
represents ventricular depolarization and triggers ventricular contraction.
QRS Duration
should generally be less than 0.10 to 0.12 second
ST segment
marks the beginning of ventricular repolarization and should be flat on the isoelectric line.
T wave
represents ventricular repolarization.
QT Interval
ventricular depolarization and repolarization
Duration: <0.38 sec.
5-Lead Placement
RA = White 2nd ICS
RL = Green Last ICS
LA = Black 2nd ICS
LL = Red Last ICS
Chest = Brown 4th ICS right sternal border.
12-Lead Placement
>V1-V2: each aligned in the 4th intercostal spaces; V1 on the right of the sternum and V2 on the left
>V3: on the 5th left rib (between 4th and 5th intercostal spaces)
>V4: left 6th intercostal space
>V5: anterior axillary line at the same level as V4
>V6: midaxillary line at the same level as V4 and V5
>RL/LL: anywhere above ankle and below torso
>RA/LL: anywhere between the shoulder and the elbow
Leads II, III AVF view which portion of the heart?
assess the inferior wall and often correspond to the right coronary artery territory.
Because the right coronary artery often supplies the SA node, inferior infarcts may be associated with heart blocks.
Leads I, AVL, V5 & V6 view which portion of the heart?
lateral wall
Leads VI and V2 view which portion of the heart?
septal wall
Leads V3 and V4 view which portion of the heart?
anterior wall
Limb Leads Show?
frontal plane
Precordial Leads Show?
horizontal plane
Shockable Rhythms
Ventricular Fibrillation
Pulseless Ventricular Tachycardia
Torsades de Pointes
in VF/pulseless VT, one shock should be delivered as soon as possible, with immediate return to CPR and minimal interruption.
CPR interruptions should be minimized, and medications should be given during CPR rather than interrupting compressions.
Epinephrine 1 mg IV/IO every 3 to 5 minutes is part of ACLS for persistent VF/pulseless VT.
Amiodarone is the antiarrhythmic of choice after repeated shocks and epinephrine, with lidocaine as another option.
ST Segment
Should be flat
•Normally on isoelectric line
•Represents early ventricular repolarization
•Varies with heart rate, electrolyte disturbances and medications
•Normally not elevated more that 1mm or depressed more than 0.5mm to 2mm
•ST elevation = infarction.
•ST depression = ischemia
QT Prolongation
can result from medications and electrolyte abnormalities and may predispose to torsades de pointes.
Heart Blocks
An AV block exists when conduction through the AV node or bundle of His is delayed or blocked.
AV blocks increase in seriousness from first-degree, to second-degree type I, to second-degree type II, to third-degree (complete) block.
third-degree heart block as the most serious because perfusion is poor when atria and ventricles beat independently.
Inferior MI may be associated with AV nodal ischemia and AV blocks because of right coronary artery involvement.
Type I and some bradyarrhythmias may be medication-related, especially from beta blockers, digoxin, or calcium channel blockers.
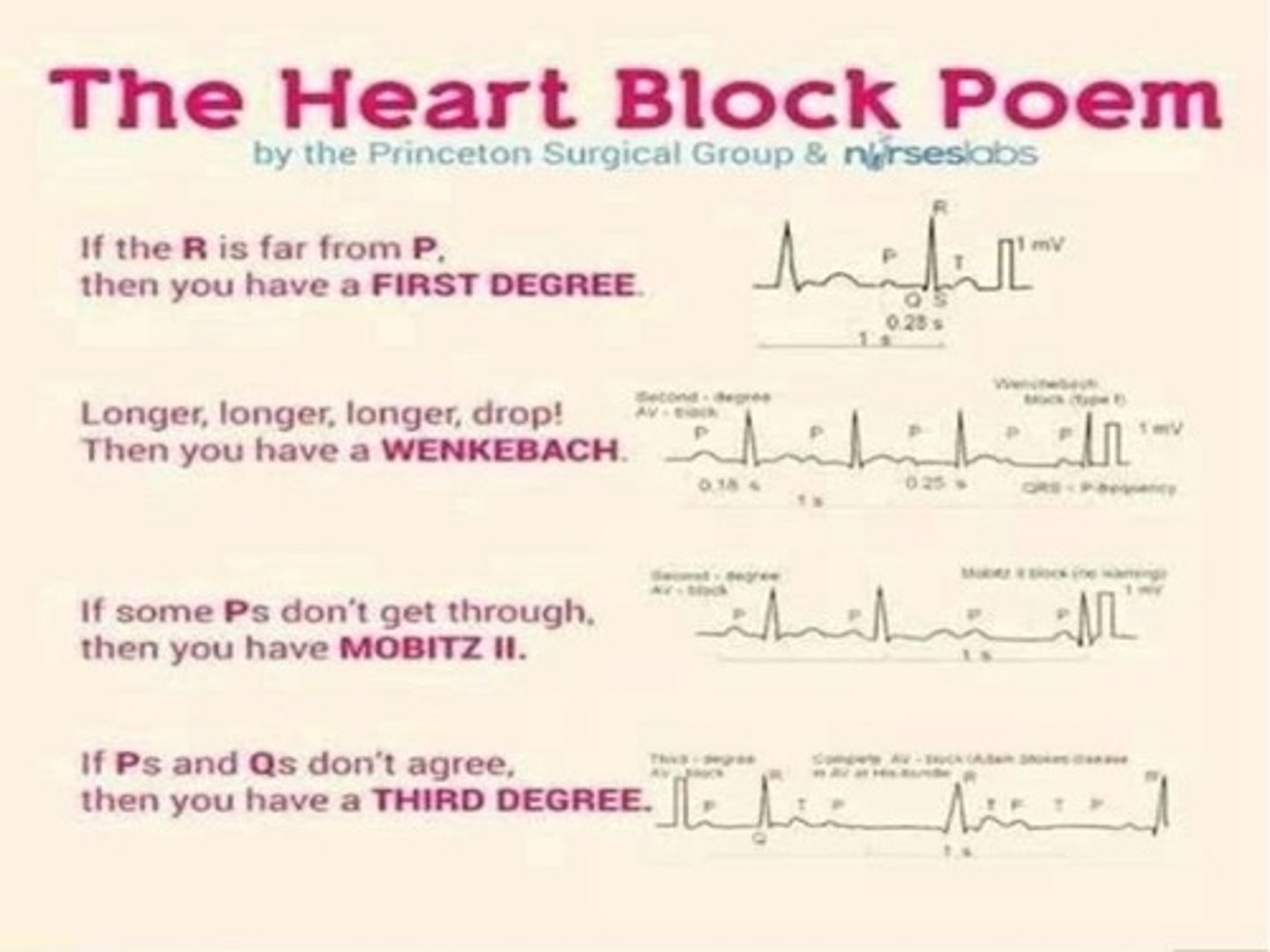
First Degree Heart Block
prolonged PR interval

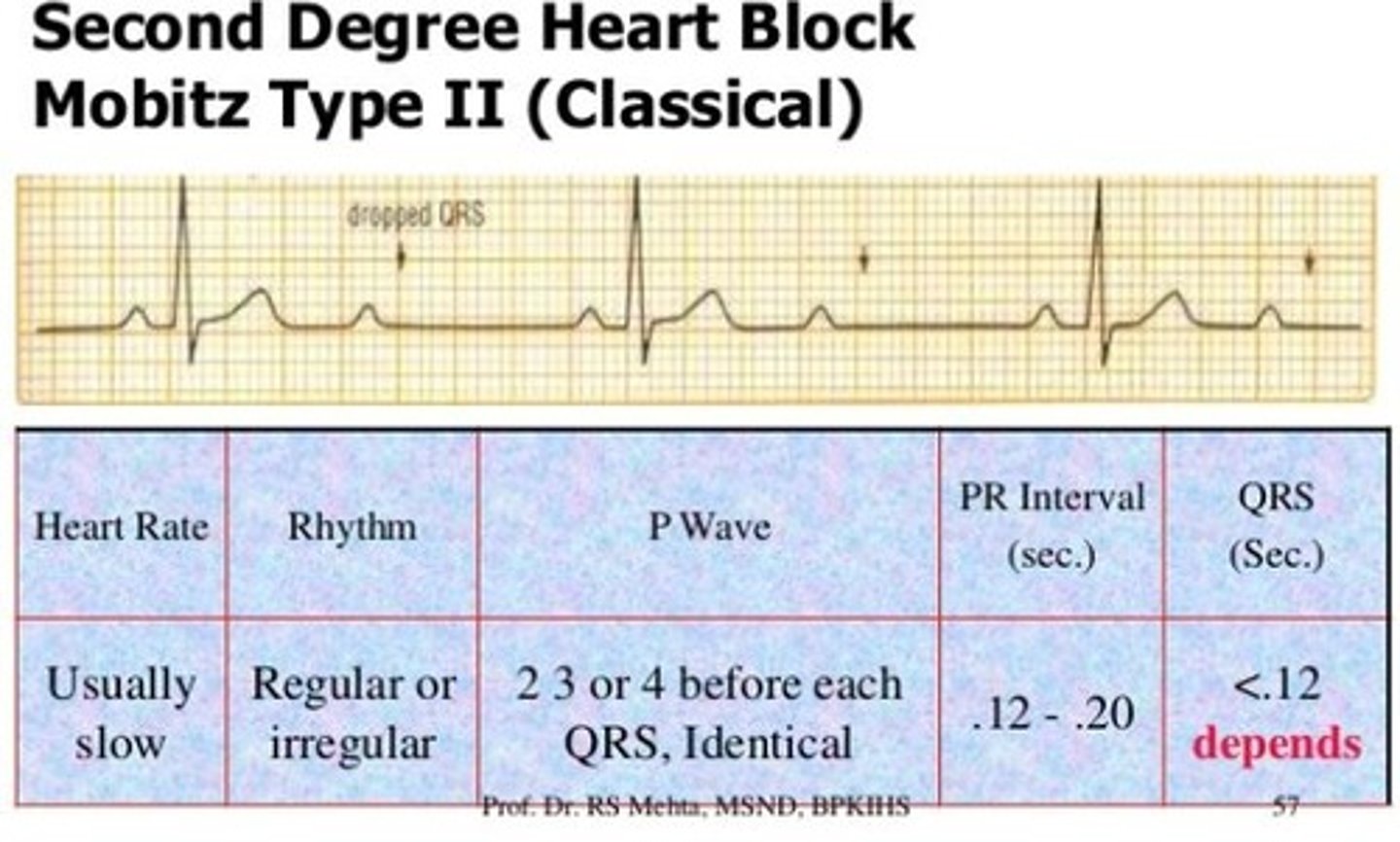
Second Degree Heart Block Type II (Mobitz II)
Series of nonconducted to conducted P waves is fixed. Consistent PR intervals, but not always followed by a QRS complex.
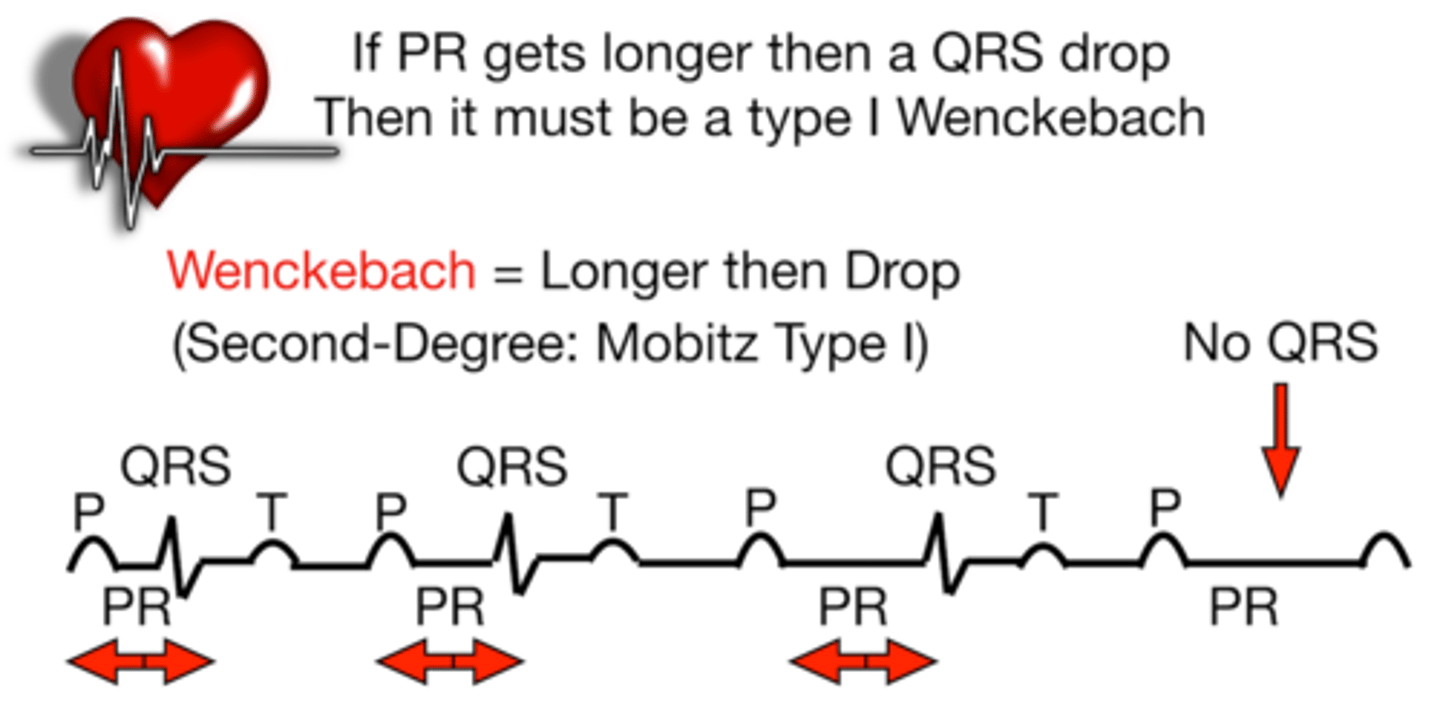
second degree heart block Type 1 (Wenckebach)
PR interval becomes longer with each succeeding complex until there is a P not followed by a QRS ("marching off")
Third-Degree Heart Block
AV block in which electrical impulses from the atria fail to reach the ventricles; also called complete heart block (CHB)
Ps and Qs don't agree
EKG Analysis
Analyze P wave: present, how many, regular?
Analyze QRS (R waves): present, how many, regular?
Determine heart rate.
Measure PR interval.
Measure QRS duration.
Measure QT interval.
Interpret rhythm.
When using a 6-second strip, rate can be estimated by counting the QRS complexes in 6 seconds and multiplying by 10.
ECG Timing
each small box = 0.04 second, each large box = 0.20 second, and 5 large boxes = 1 second at a standard speed of 25 mm/sec.
Defibrillation vs Cardioversion
Modern defibrillators can often function in AED mode, defibrillation mode, synchronized cardioversion mode, and pacing mode.
The clinical decision point is whether the rhythm is shockable, synchronized-shock appropriate, paceable, or non-shockable.
Pad Placement
Defibrillation/cardioversion pads can be placed in standard anterior-lateral configuration.
For some synchronized cardioversions, providers may prefer anterior-posterior placement (“sandwich” front and back).
Pad packaging often includes picture guides, and pediatric patients require appropriately sized pads.
The same multifunction pads may be used for defibrillation, cardioversion, and transcutaneous pacing depending on the device.
Defibrillation/AED
•Turn on & Apply Multifunction Pads to patient
•Determine rhythm
•Is it V-fib or pulseless V-Tach ? (ONLY SHOCKABLE RHYTHMS!!)
•Select appropriate joules
•Biphasic 120-200 (depending on manufacturer)
•Monophasic stackable 200, then 200-300, then 360
•If no physician or qualified personnel available, use AED mode
•BLS/CPR should be initiated ASAP and should only be interrupted when absolutely necessary (<10 seconds)
Synchronized Cardioversion
•Electrical charge is synchronized with the QRS of the patient’s heart rhythm R waves marked
•Patient placed on monitor with physician and emergency equipment at bedside
•Once pads are on, set defibrillator to synch, select proper electrical setting (MD determines amount of energy, 2025 AHA guidelines 200 joules)
•Pre-medicate patient if able
•Treatment of: unstable SVT, V-Tach with a pulse, A-Fib & A-Flutter
if SVT does not respond to medication, synchronized cardioversion is the next step.
VT with a pulse may also require synchronized cardioversion if unstable.
A-fib and A-flutter may be cardioverted when rhythm control is needed, but timing matters.
For A-fib of more than 48 hours or of unknown duration, the patient should generally be anticoagulated before cardioversion unless emergent instability requires immediate action or a TEE confirms absence of atrial thrombus.
Rapid atrial pacing may be attempted for atrial flutter in patients who have a permanent pacemaker or epicardial wires.
What is a pacemaker?
A device designed to assist in stimulating the heart when the hearts intrinsic pacemaker is not functioning properly causing poor perfusion, especially in symptomatic bradycardia and high-grade heart block.
purpose is to restore a heart rate sufficient to maintain adequate cardiac output and tissue perfusion.
Main goal is to maintain CO & Perfusion
Symptomatic bradycardia/heart blocks
Components
•pulse generator & pacing leads
Modes
•Asynchronous ( fixed mode rare)
Synchronous ( demand mode)
Most pacemakers in current practice are in demand mode, meaning they fire only when needed.
Some devices can both pace and defibrillate, especially ICD/AICD systems.
Types of Pacemakers
Temporary
•Transcutaneous
•Internal
-Transvenous
-Epicardial
Permanent
Single Chamber Dual chamber
Transcutaneous pacing uses external pads connected to the defibrillator in pacing mode.
Transvenous pacing uses a pacing wire inserted into the right atrium or right ventricle and attached to an external generator.
Epicardial pacing wires are commonly used after open-heart surgery because post-op patients may develop dysrhythmias.
Temporary pacing may be used as a bridge if a block is believed to be medication-related and possibly reversible before deciding on a permanent pacemaker.
Mobitz II and third-degree block often require immediate temporary pacing and eventual permanent pacemaker placement.
NASPE/BPEG (NBG) code
tells you what each letter in a pacemaker mode means, position by position. Use it like a 5‑letter “decoder ring.”
Position I – Chambers paced
O = none
A = atrium
V = ventricle
D = dual (A & V)
Position II – Chambers sensed
O = none
A = atrium
V = ventricle
D = dual (A & V)
Position III – Response to sensing
O = none
T = triggered (fires when it senses)
I = inhibited (withholds pacing when it senses)
D = dual (T & I)
Position IV – Programmability / rate modulation
O = none
P = simple programmable
M = multi‑programmable
C = communicating
R = rate modulation (rate‑responsive)
Position V – Antitachyarrhythmia functions
O = none
P = pacing (anti‑tachy pacing)
S = shock
D = dual (pacing & shock)
Implantable Cardioverter Defibrillator (ICD)/Automated Internal Cardiac Defibrillator (AICD)
refers to an implanted device that continuously monitors heart rhythm and can treat dangerous ventricular arrhythmias with shocks; many modern devices can also provide pacing when needed.
Implanted under the skin, usually with leads to the heart, to detect and treat life-threatening rhythms.
Can deliver a shock for dangerous ventricular tachycardia or ventricular fibrillation.
Many ICDs can also pace the patient, so they may function as both pacemaker and defibrillator.
ICDs constantly monitor the heartbeat and respond when a dangerous rhythm is detected.
The main rhythms of concern are VT/VF, which are shockable ventricular arrhythmias associated with sudden cardiac death risk.
Some devices provide antitachycardia pacing and bradycardia pacing in addition to high-energy shock therapy, which is why implanted rhythm devices can overlap in function.
LifeVest
is the temporary external version—a wearable cardioverter-defibrillator used as a bridge when permanent ICD placement is delayed, uncertain, or temporarily inappropriate.
Single-Chamber Pacemaker
Pacemaker coding identifies the chamber paced, the chamber sensed, and the response to sensing.
P chamber paced.
S chamber sensed.
R chamber response.
Dual-Chamber Pacemaker
Can pace and sense in both the atrium and ventricle.
Pacemaker Settings
Rate = the HR rate to pace the heart. is the backup or target pacing rate.
Time = Miliseconds (MS) unit of measurement for timing intervals measurement in time
• ( R= 60 1 beat every second)
Output- Miliamps (MA) the unit of measurement for the electrical current needed to stimulate “capture.” must be high enough to produce capture, meaning each pacer spike successfully depolarizes the myocardium and produces a QRS.
Sensitivity : millivolts (mV) refers to the pacemaker sensing the intrinsic HR. determines how well the pacemaker can “see” intrinsic cardiac activity.
Sensitivity
is the pacemaker’s ability to detect the patient’s own intrinsic cardiac activity, and it is set in millivolts (mV).
The key thing to remember is the counterintuitive rule: a lower mV setting = more sensitive, while a higher mV setting = less sensitive.
Correct sensing lets the pacemaker stay in demand mode, pacing only when needed.
Fence analogy: A low fence lets the pacemaker “see” more, while a high fence blocks its view; in device language, lowering the mV threshold makes the pacemaker more sensitive.
If pacemaker can’t sense will not fire or capture.
Failure to sense (undersensing) means the pacemaker does not detect the patient’s intrinsic beat, so it may pace inappropriately or asynchronously.
Failure to capture means the pacemaker fires, but the myocardium does not respond; that problem is usually fixed by increasing output (mA), not changing sensitivity.
Pacemaker Malfunctions
•Failure to Pace
•Failure to Capture
•Failure to Sense
Failure to Pace
No electrical spikes are present. means the patient should be paced, but no pacer spikes appear on the strip.
Pacemaker is NOT delivering pacer impulses.
Possible causes: left in monitor mode instead of pace mode, loose connections, insufficient power/battery.
Failure to Capture
Visible pacer spikes with NO associated QRS complex. meaning the electrical impulse did not depolarize the myocardium.
Output of pacemaker pulse fails to make chamber depolarize.
Troubleshooting includes increasing milliamps/output until capture is achieved if using a temporary pacemaker.
Possible causes: wire migration, output too low, loose connections, electrolyte imbalances, acid-base problems, meds.
Failure to Sense
Pacemaker spikes erratic, not aligned with QRS. pacing spikes occurring inappropriately, sometimes “all over the place,” not timed correctly with intrinsic beats.
Pacemaker fails to detect intrinsic rhythm and does not pace appropriately.
Possible causes: sensitivity too high, lead fracture/displacement, battery, electromagnetic interference. If the device cannot properly recognize intrinsic activity, it may fire when it should remain inhibited.
Permanent-device failure to sense may require formal device interrogation and reprogramming.
SA node intrinsic rate
60 to 100 bpm.
AV junction intrinsic rate
40 to 60 bpm.
Purkinje/ventricular escape rate
20 to 40 bpm.
Refractory periods
Absolute refractory period: cells will not respond to stimulation, roughly from QRS onset to T-wave peak.
Relative refractory period: vulnerable period when a strong stimulus can trigger dangerous dysrhythmia, including the R-on-T phenomenon and ventricular fibrillation.
Supernormal period: a weaker than normal stimulus can trigger depolarization.
Normal sinus rhythm (NSR)
Originates in SA node, travels through conduction system unimpaired at normal rate and rhythm.
Defined by:
Regular rhythm.
Rate 60–100 bpm.
Normal P before every QRS, PR 0.12–0.20, QRS <0.12.

Premature atrial complexes
Rhythm: regular except for premature beat(s).
Rate: usually normal overall.
P wave of PAC: may be upright, flattened, notched, or buried in preceding T; typically different shape from sinus P.
P:QRS ratio: 1:1.
PR: 0.12–0.20 sec, may be prolonged in the PAC.
QRS: narrow, <0.12 sec.
PACs are early atrial beats that may have altered P-wave shape and are usually benign.
Causes include stress, anxiety, fatigue, nicotine, caffeine, alcohol, stimulants, CHF, ischemia, and electrolyte imbalance.
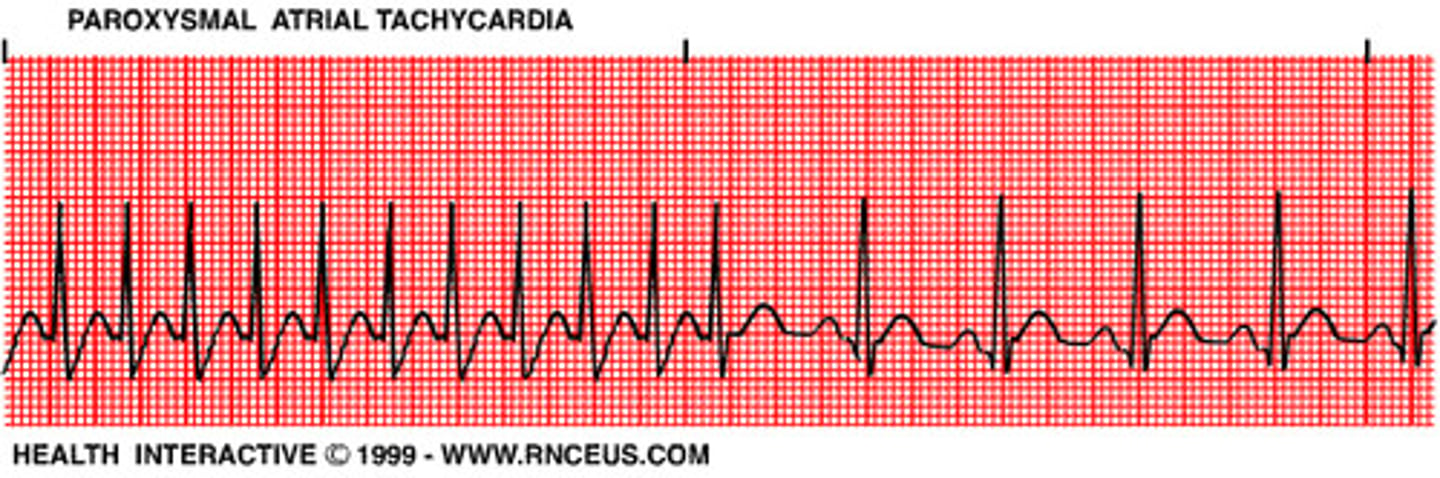
Supraventricular tachycardia
SVT is a regular narrow-complex tachycardia usually 150 to 250 bpm.
P waves may be hidden in T waves, so PR is often hard to measure.
Stable SVT can be treated with oxygen, IV access, cardiac monitoring, and vagal maneuvers.
Adenosine is first-line if vagal maneuvers fail.
Adenosine administration is a 6 mg rapid IV push, then 12 mg if needed, while expecting a brief period of asystole.
Adenosine should not be used for irregular wide-complex tachycardias, because it can precipitate VF.
Supraventricular tachycardia Treatment
For stable patients:
Oxygen, IV access, continuous cardiac monitoring.
Vagal maneuvers (bearing down, gagging, carotid sinus massage—only by provider) terminate SVT in ~20–25% of patients.
If ineffective or only temporarily helpful, adenosine is first‑line: transient AV nodal block → brief asystole and potential conversion to sinus.
For unstable patients (hypotension, chest pain, altered mental status): immediate synchronized cardioversion.
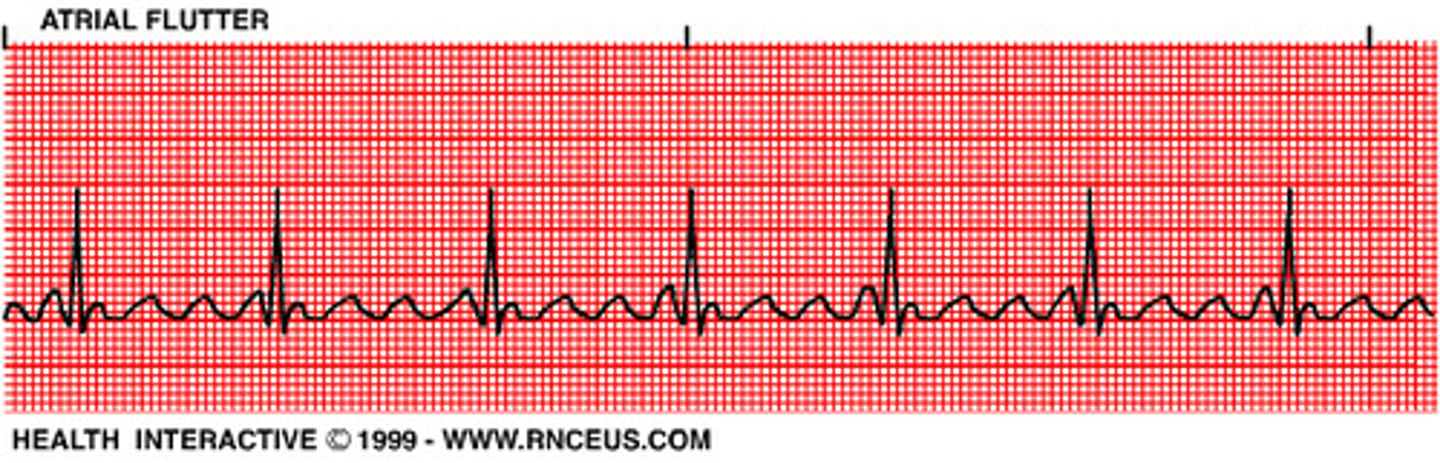
Atrial flutter
usually has an atrial rate around 250 to 350 bpm with a sawtooth pattern.
The ventricular response depends on AV conduction; examples may be described as 2:1, 3:1, etc.
PR interval: usually not measurable.
QRS: narrow.
Treatment includes rate control, antiarrhythmics, or synchronized cardioversion.
Atrial flutter – treatment focus
Patients are often asymptomatic, but symptoms increase as ventricular rate rises.
Primary goal in rapid ventricular response: slow the ventricular rate.
Rate control: beta blockers or calcium channel blockers (e.g., diltiazem) as with SVT.
Rhythm control: antiarrhythmics (e.g., amiodarone) or synchronized cardioversion to restore NSR.
In patients with pacemakers/epicardial wires, rapid atrial pacing may be used to override the flutter focus and allow SA node control.
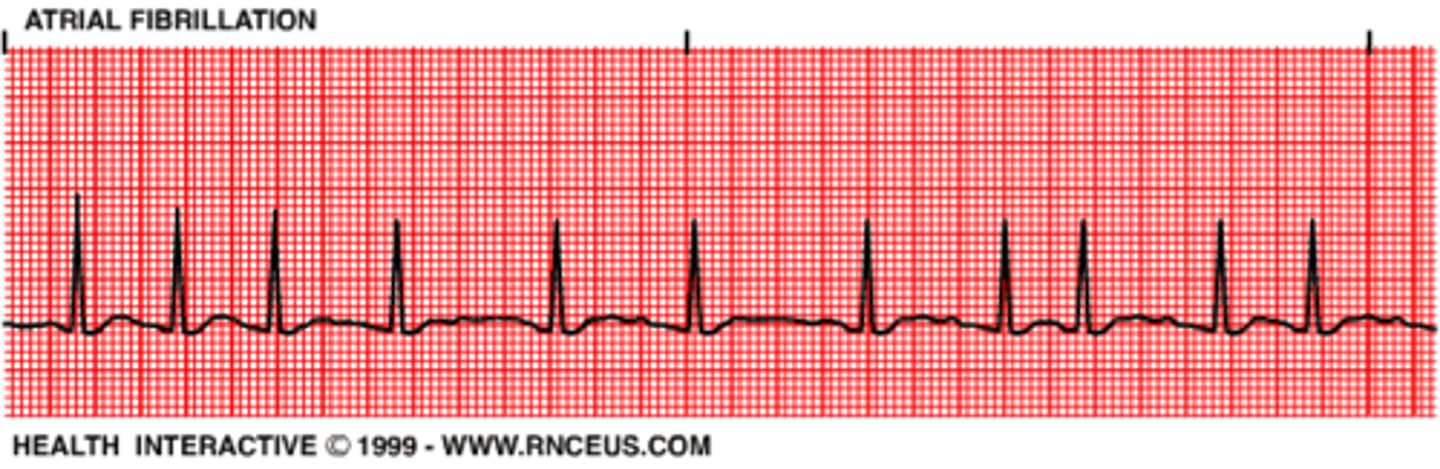
Atrial fibrillation
Atrial fibrillation produces no effective atrial contraction, causing loss of atrial kick and a 20 to 30 percent reduction in cardiac output.
It also creates a significant embolism risk because of blood pooling in the atria.
The rhythm is irregularly irregular, with no identifiable P waves and a ventricular rate that may be controlled or rapid.
Management includes rate control, rhythm control, and anticoagulation when indicated.
Junctional rhythms
Premature junctional complexes and junctional escape rhythms originate in the AV junction and may show inverted P waves before, during, or after the QRS.
Junctional escape rhythm is typically 40 to 60 bpm and may act as a protective safety rhythm if the SA node fails.
AV blocks
First-degree AV block: PR > 0.20 and constant.
Mobitz I: progressive PR lengthening until a dropped QRS.
Mobitz II: constant PR on conducted beats with intermittent dropped QRS complexes; more serious and often requires pacing.
Third-degree AV block: complete AV dissociation with poor perfusion and likely pacing requirement.
First‑degree AV block Treatment
usually asymptomatic and hemodynamically stable → monitor; adjust meds or monitor closely after MI for progression.
Second‑degree AV block Type I (Mobitz I / Wenckebach) Treatment
often asymptomatic; if symptomatic and slow, treat like sinus brady (e.g., atropine, temporary pacing if needed).
Second‑degree AV block Type II (Mobitz II) Treatment
unstable patients require immediate temporary pacing; atropine may be considered while waiting but should not delay pacing; anticipate permanent pacemaker and specialist consult.
Third‑degree AV block (complete heart block) Treatment
temporary pacing (transcutaneous then transvenous) and evaluation for permanent pacemaker after reversible causes addressed.
PVCs and ventricular dysrhythmias
Isolated PVCs may be relatively benign, but multiple PVCs in a row can deteriorate into VTach.
Electrolyte evaluation, especially potassium and magnesium, is important when PVCs increase.
Torsades de pointes
The instructor described torsades as a twisting ventricular rhythm related to prolonged QT and taught magnesium as the key treatment, often 1 to 2 grams IV.
Ventricular tachycardia and ventricular fibrillation
Pulseless VT and VF are shockable rhythms that require immediate defibrillation and CPR.
VT with a pulse may require synchronized cardioversion if unstable.
Persistent VF/pulseless VT management includes epinephrine and amiodarone in ACLS.
Asystole and PEA
Asystole is a non-shockable rhythm with no effective electrical or mechanical cardiac activity.
PEA is organized electrical activity without a pulse because mechanical contraction is absent or inadequate.
Both are treated with high-quality CPR, epinephrine, and aggressive search for reversible causes, not defibrillation unless rhythm becomes shockable.
Warfarin safety in atrial fibrillation
The reading highlighted warfarin as a high-alert medication requiring standardized dosing, close INR monitoring, and patient education regarding interactions and bleeding risk.
Ventricular fibrillation (VF) Treatment
Immediate CPR with minimal interruptions while accessing defibrillator/AED.
One shock as soon as possible, then resume CPR immediately for 5 cycles.
If VF/pulseless VT persists:
-Repeat shock, continue CPR.
-Give epinephrine 1 mg IV/IO q 3–5 min during CPR; do not stop compressions just to give meds.
-Consider antiarrhythmic (amiodarone first‑line, then lidocaine) after 2–3 shocks + epi.
Ventricular asystole (“cardiac standstill”) Treatment
Immediate CPR with minimal interruptions.
Asystole is non‑shockable – defibrillation does not help.
Give epinephrine 1 mg IV/IO q 3–5 min; recheck rhythm after about 5 cycles of CPR.
If rhythm converts to shockable (VF/pulseless VT) → follow VF protocol; if organized with pulse → post‑resuscitation care.
If persistent asystole despite efforts, consider family presence and termination of resuscitation.
Pulseless electrical activity (PEA) Treatment
follows asystole/PEA ACLS algorithm:
CPR with minimal interruptions, epinephrine 1 mg IV/IO q 3–5 min, no shocks unless rhythm becomes VF/pulseless VT.
Actively search and treat H’s and T’s (e.g., fluids for hypovolemia, needle decompression for tension pneumothorax, pericardiocentesis for tamponade, etc.).