Intro to urinary system medicine & clinical approach
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Recall the functions of the kidney
Excretion of waste —> azotaemia
Control of body fluid balance (vol and composition)
Electrolytes
Acid-base
Blood pressure
Endocrine organ
Renin
Erythropoietin (EPO)
1,25-dihydroxyvitamin D (calcitriol)
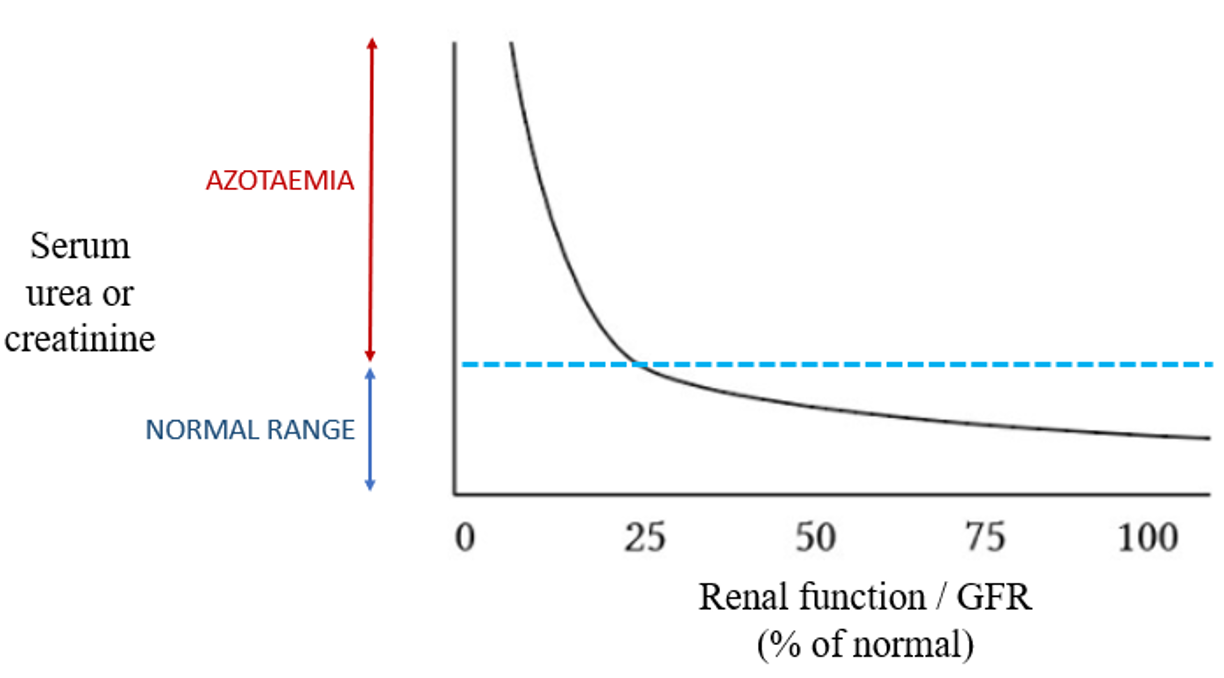
Define azotaemia and recall the types
Azotaemia = increase urea and creatinine
Pre-renal azotaemia —> decreased GFR due to decreased renal perfusion
Dehydration, hypovolaemia, heart failure
Renal azotaemia (Acute or chronic) —> renal parenchymal disease
When enough nephrons aren't functional
Post renal azotaemia —> interference with urine excretion
Urethral obstruction, UT rupture
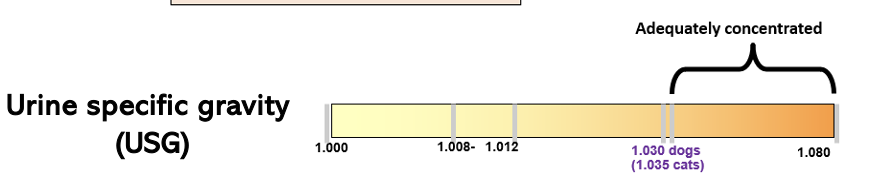
What concentrations of urine are expected in pre-renal and renal azotaemia?
Pre-renal —> Concentrated urine (USG: >1.030)
Renal —> Dilute urine (USG: 1.008-1.029)
Define CKD
Structural or functional abnormalities of one or both kidneys that have been there for 3 months or longer i.e. presence of kidney damage or reduced kidney function
(irreversible dx)
Define AKI, what can cause it?
Rapid loss of kidney function (varied from mild to severe e.g. leptospirosis, ethylene glycol, NSAID toxicity
Describe the pathogenesis of AKI
Results in abnormal GFR, tubular function and urine production
A sudden inability to maintain fluid, acid-base and electrolyte balance
May result in azotaemia
What are the most common consequences of reduced kidney function?
PUPD —> increased filtered load per surviving nephron, disruption of normal countercurrent system, impaired response to ADH
Anorexia —> can result from oral pain
Anaemia —> EPO deficiency)
Retinopathy → blindness
What is the difference between azotaemia and uraemia?
Azotaemia —> abnormal conc. of urea, creatinine and other nitrogenous compounds (LAB CHANGE)
Uraemia —> clinical syndrome that results from loss of kindey function, clinical signs (CLINICAL PICTURE)
What are the "target organs" affected by high blood pressure?
Kidney
Heart
CNS (brain)
Eyes/Retina
Which acid/base disturbance is most common in CKD?
Metabolic acidosis
(inability to excrete acid)
What may an owner report in history taking when the animal has kidney disease
Drinking and urination changes
PUPD, Pollarkiuria (increased frquency|), Stanguria (strain) , Dysuria (diffulcty passing urine)
Haematuria
Throughout urination without pollakuria, stranguria (upper UT)
Associated with pollakiuria, stranguria if bladder problem
Bleeding between urinations probably urethral/prostatic/genital tract
What value defines polydipsia?
If more than 100ml/kg/day
Define:
Pollakiuria
Stranguria
Pollakiuria —> increased frequency
Stranguria —> straining
What must be distinguished from PUPD during history taking?
Urinary incontinence
Cystitis
Submissive urination
Marking behaviour
What are the recommended core tests for kidney disease?
Haematology
Biochemistry
Urinalysis
+/- urine culture
What haemotology results may you expect in kidney disease?
Raised WBC —> inflm such as pyelonephritis
Ht, Hb, RBC: Normocytic, normochromic non regen anemia can occur
What biochem results would you expect in kidney disease?
Urea, creatinine increase
Increase phosphorus
What extent of damage does renal azotaemia imply?
Loss of at least 75% of functioning nephron
NB modest increase can represent significant damage
How do urea and creatinine differ as markers?
Urea
Made in liver from ammonia from catabolised proteins
Correlates well to kidney size
Urea can be affected by diet
Creatinine
More accurate
Produced in muscle in constant process, can be affected by muscle mass
Correlated well to GFR
Other than urea and creatinine what markers should be looked at in biochem results for suspected kidney disease
Albumin
decrease in PLN (protein losing nephropathy)
also important in Ca interpretation
Potassium
Phosphorus
Excreted by the kidneys
Hence iP increases when GFR reduced
Calcium
Total Ca may be low, normal or high in renal disease
Hypercalcaemia can cause kidney damage
SMDA
How can you perform urinalysis?
Free catch midstream (non-sterile)
Cystocentesis (sterile)
Catheterisation (not sterile, transfer of bacteria from LUT)
What gross examination points should you look at in a urine sample?
Colour
pale yellow to amber = normal
Red to brown = haematuria or haemoglobinuria
Dark yellow / brown = bilirubinuria
Turbidity
normal urine is clear
cloudy with increased cells, crystals, bacteria, mucus, lipids, casts, sperm
What bilirubin values would you expect on a dipstick? When does it increase?
Small amount = normal in dog
Always abnormal in cat
Increased in hepatic disease / haemolysis
When would blood/Hb be positive on dipstick and what should you do in positive reaction?
Positive if blood, Hb or Mb present
Centrifuge to see if RBC settle out
Will in case of RBC, wont with haemoglobinuria
Which values of a dipstick should be ignored?
Leukocytes
Nitrites
USG
What is the most accurate quantification of proteinuria?
Urine protein to creatinine ratio (UPCR)
more accurate than dipstick
Adequately concentrated USG in dogs and cats?
Dog- 1.030 or higher
Cat- 1.035 or higher
What is isosthenuria? What USG values reflects this?
Same specific gravity as plasma
May be normal if drinks a lot of water
Definitely abnormal if dehydrated
1.008-1.012
Rule of thumb:
Inadequate conc + azotaemia = renal azotaemia
What does a moderately/sub-optimally concentrated USG suggest?
Grey area
May be normal if patient is hydrated
Is abnormal in dehydration
If azotaemia present suggests renal azotaemia
What is hyposthenuria?
Lower Specific Gravity than Plasma
Requires functioning nephrons = clinically useful
Typically ADH problems
Maybe problem is drinks lots of water
Definitely abnormal in dehydration
What crystals are these?

Struvite
What crystals are these
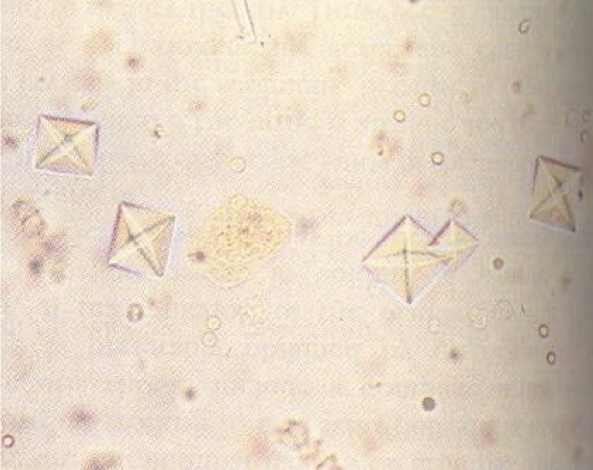
Calcium oxalate dihydrate
By how much does GFR need to reduce before serum creatinine becomes abnormal?
75%
Define dysuria
Difficulty passing urine
vs anuria = no outflow of urine