bild 2 midterm 2
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
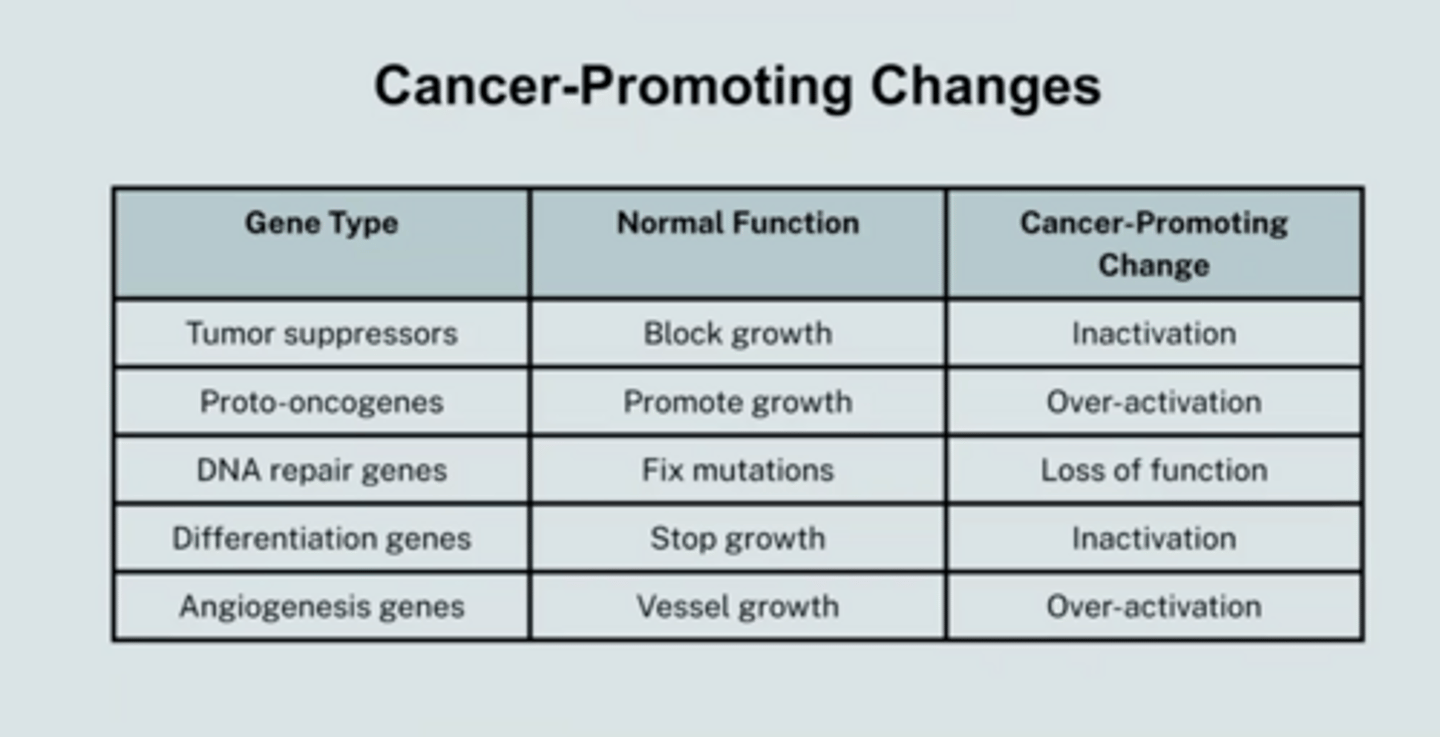
tumor suppressors:
Normally repress growth, so when inactivated will promote cancer.
proto-oncogenes
Normally encourage growth, so when over-activated (or inappropriately activated) will promote cancer.
genes that promote differentiation
Normally turned on
to promote differentiation and turn off growth, so with
inactivated will promote growth and spread of cancer.
dna repair genes
Normally fix errors in DNA, so when inactivated will promote mutations and therefore cancer.
genes that promote angiogenesis:
Normally promote
growth of blood vessels, so when over-activated or
inappropriately activated will promote tumor growth and spread of cancer.
depolarization
membrane potential gets more positive (less negative)
hyperpolarization
membrane potential gets more negative (less positive
oncogene
promotes cell growth and division (stuck accelerator)
over-activation of proto-oncogene
more cancer
inactivating, inhibiting or suppressing tumor suppressor
more cancer
inactivating, inhibiting, or suppressing oncogene
less cancer
promoting tumor suppressor
less cancer
tumor suppressor
suppress cancer (brake) -> promote apoptosis
apoptosis
cell death, repair DN, slow down cell division
cancer
uncontrollable growth (cell division) of body cells -> form a mass (tumor); arises from mutations in genes -> multiple mutations accumulated
promotes cancer
- more cell division = more chance for mutation
- more undifferentiated cells = more division so more mutation
- impaired or defective DNA repair mechanisms = more chance for mutation
- more growth signaling
- more blood vessels (angiogenesis) = for tumor growth
- more capaable of metastasis
why do fully differentiated cells not promote cancer
because they undergo less cell division -> so there is less of a chance for mutation
angiogenesis
more blood vessels = allows for tumor growth.as tumor grows larger, its volume increases faster than surface area = > low surface area/volume ratio => less nutrients exchange, tumor cannot grow more 1-2mm => need blood vessels
metastasis
spread of cancer cells from primary tissue to distant organs through blood
cancer promoting changes chart
know gene type, normal funciton, cancer-promoting change
chemotherapy
systemic drug treatment that kills rapidly dividing cells by damaging DNA or disrupting cell division
radiation therapy
local treament that uses high-energy radiation to damage DNA and destroy cancer cells in a specific area
Immunotherapy
treatment that stimulates or modifies the immune system to recognize and attack cancer cells.
localized treatment (solid tumor, localized)
radiation, surgery (most effective)
localized treatment (blood cancer - systematic, ex: leukemia)
no radiation, no surgery
systematic treatment (solid tumor, localized)
chemotherapy, immunotherapy (yes, but depends)
systematic treatment (blood cancer - systematic, ex: leukemia)
chemotherapy (most effective), immunotherapy
rapid proliferation
rapid increase, spread, or multiplication of something, often referring to a high rate of growth or reproduction in numbers
Why does cancer and embryonic development share these characteristics of rapid proliferation, ability to migrate, and reduced sprecialization.
both cancer cells and embryonic cells activate gentic programs that promote cell division, migration, and reduced differentiation.
endocrine system (hormones, chemical messengers) - long distance communication within the mammalian body (nervous system)
- gland releases hormone into bloodstream
- hormone circulates everywhere
- ONLY cells with the right receptor respond
- slow duration
- long-lasting effects
- broad targets (cells throughout body)
nervous system (neurons) - long distance communication within the mammalian body (nervous system)
- electrical signal travels down a neuron (action potential)
- chemical signal crosses synapse (neurotransmitter)
- signal reaches a specific target cell
- extremely fast (milliseconds
- short-lived effects
- precise target (muscles, neurons, and glands)
neurotransmitter
chemical signal crosses a synapse
nervous system
electrical impulses are the messengers in the nervous system
endocrine system
Hormones are the chemical messengers in the endocrine system that target cells through the bloodstream
parts of the nervous system
brain, spinal cord, peripheral nervous system, ganglion, nerve
parts of the endocrine system
Pituitary gland,
Pineal gland,
Thyroid gland,
Thymus,
Adrenal glands,
Pancreas, ovary (female), testis (male)
neurons
- electrical signaling
- generate action potentials
- carry information
- communicaton
glia
do everything neurons don't
- support and protection
- do not fire action potentials
astrocyte function
Deliver nutrients from blood to neurons Maintain ion balance (K+, Na+) Help repair damage
astrocyte location
CNS
microglia function
destroy pathogens, clean cellular debris
microglia location
CNS
oligodendrocytes function
Wrap axons in myelin One cell → wraps many axons
oligodendrocytes location
CNS
schwann cells location
Wrap axons in myelin One cell → one axon
schwann cells location
PNS
central nervous system
- brain and spinal cord
- decision making
- integration system
peripheral nervous system
- all nerves outside of the CNS
- sends info TO and FROM CNS
dendrites
receive signals
soma
integrates signals
axon
transmits signal
axon terminals
release neurotransmitter
nucleus
gene expression (not signaling)
information flow through a neuron
dendrites > soma > axon > axon terminals
what happens when Na+ channels are blocked
- You do not get a normal AP
- no sharp rising phase; at most a small subthreshold bump
what does rising phase depend on
Na+ influx
what happens when Na+ channels open less well (reduced function) ?
- harder to reach threshold
- if it fires, peak may be reduced or AP may fial to fully develop
what happens when Na+ channels fail to inactivate
- the AP stays depolarized longer (plateau-ish)
- repolarization is delayed
- neuron may be prone to repeated firing/seizures
repolarization
the biological process where excitable cells (neurons or muscle) restore their negative internal charge after depolarization. It is a critical "reset" phase of the action potential—often described as cellular relaxation or recharging—where sodium channels close and potassium channels open, allowing positive potassium ions to leave the cell
what happens if K+ channels are blocked (ex: TEA)
- falling phase is slower
- repolarization delayed
- undershoot reduced or missing
- AP is "wider" = takes longer to return to rest
- key: AP propagation can still occur because propagation depends on Na+ driven depolarization to trigger the next segment
what happens when K+ channels open more easily/earlier
- faster repolarization
- bigger undershoot (more hyperpolarization)
- peak might be cut short (because K+ "fights" Na+ sooner)
how lack of myelination would affect the propagation of the action potential
- AP regenerated at every patch of membrane
- slower conduction
- more ion dissipate
how myelination would affect the propagation of the action potential
- AP "jumps" between nodes = saltatory conduction
- faster, energy-efficient
what is the shape of AP when myelinated or not
- AP shape is identical from unmeyelinated and myelinated, only arrival time changes.
how does AP change when demyelinated
becomes slower, less efficient, or fails
neurotransmitter release
- controlled by Ca2+ entry and vesicle fusion
- more release . more receptors activted . stronger signaling
- less release . weaker signaling
whether receptors can respond
- nt only works if receptors are present and functional
- blocked or absent receptors = no signaling, even with normal release
- more receptors or higher sensitivity = stronger response
length nt stays in synapse
- clearance (reuptake, degradation, diffusion), ends the signal
- slower clearance = longer, stronger signaling
- faster clearance = shorter, weaker signaling
if nt release increases
- predictions: more nt in the synaptic cleft, more receptors bind nt, stronger postsynaptic response, greater chance the postsynaptic cell reaches threshold and fires an AP
if nt release decreases
- predictions: less nt available to bind receptors, weaker postynaptic response, postsynaptic neuron less likely to reach threshold
no matter how healthy the postsynaptic cell is, less NT = ....
less signaling
examples from lecture about nt signaling
- black widow spider toxin creates Ca2+ pores
- more Ca2+ enters presynaptic neuron
- more vesicle fusion > more NT relesed
↑ NT release
↑ signaling
↓ NT release
↓ signaling
↑ receptors
↑ signaling
Block receptors
↓ or no signaling
Slower clearance
↑ duration & strength of signaling
Faster clearance
↓ duration & strength of signaling
clearance
(reuptake, degradation, diffusion), ends the signal
water-soluble molecules bind....
to receptors on the cell membrane
lipid-soluable molecules bind....
to receptors inside the cell
two mechanisms for how different target cells exposed to the same hormone can respond in different ways
1. Different target cells may have different receptors for the hormone
2. Different target cells use the same receptor but different signal transduction pathways inside the cells to turn the receptor's response into a cellular response
how do different signal transduction pathways inside cells turn the receptor's response into a cellular response?
-activate certain enzymes
- release of ions like calcium
- gene expression
hypothalamus
receives information from brain and initiates reponse
pituitary
responds to hypothalamus to secrete hormones into the blood
anterior pituitary
1. hypothalamus secretes first hormone ex: GnRH
1. Hormone acts on anterior pituitary to release second homrone ex: LH, FSH
is the anterior pituitary direct or indirect?
indirect
posterior pituitary
1. hypothalamic axons project onto pituitary blood vessels and release hormone directly to the body ex: ADH, oxytocin
is the posterior pituitary direct or indirect?
direct
If hypothalamus is overactivated, how does that affect the eventual release of Thyroid-Stimulating Hormone (TSH)?
High TRH > High TSH release > high thyroid release > more inhibition on hypothalamus and more inhibition of anterior pituitary > less TSH is made
what does the thyroid hormone contain nd require?
iodine
If someone has low CRH levels, does that mean there is definitely something wrong with their hypothalamus?
No. This can also be because of high cortisol levels