Motor Behavior Quiz 2 Ch. 4-6
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
biomechanical approaches to managing hypertonicity focus on
altering muscle length through prolonged stretching
Casts, splints, and orthoses are used to
manage hypertonia, maintain or increase PROM, improve function in patients with neural pathology
Patient positioning is biomechanically used for what
improve muscle length
hierarchy of sensory function
low → high
detection → discrimination → quantification → cortical sensation
detection → single pt stimulus
discrimination → btw 2 stimuli
quantification → organize tactile stimuli according to degree (roughness/wt)
cortical sensation → graphesthesia, stereognosis (recognize car in hand)
UE flexion synergy presentation
scapular retraction & elevation
shoulder abd & ER
elbow flex
forearm sup
finger & wrist flex
LE extensor synergy
hip ext, add & IR
knee ext
ankle PF & inversion
toe PF
Potential lesion locations if explicit learning is impaired
medial temporal lobe areas, sensory association cortex, hippocampus
Potential lesion location if nonassociative learning is impaired
reflex pathways
Potential lesion location if associative learning is impaired
amygdala, cerebellum, deep cerebellar nuclei, premotor cortex
Potential lesion location if procedural learning is impaired
striatum and other motor areas
Diaschisis
transient CNS disorder in which a part of the brain that is structurally intact loses function because of a loss of inputs from an anatomically connected area of the brain that is injured
The sudden functional depression of brain regions distant from the primary site of injury can be due to
a reduction in blood flow and/or metabolism
Early recovery of function following stroke is due to
the resolution of diaschisis
Cerebral edema
space-occupying lesion that can cause an increase in intracranial pressure
Recovery of synaptic effectiveness and nerve conduction is due to
resolution of edema
Long term sensitization results in
Increased number of synaptic connections
Sensitization mechanisms
Prolonged actional potentials that increase the EPSP
Example of habituation
Decreasing sensitization to dizziness during head movements in patients with inner ear disorders
Short-term habituation results in
No structural changes, just a decrease in EPSP amplitude at the synapse
Long-term habituation results in
Decreased number of synaptic connections and active transmitting zones within the existing synaptic connections
hyperkinetic disorders
Athetoid CP, Huntington’s Disease, Hemiballismus
Hypokinetic disorders
Parkinson’s
hyperkinetic disorders characterized by
excessive and involuntary movements and hypotonia
Athetosis/athetoid movement
slow involuntary writhing and twisting movements
Which extremity is affected more with athetosis
upper extremity
Athetosis can also affect
the face, neck, and tongue
Primary cause of athetosis
Athetoid CP
hyperkinetic disorder characteristics
excessive and involuntary movements and hypotonia
Chorea/choreiform movements
involuntary, rapid, irregular, and jerky movement
Primary cause of choreiform movements
Side effect of antiparkinsonian medications
Primary cause of dystonia
Basal ganglia disorders
Dystonia characteristics
co-contraction of agonist and antagonist muscles
What is dystonia initiated/worsened by?
voluntary action
Dystonia is associated with
overflow muscle activation
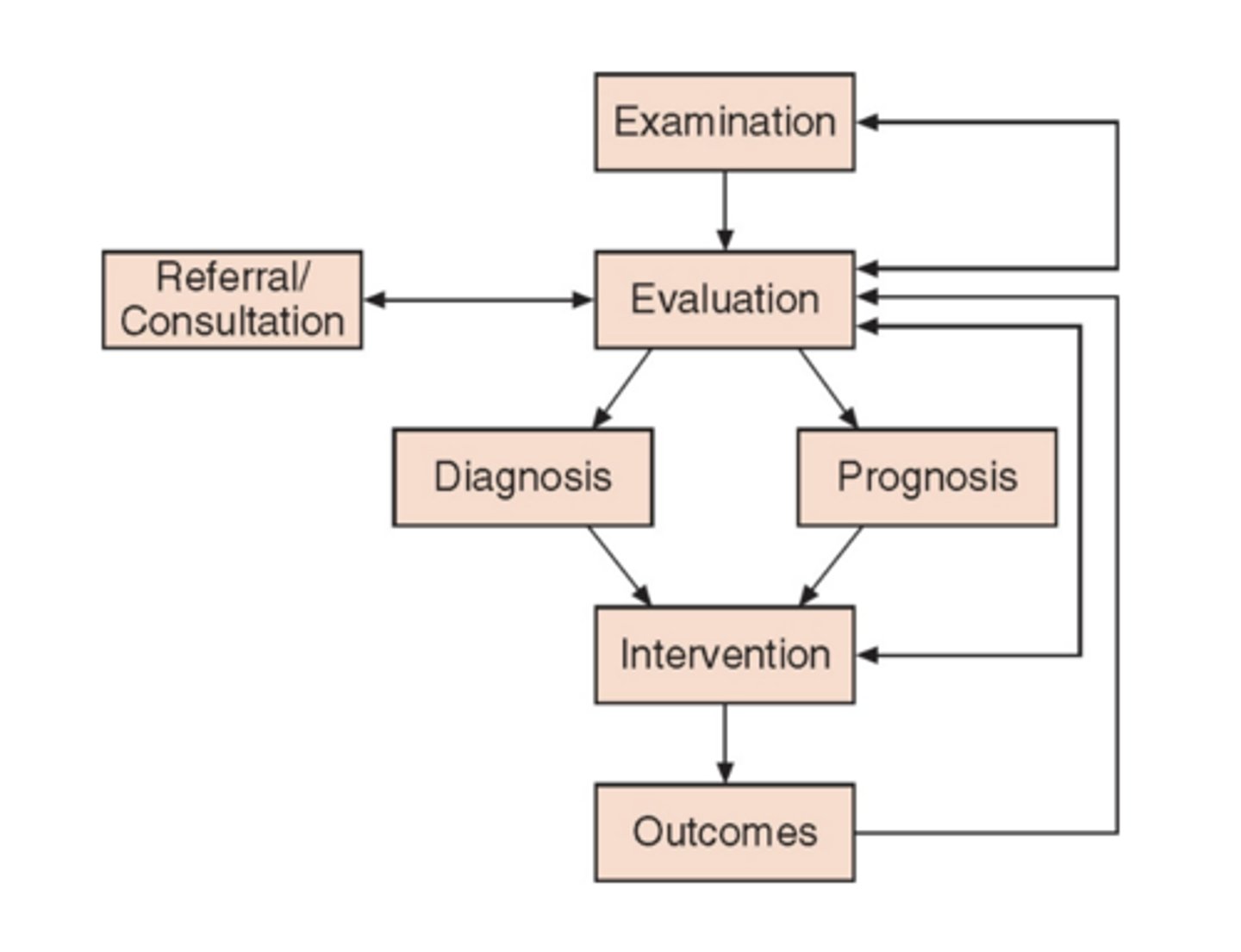
APTA model of practice
exam → history, review of systems, test & measures, data collection to form diagnosis, prognosis, POC
evaluation → clinical reasoning based on data from exam
prognosis, diagnosis → intervention
plan of care
Principle 1 of neuroplasticity
Use it or lose it
Use it or lose it
Failure to drive specific brain functions can lead to functional degradation
Principle 2 of neuroplasticity
Use it and improve it
Use it and improve it
Training that drives a specific brain function can lead to an enhancement of that function
Principle 3 of neuroplasticity
Specificity
Specificity
The nature of the training experience dictates the nature of the plasticity
Principle 4 of neuroplasticity
Repetition matters
Repetition matters
induction of plasticity requires sufficient repetition
Principle 5 of neuroplasticity
intensity matters
Intensity matters
induction of plasticity requires sufficient training intensity
Principle 6 of neuroplasticity
time matters
Time matters
different forms of plasticity occur at different times during training
Principle 7 of neuroplasticity
salience matters
Salience matters
the training experience must be sufficiently salient to induce plasticity
Principle 8 of neuroplasticity
Age matters
Age matters
training-induced plasticity occurs more readily in younger brains
Principle 9 of neuroplasticity
transference
Transference
plasticity in response to one training experience can enhance the acquisition of similar behaviors
Principle 10 of neuroplasticity
interference
Interference
plasticity in response to one experience can interfere with the acquisition of other behaviors
finger to nose nonequilibrium test of coordination
The shoulder is abducted to 90 degrees with the elbow extended. The patient is asked to bring the tip of the index finger to the tip of the nose.
finger to therapist’s nonequilibrium test of coordination
The patient and therapist sit opposite each other. The therapist’s index finger is held in front of finger of the patient. The patient is asked to touch the tip of the index finger to the therapist’s index finger.
finger to finger nonequilibrium test of coordination
Both shoulders are abducted to 90 degrees with the elbows extended. The patient is asked to bring both hands toward the midline and approximate the index fingers from opposing hands.
Alternate nose to finger nonequilibrium test of coordination
The patient alternately touches the tip of the nose and the tip of the therapist’s finger with the index finger.
Finger opposition non equilibrium test of coordination
The patient touches the tip of the thumb to the tip of each finger in sequence. Speed may be gradually increased.
Mass grasp nonequilibrium test of coordination
An alternation is made between opening and closing fist. Speed may be gradually increased
Pronation/supination nonequilibrium test of coordination
With elbows flexed to 90 degrees and held close to the body, the patient alternately turns the palms up and down. This test also may be performed with shoulders flexed to 90 degrees and elbows extended. Speed may be gradually increased.
Rebound test nonequilibrium test of coordination
The patient is positioned with the elbow flexed. The therapist applies sufficient manual resistance to produce an isometric contraction of biceps. Resistance is suddenly released. Normally, the opposing muscle group with contract and check movement of the limb.
Tapping hand nonequilibirum test of coordination
With the elbow flexed and forearm pronated, the patient is asked to tap the hand on the knee.
Tapping foot nonequilibrium test of coordination
The patient is asked to tap the ball of one foot on the floor without raising the knee; the heel maintains contact with the floor.
Pointing and past pointing nonequilibirum test of coordination
The patient and therapist are opposite each other, either sitting or standing. Both patient and therapist bring shoulders to a horizontal position of 90 degrees of flexion with elbow extended. Index fingers are touching or the patient’s finger may rest lightly on the therapist’s. The patient is asked to full flex the shoulder and then return to the horizontal position such that index fingers will again approximate. Both arms should be tested, either separately or simultaneously. A normal response consists of an accurate return to the starting position.
alternate heel to knee; heel to toe nonequilibrium test of coordination
from a supine position, the patient is asked to touch the knee and big toe alternately with the heel of the opposite extremity
toe to examiner’s finger nonequilibrium test of coordination
from a supine position, the patient is instructed to touch the great toe to the examiner’s finger.
heel on shin nonequilibrium test of coordination
from a supine position, the heel of one foot is slid up and down the shin of the opposite lower extremity
drawing a circle nonequilibrium test of coordination
The patient draws an imaginary circle in the air with either upper or lower extremity.
Fixation or position holding nonequilibrium test of coordination
upper extremity: the patient holds arms horizontally in front.
lower extremity: the patient is asked to hold the knee in an extended position
____________ feedback facilitates learning better than ________ feedback
intermittent; constant