Endocrine diagnostics and histology
1/173
Earn XP
Description and Tags
In this hyperadrenocorticism = HAC, hypoadrenocoritism will be stated as HypoAC. Also includes steroid lecutre W3.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
174 Terms
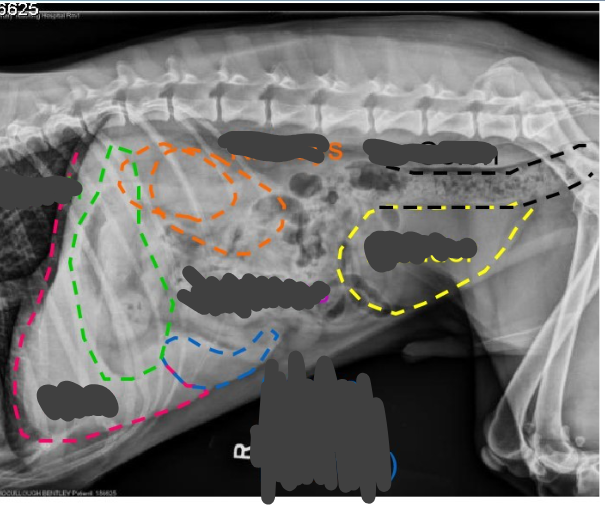
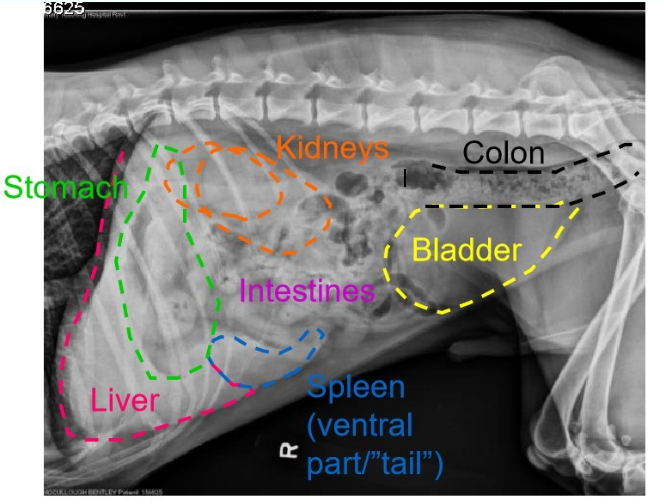
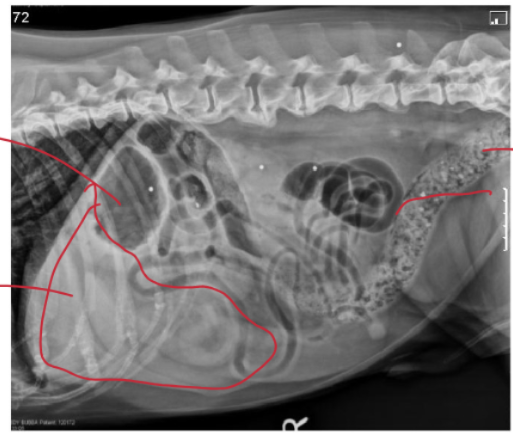
Identify the anatomy on this normal lateral radiograph
Green = stomach
Pink = liver
Orange = kidneys
Blue = spleen (ventral part)
Black = colon
Yellow = bladder
Middle = intestines
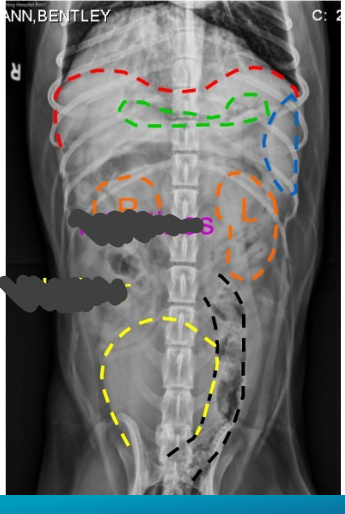
What view radiograph is this, identify the normal anatomy
ventrodorsal
red = liver
green = stomach
blue = spleen
orange = kidneys
black = colon
yellow = bladder
middle = intestines
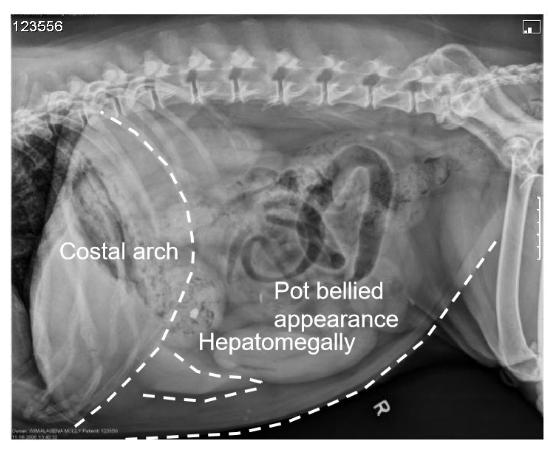
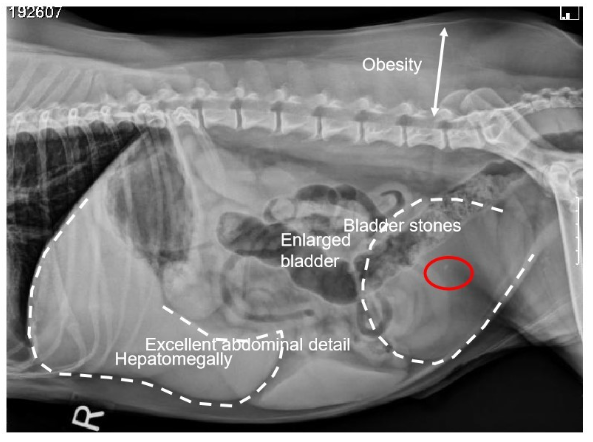
Identify 10 features that signal to abnormal adrenals (HAC)
obesity
pot belly
hepatomegally - extends beyond the costal arch
± adrenal mass
large bladder
± cystoliths
dystophic mineralisation of soft tissues e.g. calcinosis cutis adrenal gland and/or kidney
ossteopenia (thinning bones)
excellent contrast b/w intraabdominal fat
What is an identifying feature of pituitary-dependent HAC
hepatomegaly
What is a defining feature of hyperadrenocorticism
contrast provided by intraabdominal fat
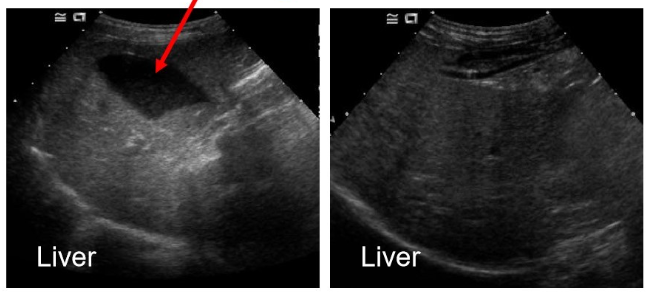
What is this structure?
gall bladder
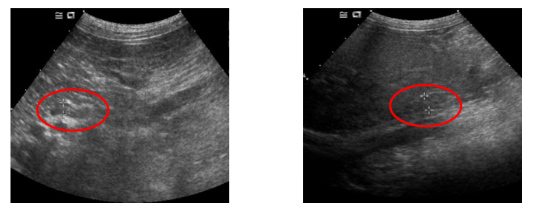
What is this structure?
adrenal gland
What is the average width of adrenal glands with dogs who have pituitary-dependent HAC?
8.6mm
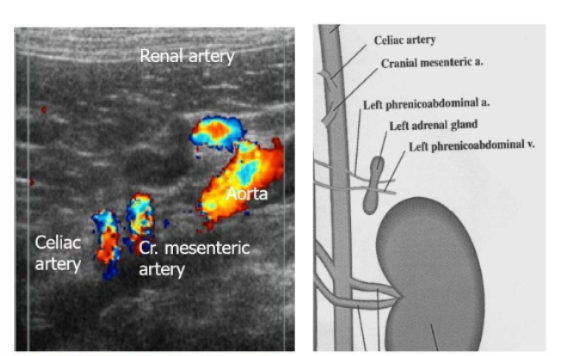
What are the blood vessel supply to the left adrenal?
left phrenicoabdominal artery
left phrenicoabdominal vein
aorta with the cranial mesentaric artery and celiac artery branching off cranial to the adrenals
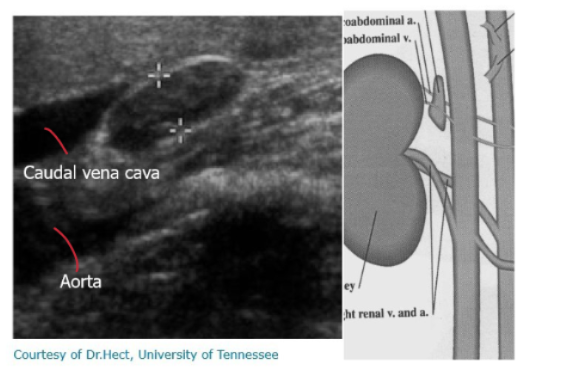
What is the blood supply to the right adrenal?
phrenicoabdominal vein and artery
caudal vena cava
aorta also present
What are the abnormalities on this radiograph, what does it signal to?
‘‘mass effect’’, deviating colon, enlarged liver, stark contrast of organs due to fat
adrenal dependent HAC

What is the ‘‘mass effect’’ abnormality on this radiograph, what condition does it signal to? (dog)
deviating small intestine
adrenal dependent HAC
What are the anatomical landmarks used to localise the left and right adrenal gland?
celiac and cranial mesenteric arteries (left gland caudal, right gland cranial)
cranial to renal artery
phrenicoabdominal cein crosses mid portion of adrenal gland
aorta (left), caudal vena cava (right)
What should the size of a normal adrenal gland be (dog and cat)?
Dog varies with patient body weight - looking at the caudal pole of the adrenal gland
Left gland: 5.1 - 7.3 millimetres (smaller dog = smaller size vice versa)
right: 5.3-8.7mm
Cats
2-5mm
Should be taken into consideration with other clinical findings and view of measurement on the ultrasound
What changes in the adrenal size and shape would we expect with:
pituitary-dependent HAC
benign adrenal-dependent HAC?malignant adrenal-dependent HAC?
both pituitary and adrenal dependent HAC?
bilaterally enalrged
unilaterally enlarged
unilateral adrenal enlargement, potential atrophy of the other adrenal
adrenal asymmetry without it being as extreme (very rare and difficult to diagnose)
In addition to hyperadrenocorticism, what other pathological processes can cause adrenomeglay?
chronic stress
chronic stress on non-adrenal illness
phaeochromocytoma
non-cortisol secreting adrenocortical tumours
rare things like metastatic tumours, tuberculosis or other granulomatous lesions, congenital adrenal hyperplasia.
For obese cats:
what is the ideal body score for a cat
what are the two types of body condition scores
why is it relevant to know which type we’re using
why is it an advantage to use BCS rather than simply weight??
5/9 - 44-55% body fat (each level is around 5% body weight0
body and muscle condition scores
an animal may have lots of fat storage but no muscle
looks at composition rather than mass (see point above), but it is subjective (weight is objective and comparable). should take both in every clinical scenario.
Obesity can be detrimental to many different body systems. Which systems are at risk and what are possible consequences of obesity to these body systems.
heart, CVS
liver
increased pressure on joints
increased inflammatory markers
endocrine - stored cells with fat → hormone synthesis and storage is limited/suppressed.
What are the physiological principles behind weight gain in the following endocrine diseases?
hyperadrenocorticism
hypothyroidism
acromegaly
more glucose → more insulin → more storage
decreased T3/T4 → decreased metabolic rate → less food needed → starvation response → storage
increased growth hormone
Outline how a glucose-intolerance test is take
Prep: fast the cat for 12 hours
take a blood sample - 0.5ml into FOx
either via IV (500mg/kg) or orally (2g/kg), give the glucose solution
take samples into FOx tubes after 5, 10, 15, 30, 45 nd 60 minutes
send to a lab
observe results
In a glucose-tolerance test what would we expect for:
normal cat
plasma glucose initially rises and falls off, to return to normal values within 2-3 hours
half life of glucose = 16-38 minutes
In a glucose-tolerance test what would we expect for:
diabetic cat
reduced first phase of insulin secretion, followed by a delayed, exaggerated insulin response
In a glucose-tolerance test what would we expect for:
glucose intolerance
what may this be caused by?
second phase of insulin secretion is lost → glucose levels stay higher longer
diabetes mellitus, phaeochromocytoma, hyperadrenocorticism
In a glucose-tolerance test what would we expect for:
islet cell functional tumour
lower maximum plasma glucose levels and more rapid return to pre-glucose levels
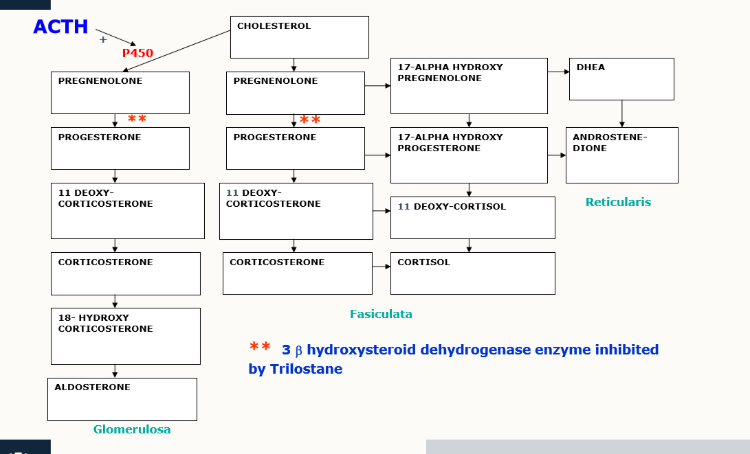
What do all steroid hormones begin as?
cholesterol
What is the pathway of steroid hormone production
cholesterol → pregnenolone
What is cholesterol conversion into pregnenolone limited by?
ACTH
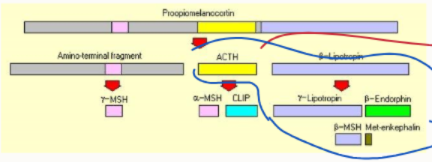
What is ACTH synthesised from?
POMC
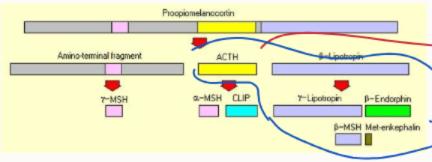
How does HAC differ between horses and dogs?
dogs is caused by an excess of HAC
horses - caused by the zona intermedia in the pituitary gland → more hormones involved (blue circle)
Outline the physiology of glucocorticoids
how are they transported in blood
how do they signal at their target cell
90% bound to plasma proteins
bind to specific cell membrane/cytosolic receptor at target → transported to the nucleus → altered gene expression
What are 4 actions of glucocorticoids
stimulates gluconeogenesis
stimulates glycogenolysis
causes proteolysis
promotes lipolysis
Outline the effect of glucocorticoids on:
fat
muscle
liver
mobilisation from peripheral stores
catabolism
gluconeogenesis, antagonise insulin
Outline the effect of glucocorticoids on:
kidney
skin
bone
increased GFR, blocked ADH action
follicular atrophy, sebaceous gland atrophy
reduce calcium levels, osteopaenia
Outline the effect of glucocorticoids on:
brain
immune system
hunger and thirst
release neutrophils from their marginal pool, down-regulates immune responses (T-cell function and recruitment, B-cell activation)
What is the main stimulus for aldosterone release?
low blood pressure - RAAS
high serum K+ also stimulates release
What are the 4 most important androgens?
testosterone
dihydrotestosterone (DHT)
dehydroepiandrosterone (DHEA)
androstenedione
What is the function of androgens?
stimulate/control the development and maintenance of male characteristics by binding to androgen receptors
What are androgens the precursors for?
oestrogens
What is HAC characterised by?
excessive production of steroid hormones, especially glucocorticoids, from the adrenal cortex
Canine HAC:
1. how can is develop?
of one type, what are the two sub-types?
spontaneous or iatrogenic
PDH (90% of cases) or ADH
How does a PDH result in HAC?
excess ACTH secretion → bilateral adrenal hyperplasia
How does ADH result in HAC?
50% adenomas
50% carcinomas
independent of pituitary control - low ACTH
what is the difference in PD HAC:
microadenoma
macroadenoma
what effect do these have?
<10mm, majority of cases
>10mm, slow growing → neurological signs
normal negative feedback mechanisms fail
for AD HAC:
observation grossly of adrenal glands?
independent from…
calcification?
unilateral adrenal enlargement → atrophy of the contralateral side
ACTH control - conc low/undetectable
50% of adrenal glands will be calcified regardless of tumour type

What tends to be the signalment of AD HAC?
older dogs (11-12 years)
larger breed dogs
What tends to be the signalment for PD HAC?
middle aged dogs 7-9 years
poodles, daschunds and small terriers
What are specific clinical signs that signal HAC?
PU/PD
abdominal enlargement (Pot belly)
polyphagic (alopecia)
skin changes
hepatomegaly
muscle wasting/weakness
lethargy/exercise intolerance/panting
reproductive changes
Apart from the known clinical signs:
how do most cases present
what organs are at risk
usually insidious (‘‘just ageing’’) - signs may be intermittent
liver, muscle, bone, kidneys, immune system, reproductive system, skin, respiratory system, CVS, CNS, PNS
Outline PU/PD in HAC
PD: >100ml/kg/day dog, >50ml/kg/day cat
PU: >50ml/kg/day
PD secondary to PU
Outline abdominal enlargement seen with HAC
classic ‘‘pot-bellied’’ appearance
re-distribution of fat into adbomen
hepatic enlagement
wasting and weakness of abdominal muscles
palpation may be easier
Outline polyphagia in relation to HAC
assumed to be due to glucocorticoids
may be misinterpreted
Outline cause of muscle wasting with HAC
usually gradual
caused by protein catabolism
With hyperadrenocorticism, where will we notice muscle wasting
limbs
spine
temporal region
What skin changes may we see associated with skin changes
bilaterally symmetrical alopecia - inhibitory effects of steroids on anogen phase
thin skin and reduced elasticity - prominent abdominal veins
excessive scale and comedones
slow wound healing
with HAC why do we see:
thin skin and reduced elasticity w. prominent abdominal veins
slow wound healing?
protein catabolism (atrophic collagen) and loss of subcutaneous fat
inhibition of fibroblast proliferation and collagen synthesis

What is calcinosis cutis, wtih what endocrine disorder do we see it, where will we see it on an animal?
slightly elevated plaques surrounded by erythema
neck, axilla, ventral abdomen and inguinal areas
How can we treat HAC in the UK?
trilostane (Vetoryl) licensed treatment.
it’s a reversible inhibitor of 3-beta hydroxysteroid dehydrogenase enzyme (prevents cortisol being produced)
adrenalectomy or hypophysectomy → needs replaceent therapy for hormones
what is a US treatment method
mititane (Lysodren) - chemical ablation of adrenal cortex, medulla spared
needs hormone replacement therapy
For HAC in cats:
more/less common, why?
uncommon, cats are more resistant to the effects of glucocorticoids
What is the signalment and are the major clinical signs of HAC in felines?
middle-older age
PU/PD, polyphagia, weight loss
extreme skin fragility
pendulous abdomen
UTIs
What is the ratio of feline PD HAD: AD HAC
75-90% PD HAC
20-25% AD HAC
What can impact our results whilst testing for HAC?
chronic illness
psychological stress
What are the 4 investigations in to determining whether an animal has HAC?
blood test investigation - biochem and CBC
urinalysis
imaging
specific tests
What parameters do we measure in biochemistry for HAC? What do we expect?
ALP - in >90% cases
ALT (mild-moderate)
cholesterol
bile acids (mild-moderate)
fasting glucose
Reduced:
BUN (blood urea nitrogen)
What haematological results do we expect with CBC for HAC?
neutrophilia
lymphopenia
eosinopaenia
monocytosis
What do we expect in urinalysis for HAC?
low USG - often <1.015, can be hyposthenuric (<1.008)
evidence of UTI
What abdominal radiographic findings do we expect?
hepatomegaly
pot-bellied appearance
calcinosis cutis
distended bladder
adrenal enlargement/calcification
What thoracic radiographic findings do we expect for HAC?
tracheal and bronchial wall mineralisation
pulmonary metastasis
osteoporosis (more human)
What is the approximate normal size of an adrenal gland - ultrasound?
25mm x 5mm
What screening tests could we use for HAC?
urinary cortisol: creatinine ratio
ACTH stimulation test
low dose dezamethason suppression test (LDDS)
Outline the urinary cortisol to creatinine ratio:
ease of test?
when do we take a sample
sensitivity vs specificity?
expected ratio?
very easy
owner, in the morning
low ratio = HAC unlikely = highly sensitive
high ratio = animals could have HAC but also elevated for many others = low specificity
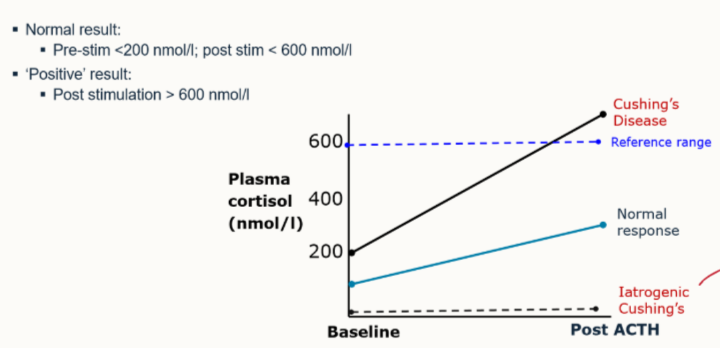
What is the protocol for ACTH stimulation test
starve overnight
test plasma cortisol at time 0
inject synthetic ACTH
test plasma cortisol 60min later
For a dog with spontaneous HAC what would we expect when performing an ACTH stimulation test
exaggerated response of cortisol increase
For the ACTH stimulation test:
easy, cheap?
sensitivity vs specificity?
quick, easy but expensive
okay sensitivity (85% PDH, >50% ADH) - don’t exclude if negative
best specificity of HAC (few false positives)
Outline the LDDS test protocol
starve overnight, measure baseline plasma cortisol, inject 0.01mg/kg dexamethasone IV
measure cortisol at 3 vs 8 hours
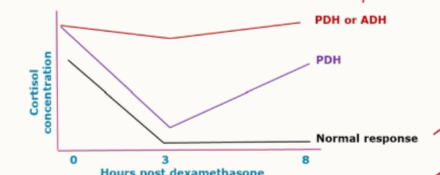
Of the LDDS test, what is a confirmatory result?
>50nmol/L at 8 hours
What is the LDDS sensitivity vs specificity
more sensitive - should detect nearly 90-95% of PDH and most ADH
lower specificity (more false positives)
If the ACTH is negative BUT we’re suspicious of disease, perform what test?
LDDS
negative - consider other diseases
positive - treat
what are the 4 tests we perform to differentiate ADH from PDH
(HDDS)
endogenous ACTH
adrenal imaging
pituitary imaging
what is the HDDS?
same protocal as for LDDS, just 0.1mg/kg dexamethasone
How does HDDS, in theory differentiate b/w AD and PD HAC
PDH: - suppression of ACTH → decreased cortisol production
ADH: suppressing ACTH has no effect → continuously high cortisol levels
why are HDDS tests no longer used?
25-30% PDH tumours → ACTH has no effect on, so act as an AD HAC = high cortisol
For the endogenous ACTH:
what happens to the levels in a functional pituitary tumour
functional adrenal tumour
is it used to diagnose ADH or PDH?
increase, they’re high
stay low - negative feedback mechanism doesn’t work
ADH, PDH can fall within normal range
In adrenal imaging:
what does PDH look like
ADH?
symmetrical enlargement and normal conformation
one enlarged gland and one atrophied gland
With adrenal dependent HAC, why is one gland atrophied?
negative feedback loop is functional in one gland, not the other.
The gland producing excessive cortisol → negative feedback mechanism which the contralateral gland responds to → not used → atrophies
What can we use for imaging the pituitary?
CT
MRI
expensive!!!
What affect do glucocorticoids have on the body? what is it controlled by?
gluconeogenesis
glycogenolysis
proteolysis
lipolysis
Controlled by ACTH
Outline aldosterone:
what does it play a central role in
where does it act
what does it cause
other than BP what can stimulate its release?
regulation of BP through RAAS
distal tubule and collecting duct
increases reabsorption of Na, Cl and hence water. Stimulates K+ release into tubular lumen.
high serum K+
How is renin release stimulated?
baroreceptors in the wall of the afferent arteriole
cells of macula densa in the distal tubule are stimulated by reduced NaCl delivery
also baroreceptors in the cardiac and arterial
what are the 3 classifications of hypoadrenocorticism
primary → addison’s disease, loss of adrenal cortex
secondary → ACTH deficiency, rare
iatrogenic hypoadrenocorticism → exogenous steroids
Primary HypoAC:
known name
what is it
what does it occur with
what are some causes in dogs
addison’s disease
deficiency of glucocorticoids and deficiency of mineralocorticoids
idiopathic atrophy: maybe immune-mediated destruction
iatrogenic
what are 2 drugs and a surgery that can result in primary hypoAC
Drugs: mitotane, trilostane
surgery: bilateral adrenalectomy
outline iatrogenic hypoAC:
cause
what may symptoms appear as?
how should we always remove steroids?
exogenous steroids → adrenal atrophy. affects cortisol only
signs of Cushing’s syndrome
taper off, suddenly remove → animal can crash
Outline the signalment of Addison’s
young-middle aged dogs
certain breed dispositions
extremely rare in cats
Give 3 dog breeds predisoposed to addison’s
standard poodles
bearded collies
portugese water dog
leonberger
great dane
rottweiler
WHWT
soft coated wheaten terrier
Outline pathophysiology
aldosterone deficiency → loss of Na+, Cl-, H20, K+, H+ retention, pre-renal renal failure due hypovolaemia
glucocorticoid deficiency → decreased stress tolerance, GI signs, weakness, appetite loss, anaemis, impaired gluconeogenesis
what is addisionian crisis?
acute HypoAC
marked hypovolaemia with azotaemia
Outline the signalment of chronic HypoAC
vauge and non-specific signs - wax and wane with treatment and stress
anorexia, vomiting, diarrhoea, PU/PD, weakness, lethargy and depression
appear normal b/w bouts, especially after some fluid therapy/steroid but RELAPSE
Outline the clinical signs of acute HypoAC
history of V+/D+
signs caused by hypovolaemic shock
usually collapsed/v weak
paradox of relative bradycardia
some abdominal pain (seems like pancreatitis)
why do we get bradycardia with acute Addisonian shock?
hyperkalaemia