asynch lect: cracked teeth and VRF
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
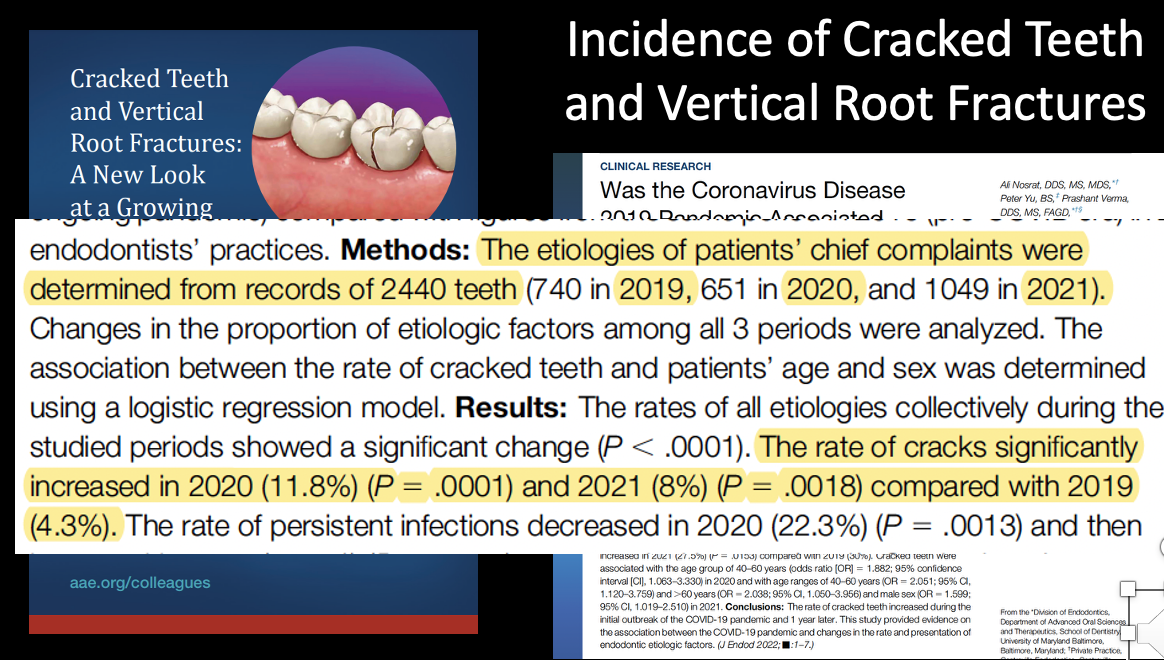
trend of cracked teeth
increasing
abfraction
v-shaped loss of hard tooth structure cause by biomechanical loading forces from flexure and/or chemical degradation of enamel and/or dentin at same location distance from the actual point of laoding

infraction is also referred to as
craze line
infraction
a crack of the enamel without loss of tooth structure


are infractions commonly encountered
yes
cracked tooth
a thin surface disruption of enamel and dentin, and possibly cementum , of unknown depth or extension

fracture
a spilt of break in bone, cartilage, or tooth structure.
fracture in tooth structure
disruption of the enamel and/or dentin and/or cementum that is assumed to be of greater depth than a crack
of unknown depth or extension
visible or not
is visible clinically or radiographically
separated or unseparated segments

root fracture
a fx that exists or extends into the root; to include dentin, cementum, and possible pulpal space, which may progress to or from enamel
2 types of longitudinal fractures
vertical root fracture
split root
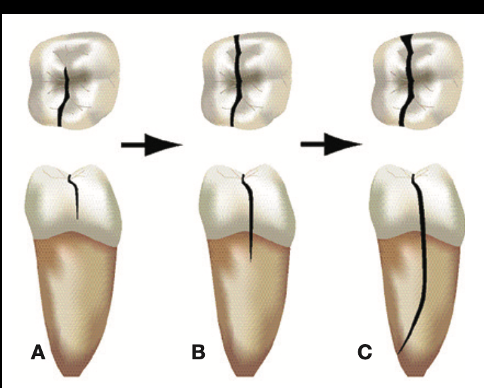
vertical root fracture
fx in root whereby the fx segments are incompletely separated; may/may not occur BL or MD

vertical root fx may cause __________ or __________
isolated periodontal defects; sinus tract
t or f: vertical root fx may be radiographically evident
t
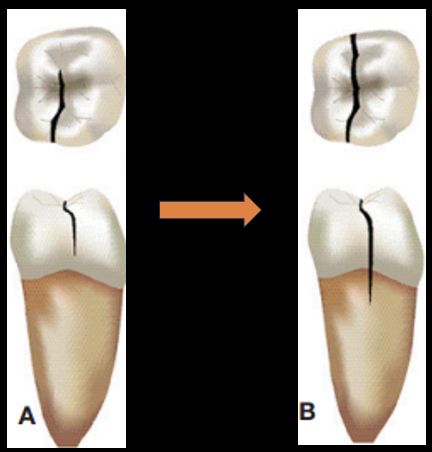
split root
continuation of a crack or vertical root fracture whereby the fx segments are completely separated longitudinally; can occur B/L or M/D
cracked teeth and VRF can be caused by
occlusal forces and dental procedures
cracked teeth/VRF can provide pathways for bacterial penetration in the ______
pulp
cracked teeth/VRF ________ over time
expand
cracked teeth/VRF may occur due to the reduction in ___________ w age
fracture resistance of the root
is there pain w cracked teeth/VRF
possible
is it easy or difficult to dx/tx plan cracked teeth/VRF
difficult
what are some diagnostic aids that can be used to help find/dx cracked teeth/VRF
CC and HPI
EOE, IOE
pulp vitality
percussion
palpation
periodontal probing
bite test
radiographs
transillumination
restoration removal
staining
wedging worse
surgical exploration
what kind of questions can you ask pt when hearing about their CC and HPI
exacerbating and relieving factors
hx of cracked teeth or VRF
parafunctional habits
TMJ pain
do they wear a NG
what signs would be seen in IOE and EOE in suspicion of cracked teeth/VRF
enlarged jaw muscles
attrition/abfraction/recession
wear facets
fractured cusps
numerous full coverage restorations
stained cracks
what sensibility tests can be used for determinign correct pulpal and periapical dx
percussion
palpation
cold test
EPT
probing depths
mobility
what type of probe is more accurate in determining a pocket that is more associated w a crack
plastic- more flexible and accuate compared to standard metal probe
what can be used to conduct a bite test
tooth slooth

goal of using a tooth slooth
attempt to replicate pts chief complaint
how to use tooth slooth
place instrument on each cusp and instruct pt to “bite slightly, squeeze tightly, and open quickly”
test several teeth
watch for pts response on bite and release

classic symptoms of cracked teeth
pain on biting

if you are doing the bite test on a pt and the pt doesn’t respond negatively, does this mean you can rule out a tooth fracture
no
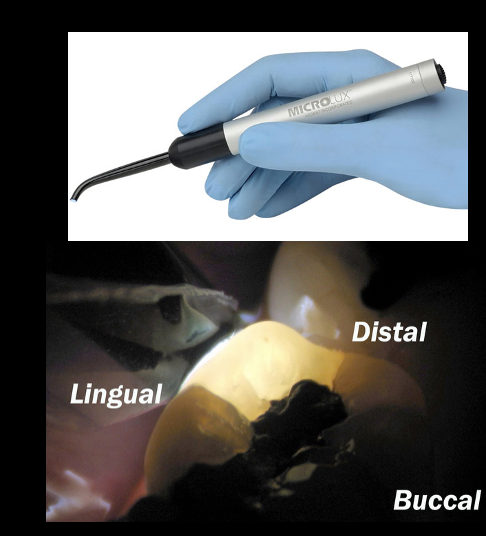
principle theory of transillumination
transmitting a beam of light penetrating through tooth structure until it meets a space (in this case, a fracture) that reflects the light beam from the crack plane
how likely is it that you will be able to dx a crack from a radiograph
usually can’t see radiographically unless the crack is rlly big
what to evaluate in periapial radiographs
continuity or lamina dura and uniformity of PDL space
quality and extent of existing endodontics and restorative tx
take multiple angled radiographs
what radiographs are helpful to use a dx aids
periapical radiographs
can CBCT be used to detect fractures
can aid in fx detection, but the width of unseparated fracture is typically undetectable <75 microns
what can CBCT be used for as a diagnostic aid
evaluating bone loss along fracture line
cracked teeth are incomplete fractures initiating from…
the crown extending subgingivally
cracked teeth are usualyl directed ______ (M-D/B-L)
M-D (crossing 1 or both marginal ridges)
signs and symptoms vary based on ________, but as soon as these signs and symptoms start to develop, this can be referred to as __________
extent of crack; cracked tooth syndrome
signs and symptoms associated w cracked tooth syndrome
sharp pain on biting and increased cold sensitivity
prevalence of cracked teeth
mand 2nd molars > mand 1 molars > max 1st molars > max 2nd molars
how to reach diagnosis of cracked tooth
hx of cracked teeth or parafunctional habits
transillumination
microscopic evaluations
staining w methylene blue
tooth slooth
periodontal probing → apical extension
radiographs
orthodontic band or diagnostic provisional
_________ may be the only way to replicate the pts chief complaint
tooth slooth
how do orthodontic band or diagnostic provisional help in dx of a crack
orthodontic band, or prep tooth for a crown and put a provisional on for a few months → both options should stabilize the crack → prevent further propagation → see if pulpal response has changed at all
tx planning a cracked tooth is dependent on
location and extent of crack
performing rct tx on cracked tooth is dependent on ______ and _______ dx
pulpal; periapical dx
in a study that evaluated cracked teeth w reversible pulpitis receiving crowns, what was found in pts needed RCT vs pts not needing one
20% required RCT within 6 mo of crown delivery
80% did NOT require RCT over the next 6 yrs
do all teeth with cracks need RCT tx
NO
study done on endodontic prognosis of cracked teeth:
5 yr survival rate of 92%,
but when there was extension of crack to the pulpal floor there was a ___% survival
when there was no pulpal floor extension, there was a __% survival
88% (reduced)
99%
study done on endodontic prognosis of cracked teeth:
2 yr survival rate 90%
teeth w probing depth of >6 mm had a ___% survival rate
teeth w probing depth of <6 mm had a ___% survival rate
74%
96.8%
study done on endodontic prognosis of cracked teeth:
had a 1-yr survival rate of 82%
they found the most significant indicators of tx success were _________, ___________, and __________
distal marginal ridge crack, deep probing depths, and periapical dx
vertical root fractures are usually directed ________ (B-L/M-D)
B-L or M-D
vertical root fractures happen most commonly to _________ teeth
endodontically treated (esp if RCT involved excessive removal of dentin or large obturations or post placement)
roots that are ____________________ are most susceptible to vertical root fractures
curved and narrow M-D or w developmental depressions
vertical root fractures _______ (can/can’t) be radiographically evident
can (J-shaped RL)
teeth in the mouth most susceptible to vertical root fractures are…
MB lower molars or B root of max premolars
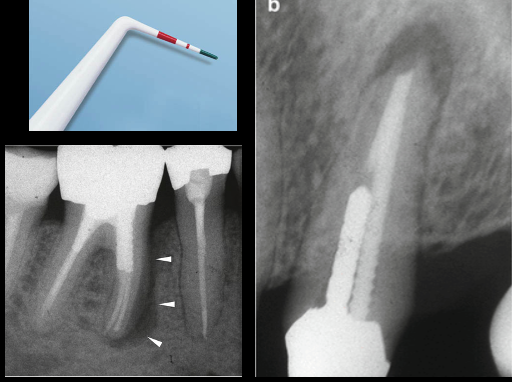
periodontal probings indicative of VRF
narrow, isolated deep probing w plastic probe (may need to numb is pt is hurting while probing)

signs in radiograph inicative of VRF
PA: halo or J-shaped PARL
CBCT
surgical exploration to aid in dx of VRF
staining
transillumination
way to prevent VRF while performing rct
preserve pericervical dentin during access
enhanced irrigation and conservative cleaning and shaping/obturation
fiber post use → make endo teeth more resistant to fx vs metal tapered post
if pt has parafunctional habits, what is a preventative method against VRF
occlusal guard
when placing posts during a RCT, the post should fit ___ in the existing canal
passively
proper _______ and emphasis on ___________ in cracked teeth and VRF are essential
dx; early detection