EM 3 Fixational EM
1/107
Earn XP
Description and Tags
Fixational EM
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
What are fixational eye movements and their main characteristic?
Micro/miniature eye movements during fixation
Eyes are never perfectly still even when fixating
Maintain visual perception during steady gaze
Why are fixational eye movements clinically and experimentally important?
Help distinguish normal vs abnormal eye movement patterns
Critical for tasks requiring stable fixation
Affect accuracy of ocular measurements/instrumentation
In what clinical/imaging contexts are fixational eye movements important?
Visual field testing
Corneal topography
LASIK procedures
OCT (optical coherence tomography)
→ Precise fixation needed for accurate results
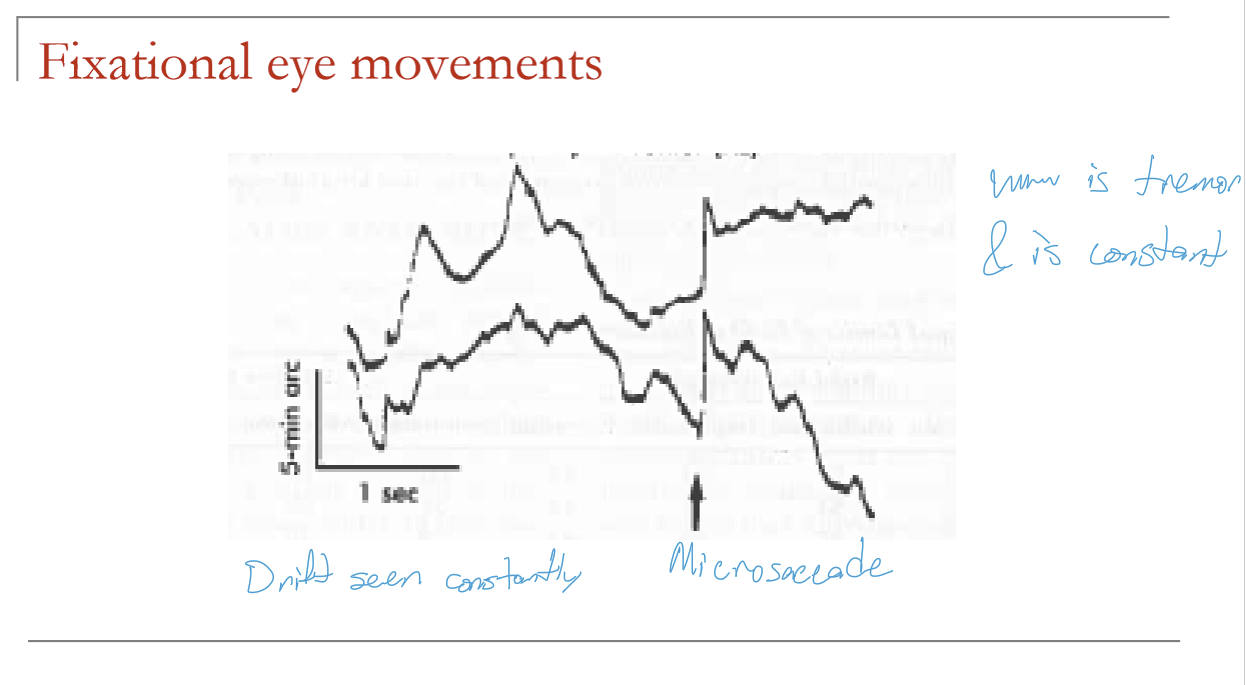
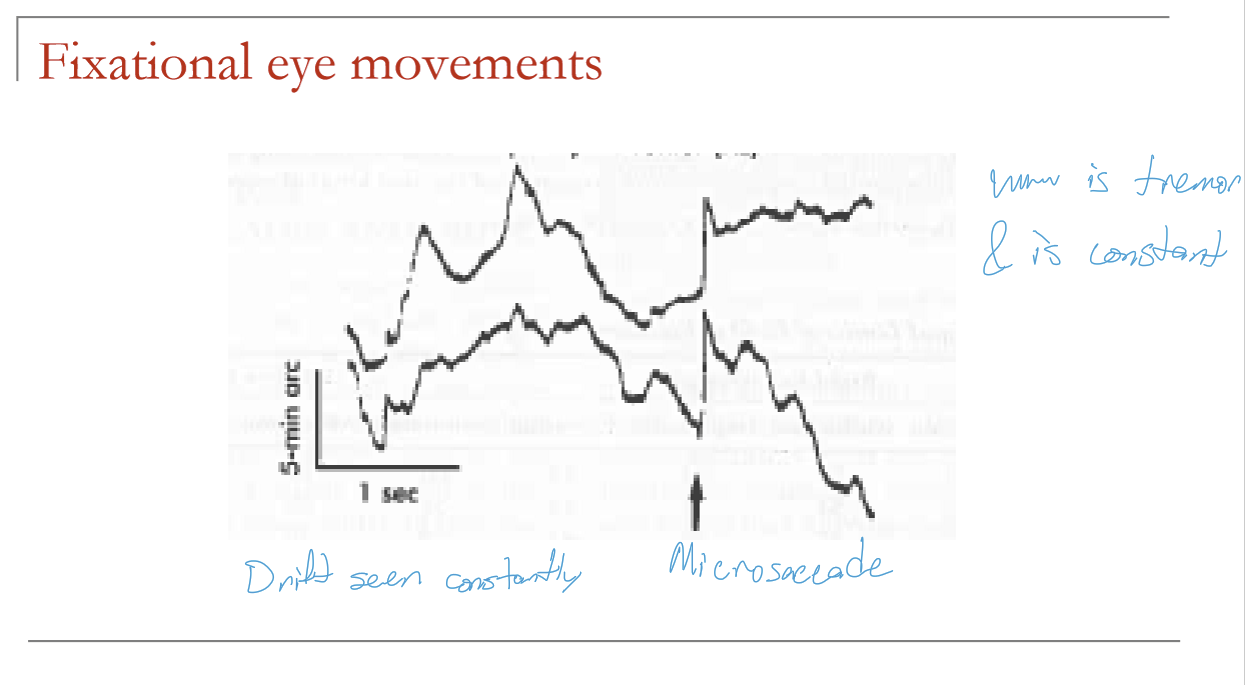
What are the three types of fixational eye movements and their general significance?
Tremor
Drift
Microsaccades
These occur during attempted fixation because the eyes are never perfectly still.
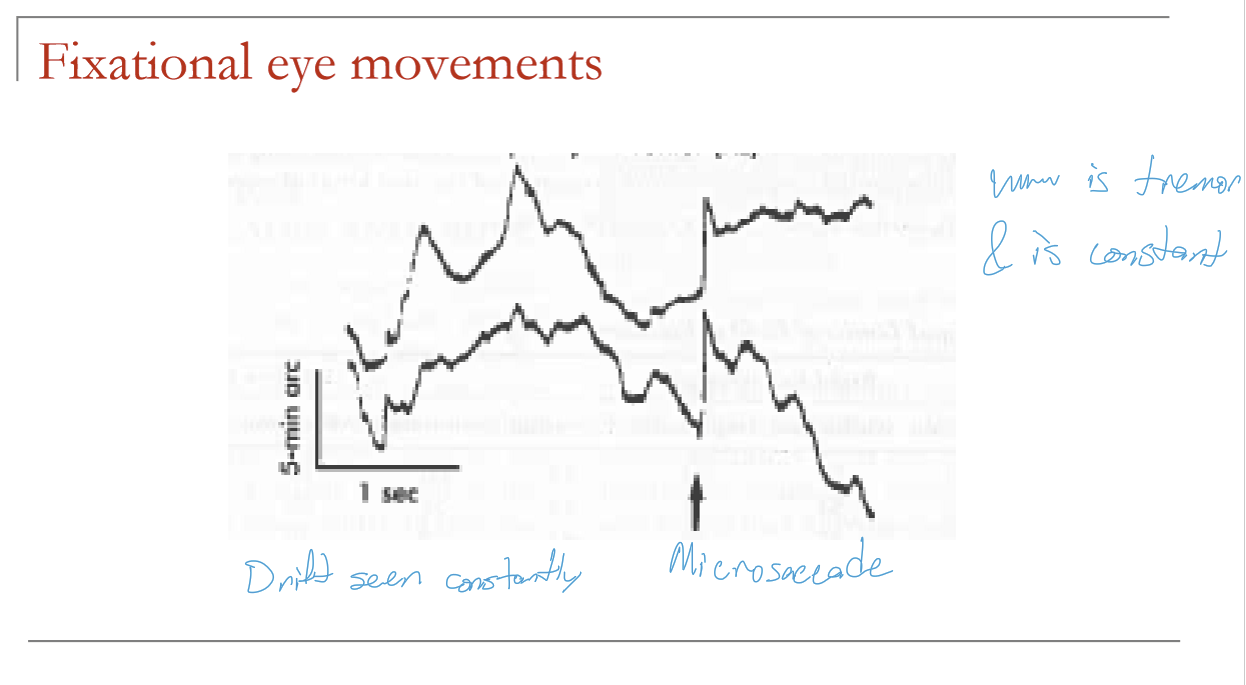
What are the characteristics of tremor in fixational eye movements?
High frequency: 30–100 Hz
Very small amplitude: 5–30 arcseconds (30 arcseconds = 1/120 of a degree)
Generally considered noise
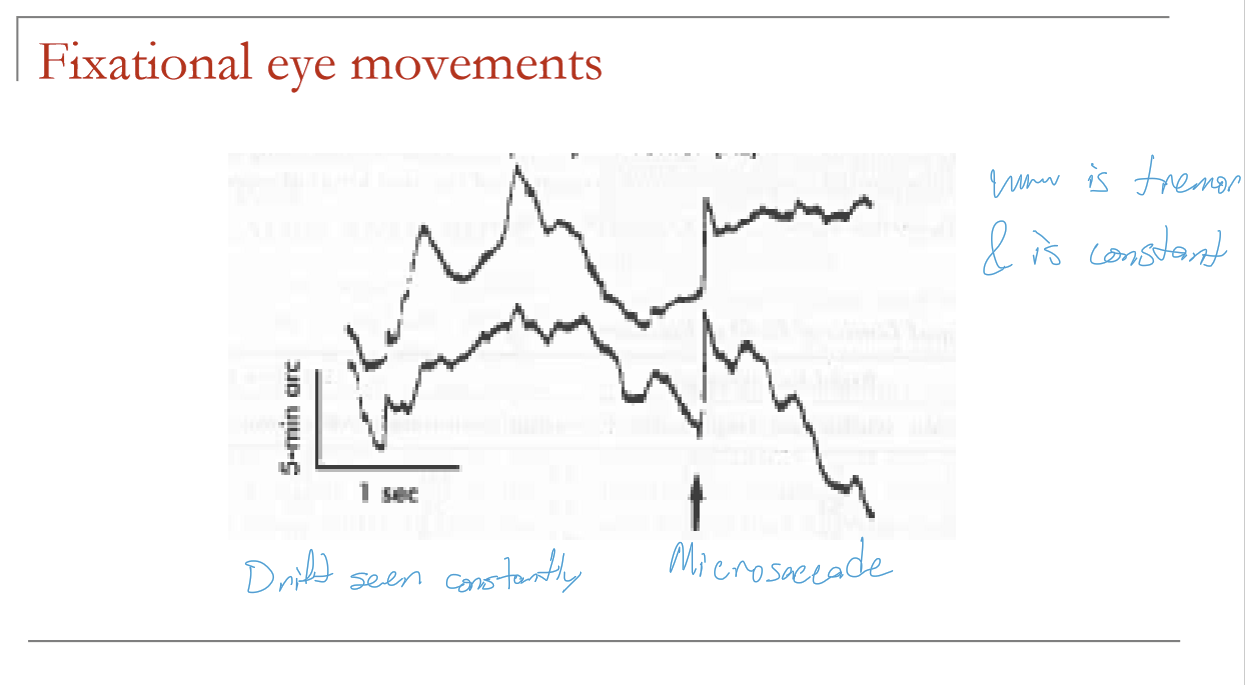
What are the characteristics of drift in fixational eye movements?
Slow movement during fixation
Velocity: 1–8 arcmin/sec (~5 arcmin/sec mean)
Amplitude: ~2–5 arcmin
Probably noise, but may help with error correction
What are the characteristics of microsaccades in fixational eye movements?
Occur 1–2 times per second
Mean amplitude: ~5 arcmin
Range: 1–25 arcmin
Rarely >10 arcmin
Usually error-correcting
Which fixational eye movements are mainly considered noise vs error-correcting?
Tremor: mostly noise
Drift: probably noise, but may be error-correcting
Microsaccades: usually error-correcting
How does the area of fixation variability change with fixation time?
The area over which fixation varies increases with fixation time
Longer fixation → greater spread around the point of regard
What is meant by a directional bias in fixation?
Fixation does not vary equally in all directions
What are the key characteristics of variation during fixation?
Fixation is not perfectly stable
Variability increases over time
Variability often has a preferred direction (directional bias)
What happens to a stabilized retinal image over time?
Initially seen clearly
After a few seconds, it fades away
Leaves a virtually blank field
What does the fading of a stabilized retinal image suggest about fixational eye movements?
Small eye movements are needed to keep the image changing on the retina
Without retinal image motion, perception fades
Therefore, fixational eye movements help maintain visual awareness
What is the Troxler effect?
Described by Troxler (1804)
Stationary retinal images fade from perception during steady fixation
Demonstrates perceptual fading when visual input is not refreshed by eye movements
What do stabilized retinal image experiments show about tremor and drift?
Simulated tremor and drift contribute little to visibility
They do not significantly improve perception of a stabilized image
Which fixational eye movement contributes most to improving visibility in stabilized retinal image testing?
Microsaccade-like movements
They produce much greater improvement in visibility than tremor or drift
What do stabilized retinal image studies suggest about the function of microsaccades?
Microsaccades help refresh the retinal image
They are likely the most important fixational movement for maintaining visibility
Supports their role in preventing perceptual fading
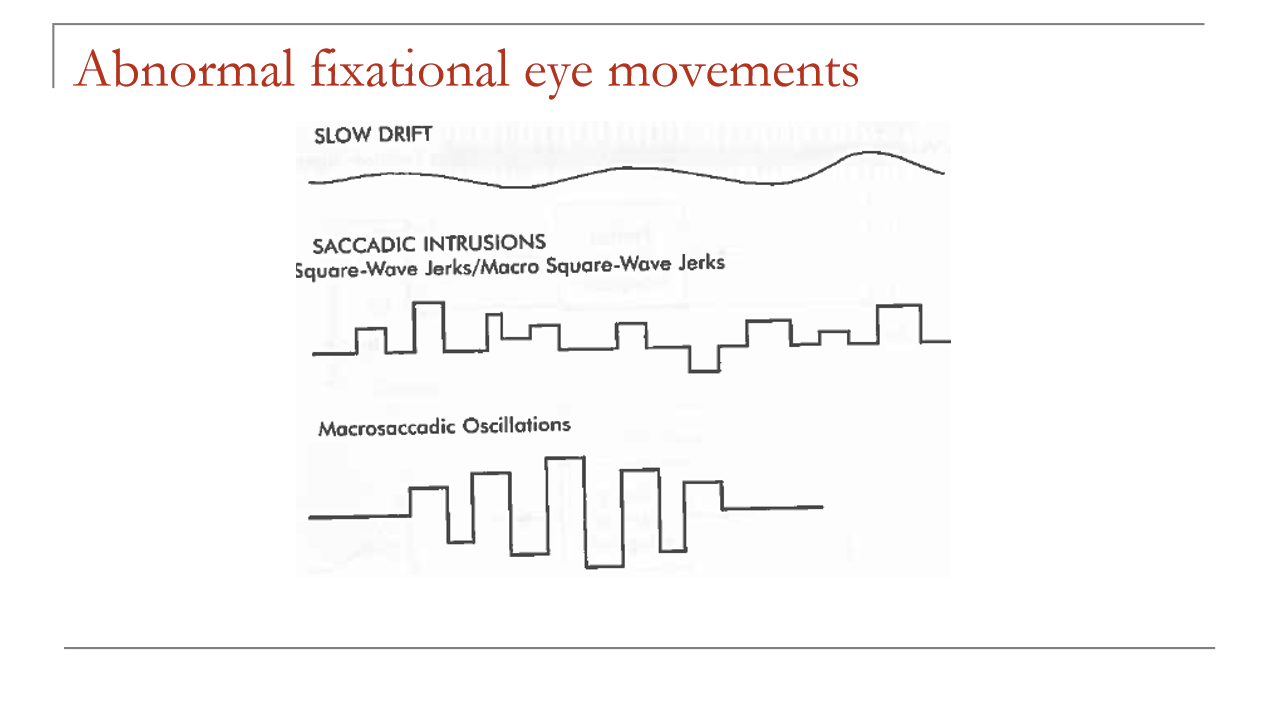
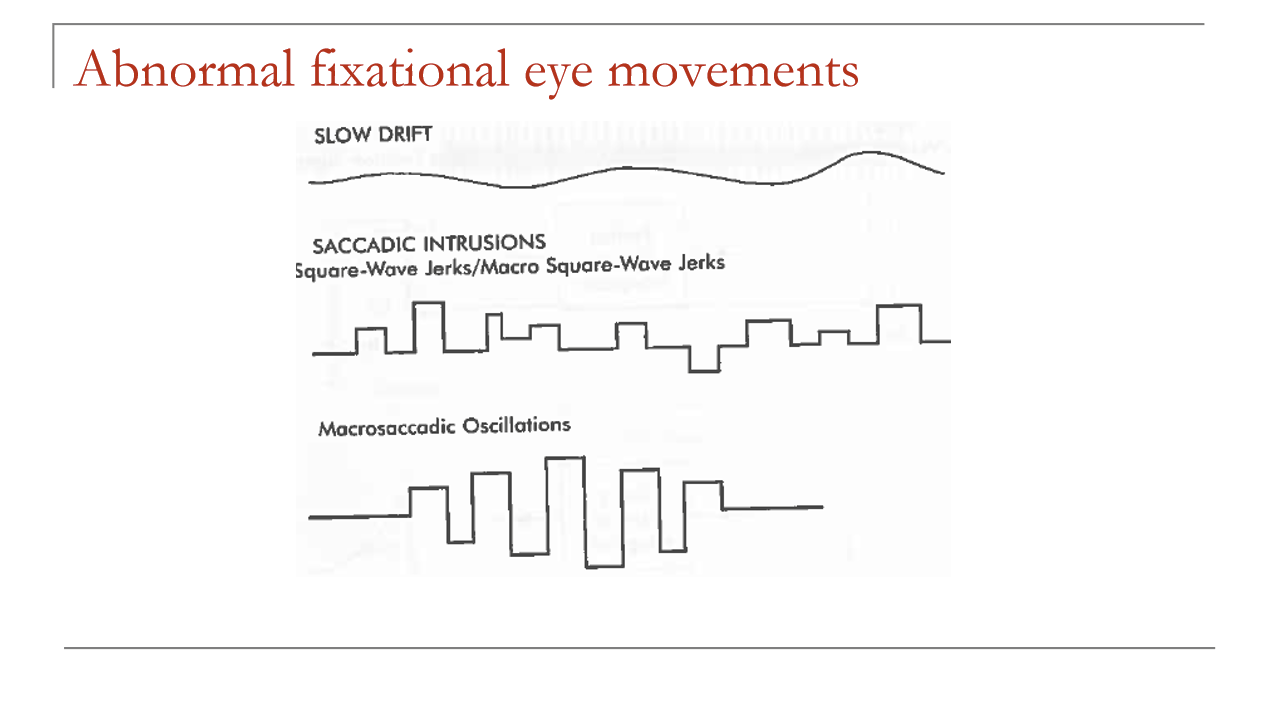
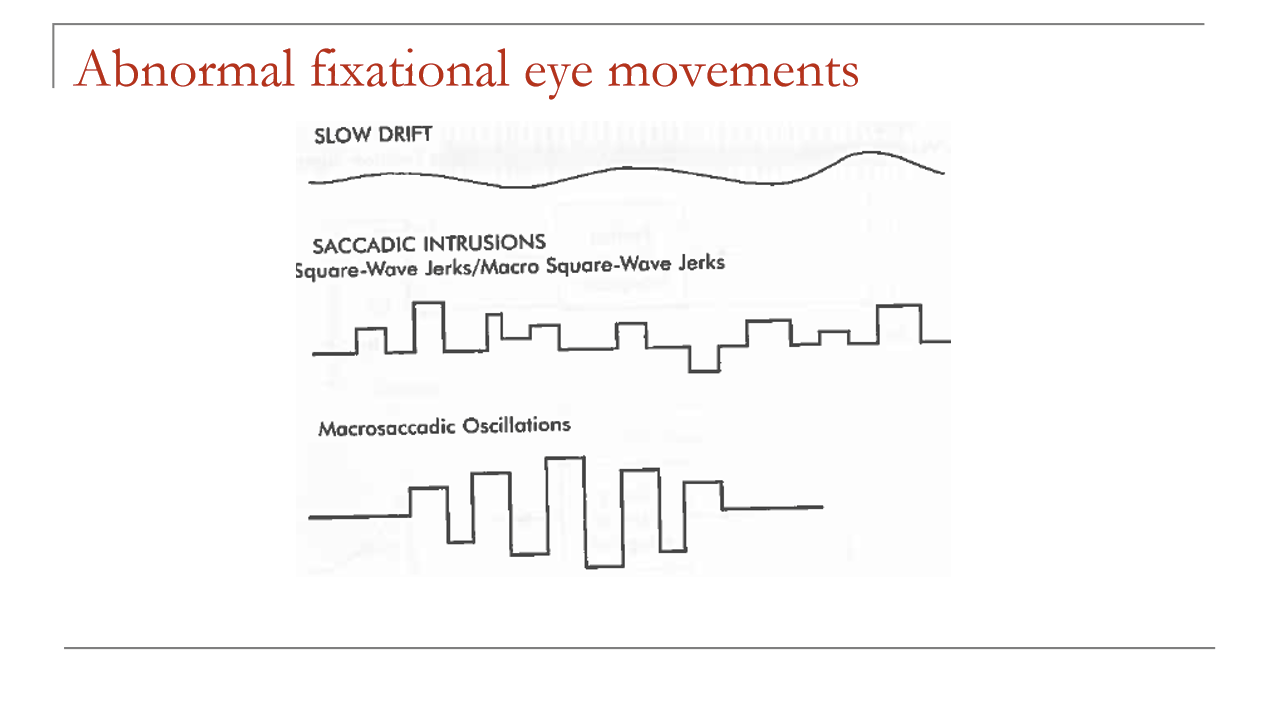
What are the 3 major categories of fixation abnormalities?
Slow drift
Saccadic intrusions
Nystagmus
What should be done if it is unclear whether a fixation abnormality is acquired or congenital?
Refer for additional testing
Distinguishing acquired vs congenital is clinically important
What are common causes of acquired fixational abnormalities?
Stroke
Tumor
Aneurysm
Infection
Multiple sclerosis (MS)
Which lesion locations are especially associated with acquired fixation abnormalities in MS?
Brainstem
Cerebellum
Vestibular system
What is slow drift as an abnormal fixational eye movement, and what condition is it commonly associated with?
A type of abnormal fixation instability
Common in amblyopia
Typically a monocular phenomenon
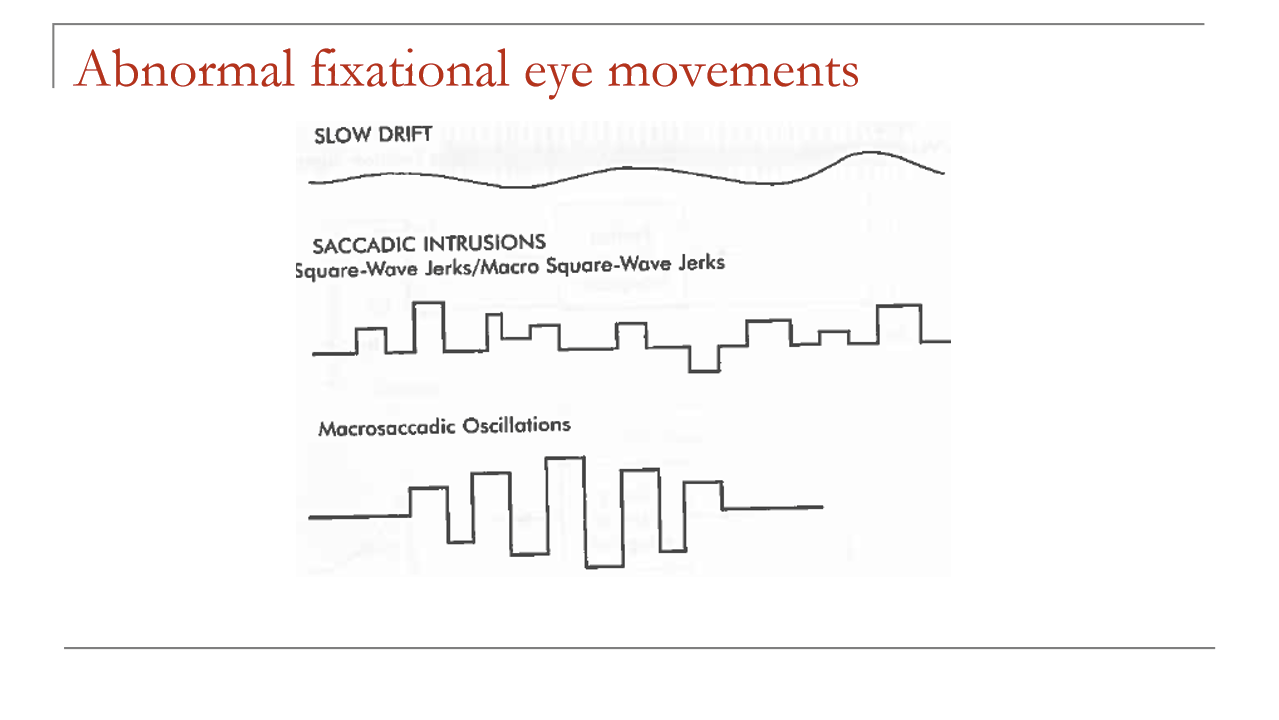
What are the typical amplitude and velocity of abnormal slow drift?
Amplitude: ≤ 1°
Velocity: < 3°/sec
How is abnormal slow drift usually corrected?
Probably corrected by saccades
Meaning: the eye slowly drifts off target, then a corrective saccade brings fixation back
How does abnormal slow drift differ from normal fixational drift?
Normal drift: tiny, slow fixational movement during normal fixation
Abnormal slow drift: larger, pathologic fixation instability
In abnormal slow drift: amplitude can be up to 1°, often seen in amblyopia, and is corrected by saccades
What are saccadic intrusions, and when should they be referred?
A category of abnormal fixational eye movements
Refer if not long-standing
Important because they may indicate neurologic disease
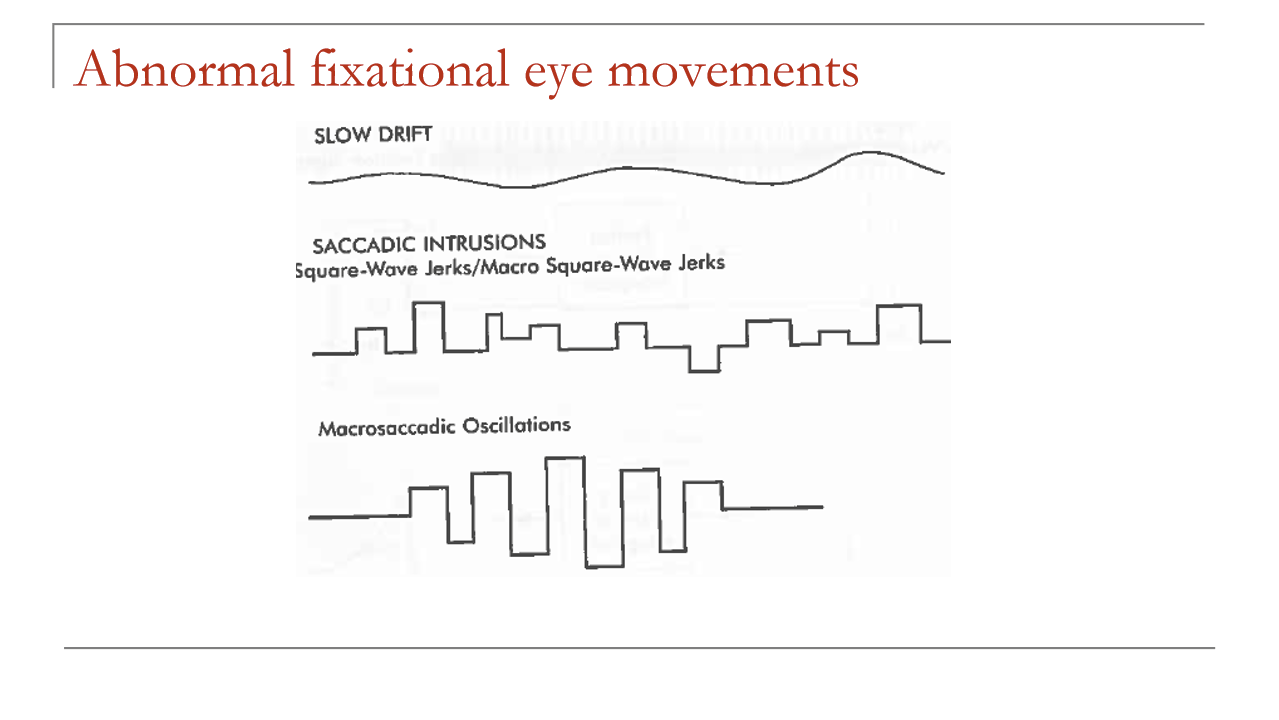
What is a square-wave jerk, and what is its clinical significance?
A type of saccadic intrusion
Seen in 25–60% of normal individuals
Amplitude: 0.5–5°
May indicate cerebellar disease or multiple sclerosis (MS)
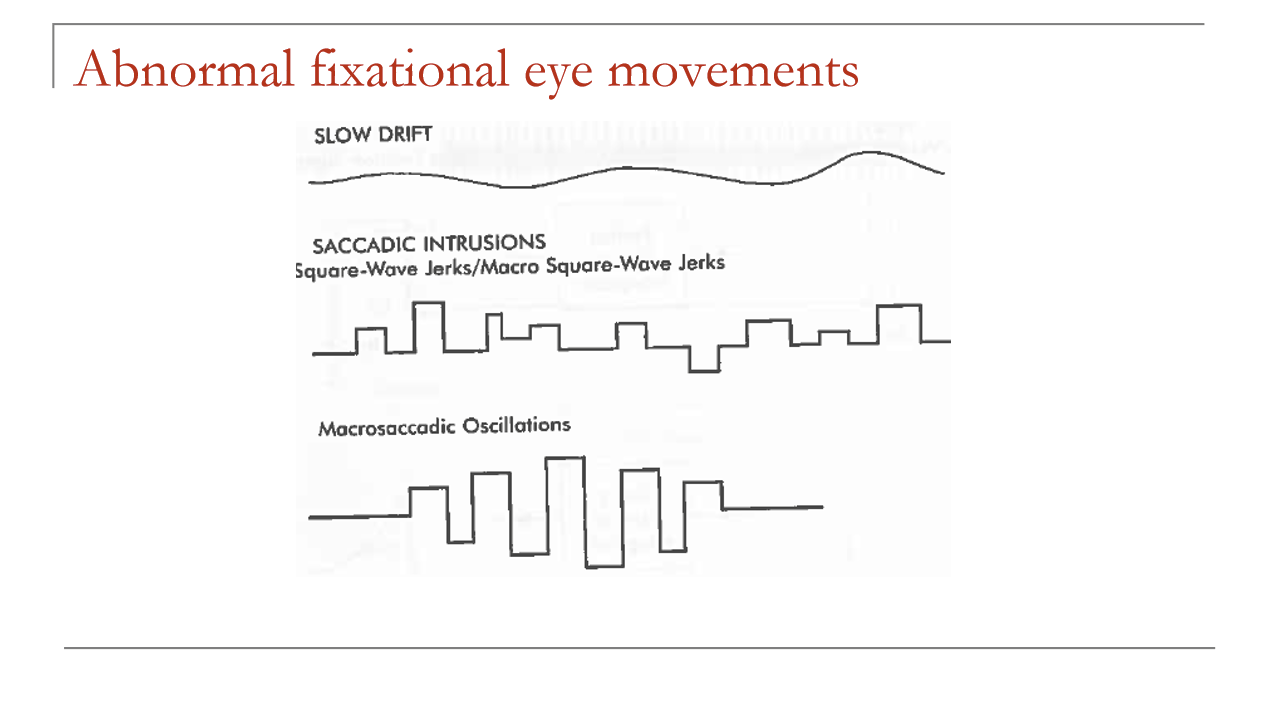
What is a macro square-wave jerk, and what are the common causes?
Larger form of a square-wave jerk
Amplitude: 5 to 15°
Most commonly associated with cerebellar disease and MS
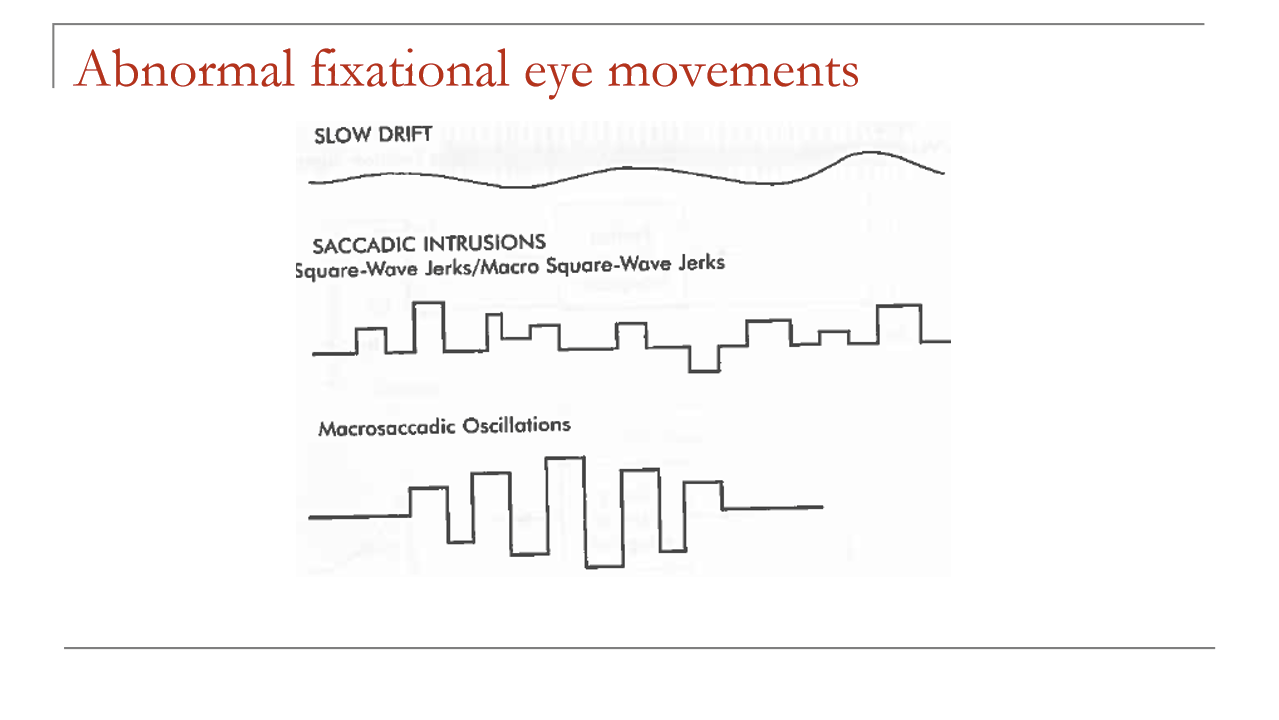
What is macrosaccadic oscillation?
A sequence of saccades to either side of fixation
Amplitude first increases, then decreases
Represents an abnormal oscillation around the fixation point
How do square-wave jerk, macro square-wave jerk, and macrosaccadic oscillation differ?
Square-wave jerk: 0.5–5°, can occur in normals
Macro square-wave jerk: 5–15°, more pathologic
Macrosaccadic oscillation: back-and-forth saccades with increasing then decreasing amplitude around fixation
What is nystagmus as an abnormal fixational eye movement?
Rhythmic oscillation of the eyes
Can be congenital or acquired
Congenital nystagmus is also called infantile nystagmus syndrome (INS)
What are the 2 main types of nystagmus?
Pendular nystagmus
Jerk nystagmus
Can pendular and jerk nystagmus be congenital or acquired?
Pendular nystagmus: can be congenital or acquired
Jerk nystagmus: can also be congenital or acquired
How is congenital nystagmus commonly labeled?
CN = congenital nystagmus
Also referred to as infantile nystagmus syndrome (INS)
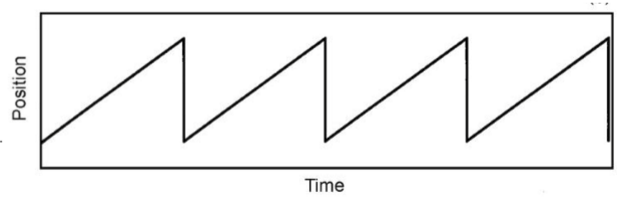
What is the characteristic waveform of jerk nystagmus?
Constant-velocity slow phase with a corrective fast phase
Produces a saw-tooth waveform on position vs time tracing
What are the major types/causes of jerk nystagmus shown on this slide?
Vestibular nystagmus
Optokinetic nystagmus (OKN)
What are the physiologic forms of vestibular jerk nystagmus?
Post-rotary nystagmus → occurs after spinning/rotation
Caloric nystagmus → induced by warm or cold stimulation in the ear
Can vestibular jerk nystagmus be physiologic or pathologic?
Yes
Can be physiologic (post-rotary, caloric)
Can also be acquired/pathologic
How do you recognize jerk nystagmus on a tracing?
Slow drift in one direction
Followed by a rapid corrective jump
Repeats rhythmically → classic saw-tooth pattern
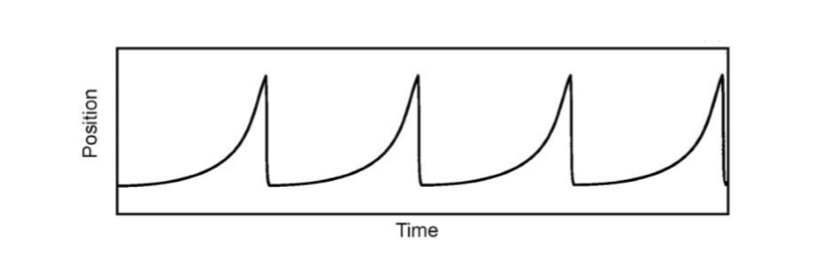
What nystagmus waveform is characterized by an accelerating slow phase?
Accelerating slow-phase nystagmus
Usually congenital
Commonly associated with congenital nystagmus / infantile nystagmus syndrome (INS)
How does an accelerating slow phase appear on a position-vs-time tracing?
The eye drifts away from fixation with increasing velocity
Followed by a quick corrective fast phase
Produces a repetitive jerk waveform
How does accelerating slow-phase nystagmus differ from constant-velocity slow-phase jerk nystagmus?
Accelerating slow phase: slow phase speeds up over time; usually congenital
Constant-velocity slow phase: slow phase stays uniform; often vestibular/optokinetic
Both are jerk nystagmus waveforms
What jerk nystagmus waveform is characterized by a decelerating slow phase?
Decelerating slow-phase jerk nystagmus
Includes gaze-evoked nystagmus
Also seen in latent nystagmus / manifest latent nystagmus
What is gaze-evoked nystagmus, and what is its movement pattern?
A form of decelerating slow-phase jerk nystagmus
Eye drifts toward primary gaze
Then a corrective saccade brings the eye back to fixation
What are important causes/associations of gaze-evoked nystagmus?
Drug induced (especially alcohol)
May be physiologic as endpoint nystagmus
When should gaze-evoked nystagmus be considered suspicious for an acquired abnormality?
If it occurs at less extreme gaze angles
Endpoint nystagmus at extreme gaze can be physiologic
Earlier onset in gaze = more concerning for acquired pathology
What is another nystagmus associated with a decelerating slow phase?
Latent nystagmus
Also called manifest latent nystagmus
What proportion of patients with nystagmus also have strabismus?
About 50% of patients with nystagmus have strabismus
Is congenital nystagmus usually idiopathic or associated with other disorders?
Can be idiopathic
Can also be associated with multiple disorders
What disorders are commonly associated with congenital nystagmus?
Albinism
Congenital cataract
Retinal disease
ONH (optic nerve hypoplasia)
When does congenital nystagmus typically present?
Usually appears within the first few months of life
What is the null position in congenital nystagmus?
The gaze direction where nystagmus intensity is least
Intensity = amplitude × frequency
At the null position, visual acuity is optimal
What is periodic alternating nystagmus (PAN) in congenital nystagmus?
A form where the null position shifts over time
Shift occurs over several minutes or longer
How does convergence affect congenital nystagmus?
There is often a reduction in nystagmus with convergence
What are the key clinical characteristics of congenital nystagmus?
Appears in the first few months of life
Usually has a null position where intensity is lowest and vision is best
PAN may cause the null to shift over time
Often improves with convergence
What are foveation periods in congenital nystagmus?
Brief periods when the eyes are relatively stable
Allow the image to fall closer to the fovea
Important because they are the moments of best visual function
Do patients with congenital nystagmus usually experience oscillopsia (a visual symptom where stationary objects or your surroundings appear to continuously shake, bounce, jiggle, or vibrate)?
No
Patients with congenital nystagmus typically do not perceive the world as moving
What is the typical abnormal head posture seen in congenital nystagmus, and why does it occur?
Patient turns the head opposite the null position
This keeps the eyes positioned in the null direction when looking straight ahead relative to the head
Purpose: reduce nystagmus and optimize vision
What is the usual direction of movement in congenital nystagmus?
Typically horizontal
What is the key rule regarding acquired nystagmus?
Acquired nystagmus is not normal
If you cannot prove it is congenital, then refer
What is the clinical recommendation if nystagmus cannot be shown to be congenital?
Refer the patient
The slide emphasizes: “If cannot prove it’s congenital, refer!!”
What findings favor congenital nystagmus over acquired nystagmus?
Congenital nystagmus:
Null point present
Decreases with convergence
Usually horizontal
No oscillopsia
Foveation periods present
Abnormal head posture common
Acquired nystagmus:
No null point
No improvement with convergence
Direction can be any
Oscillopsia present
No foveation periods
No abnormal head posture
What feature of nystagmus direction may suggest congenital nystagmus?
Congenital nystagmus is usually not two-dimensional
So nystagmus that is not two-dimensional is more consistent with congenital forms
What additional consideration is mentioned for a child with nystagmus?
Even if the nystagmus seems congenital, in a child you may still consider a brain scan
How can prism be used to manage congenital nystagmus with a null point?
Use prism to shift the image toward the null point
Goal: reduce abnormal head turn and improve comfort/vision
Example:
If null point is to the right → prescribe base-left prism
Why is prism prescribed toward the null point in congenital nystagmus?
Moves the visual target into the gaze position where nystagmus is least
Helps the patient use the null position without turning the head
Therefore decreases abnormal head posture
How can base-out (BO) prism help in congenital nystagmus?
BO prism increases convergence demand
Since congenital nystagmus often decreases with convergence, BO prism may help reduce nystagmus
What is the goal of surgery in the management of congenital nystagmus?
To move the eyes toward the null point
More accurately: shift the null point toward primary gaze
Main benefit: decreases abnormal head turn
What surgical approach is described for congenital nystagmus with an abnormal head posture?
A 2-muscle procedure
Designed to make the patient use the null position in primary gaze
Goal: reduce head posture by relocating the functional null point
If the null point is to the right, what muscle surgery can be done?
Weaken right LR + left MR
This makes the patient need to pull more to the right to keep the eyes straight
Effectively helps place the null point in primary position
What is an alternative surgical strategy if the null point is to the right?
Could also strengthen right MR + left LR
Same principle: shift the eye position demand so primary gaze aligns more with the null point
What is tenotomy surgery in the management of congenital nystagmus?
A 4-muscle procedure
Involves detaching all 4 horizontal recti and reattaching them
May be done in the same position or combined with repositioning
Which extraocular muscles are involved in the 4-muscle tenotomy procedure for congenital nystagmus?
All horizontal recti:
Right medial rectus
Right lateral rectus
Left medial rectus
Left lateral rectus
How can a combined tenotomy procedure differ from a standard 4-muscle tenotomy?
Standard tenotomy: muscles are cut and reattached in the same place
Combined procedure: tenotomy is done with repositioning of muscles, similar to a 2-muscle null-point procedure
What is latent nystagmus, and how is it usually classified?
Almost always congenital
Often associated with strabismus
It is a jerk nystagmus with a decelerating slow phase
When is latent nystagmus typically elicited, and what is the direction of the fast phase?
Occurs when one eye is covered
The fast phase is toward the viewing eye
What is manifest latent nystagmus (MLN)?
Called manifest latent nystagmus because there is often a small nystagmus even under binocular viewing
This binocular nystagmus is often subclinical
Does latent nystagmus usually require treatment, and why is it still clinically important?
Usually no treatment required
Important because it can affect the eye exam, especially when covering one eye
What is the clinical significance of acquired nystagmus?
Almost always requires referral
Often indicates an underlying neurologic, vestibular, toxic, or drug-related cause
What are the major neurologic causes of acquired nystagmus?
acq:
Stroke
Tumor
Aneurysm
Infection
Multiple sclerosis (MS)
Key MS locations:
Brainstem
Cerebellum
Vestibular system
What toxic or medication-related causes can produce acquired nystagmus?
Alcohol intoxication
Phenytoin (Dilantin)
Other anti-seizure medications
Sedatives
What type of nystagmus is gaze-evoked nystagmus?
A jerk nystagmus
Has a decelerating slow phase
What is the normal/physiologic form of gaze-evoked nystagmus?
Endpoint nystagmus
Also called physiological nystagmus
It is still a jerk nystagmus
What does pathologic gaze-evoked nystagmus suggest, and what are common causes?
Suggests a neurologic disorder
Common associations:
Multiple sclerosis (MS)
Cerebellar disease
Vestibular system disorders
How do physiologic endpoint nystagmus and pathologic gaze-evoked nystagmus compare?
Both: are jerk nystagmus with a decelerating slow phase
Physiologic form: endpoint nystagmus at extreme gaze
Pathologic form: due to neurologic disease (e.g., MS, cerebellar, vestibular lesions)
How is horizontal gaze nystagmus (HGN) used in alcohol testing?
Used as a roadside sobriety test
Helpful when direct blood alcohol concentration (BAC) testing is not practical
Alcohol can produce horizontal gaze-evoked jerk nystagmus
What is the relationship between angle of onset of nystagmus and BAC in alcohol intoxication?
Earlier onset of gaze-evoked nystagmus is associated with higher BAC
Tharp finding:
Angle of onset ≈ 51° – 105(BAC)Reported that HGN testing could identify BAC ≥ 0.10% about 77% of the time
How was gaze nystagmus scoring used in the Dr. Good study?
Highway patrol examiners scored gaze nystagmus on a 0–6 scale
4 or greater = failure
Used to help predict whether BAC was ≥ 0.10%
What is visuoscopy and what instrument is used?
A method to assess fixation location on the retina
Performed with a direct ophthalmoscope using the fixation target setting
What does the patient see and what does the examiner see during visuoscopy?
Patient: sees the fixation target
Examiner: sees the target imaged on the retina
How does visuoscopy determine whether fixation is central?
View the macula with a direct ophthalmoscope fixation target
Have the patient look at the center of the target
If fixation is central, the foveal reflex aligns with the center of the target
What are the main purposes of visuoscopy when evaluating fixation?
Determine whether fixation is steady or unsteady
Determine whether fixation is central or eccentric
If eccentric, determine the direction and magnitude of eccentric fixation
How do you interpret the rings in a visuoscopy target when measuring eccentric fixation?
The center ring has a radius of 1 prism diopter (pd)
Each successive ring increases by 1 pd
This lets you estimate the magnitude of eccentric fixation in pd
What is an important distinction regarding eccentric fixation?
Do not confuse eccentric fixation with eccentric viewing
Eccentric fixation = abnormal retinal locus used for fixation
Eccentric viewing is a different concept
What is eccentric fixation?
Patient believes they are looking straight at the target
There is a change in monocular visual direction
Uses a nonfoveal retinal point for fixation
Clinically, we try to eliminate eccentric fixation
What is eccentric viewing?
Used by patients with a central scotoma
Patient intentionally looks away from the target
Purpose: place the image on a healthier nonfoveal retinal area
Clinically, patients may be taught eccentric viewing
How do eccentric fixation and eccentric viewing differ in patient awareness and mechanism?
Eccentric fixation: patient thinks they are looking directly at the target; abnormal monocular visual direction
Eccentric viewing: patient knowingly looks off to the side because straight-ahead viewing does not allow the target to be seen
How can best visual acuity be approximated in a patient with eccentric fixation?
Use the formula: MAR = EF + 1
MAR = minimum angle of resolution (in arcminutes)
EF = magnitude of eccentric fixation (in prism diopters, pd)
What is MAR, and how does it relate to Snellen acuity?
MAR = minimum angle of resolution in minutes of arc
It is the reciprocal of the Snellen fraction
Examples:
20/20 → MAR = 1
20/40 → MAR = 2
How is fixation assessed with a penlight?
Patient monocularly fixates a penlight held by the examiner
Examiner sights over the penlight
Note the position of the first Purkinje image (corneal reflex) relative to the center of the entrance pupil