[PT10117] [1T1S] [1.2] Proprioceptive Neuromuscular Facilitation (PNF)
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
68 Terms
Who believed that physiologic and proprioception can be applied to trat patients with neurological conditions?
Dr. Herman Kabat
Aside from Dr. Kabat, who are his two students who helped develop a book discussing PNF?
Margarett Knott
Dorothy Voss
A system of promoting/facilitating the response of the neuromuscular mechanism by stimulating the proprioceptors
Proprioceptive Neuromuscular Facilitation (PNF)
How can you differentiate PNF from Rood’s?
PNF stimulates proprioceptors
Rood stimulates tactile and sensory receptors
What movement patterns does PNF utilize?
Spiral and diagonal movement patterns
Three Sherrington’s Neurophysiological Principles (3)
Reciprocal innervation
Successive induction
Irradiation
SHERRINGTON’S NEUROPHYSIOLOGICAL PRINCIPLES
What principle is described below:
The contraction of muscles is accompanied by the simultaneous inhibition of their antagonists
Reciprocal innervation
SHERRINGTON’S NEUROPHYSIOLOGICAL PRINCIPLES
What principle is described below:
Increased excitation of the agonist muscles follows the stimulation and contraction of antagonists
Successive induction
SHERRINGTON’S NEUROPHYSIOLOGICAL PRINCIPLES
What principle is described below:
The spreading of excitation leads to increased strength of the response
Irradiance
Six Principles of PNF Techniques (6)
Potentials that have not been fully developed
Rhythmic and reversing in character of movement
Orderly sequence of total patterns of movement and posture
Repetition for retention of motor learning
Goal-directed activities
Selection of appropriate sensory cues
Three Unilateral Diagonal Patterns (3)
UE
LE
Head, neck and trunk
Three Bilateral Patterns (3)
Symmetric patterns
Asymmetric patterns
Reciprocal patterns
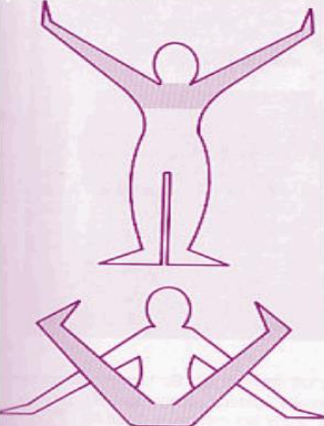
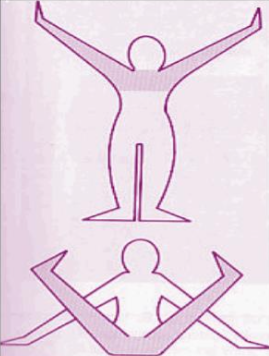
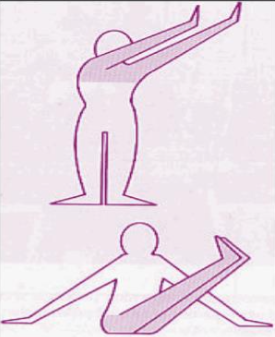
What bilateral pattern is shown on the picture?
Symmetrical
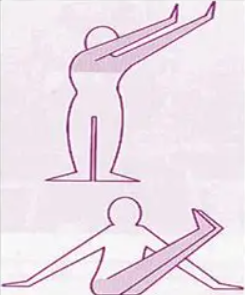
What bilateral pattern is shown on the picture?
Asymmetrical
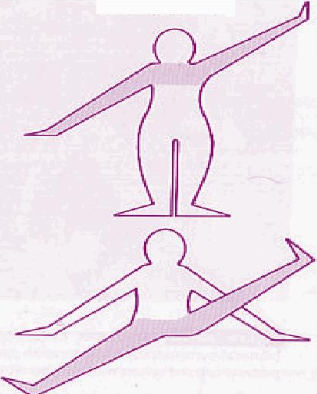
What bilateral pattern is shown on the picture?
Reciprocal
BILATERAL PATTERNS
Paired extremities perform like movements at the same time
Symmetrical patterns
BILATERAL PATTERNS
Paired extremities perform movements toward one side of the body at the same time
Facilitates trunk rotation
Chopping and lifting patterns
Asymmetrical patterns
BILATERAL PATTERNS
Paired extremities perform movements in the opposite direction at the same time
Reciprocal patterns

Three Combined UE/LE Movement Patterns (3)
Ipsilateral pattern
Contralateral pattern
Diagonal reciprocal pattern

What combined movement pattern is shown on the picture?
Contralateral

What combined movement pattern is shown on the picture?
Ipsilateral

What combined movement pattern is shown on the picture?
Diagonal reciprocal
COMBINED MOVEMENT PATTERNS
Extremities of the same side moving in the same direction at the same time
Ipsilateral pattern

COMBINED MOVEMENT PATTERNS
Extremities of the opposite sides moving in the same direction at the same time
Contralateral pattern

COMBINED MOVEMENT PATTERNS
Contralateral extremities moving in the same direction at the same time while opposite contralateral extremities move in the opposite direction
Diagonal reciprocal patterns

Six Progressions in Performing PNF techniques (6)
Total to individuated
Proximal to distal, distal to proximal
Mobile to stable
Gross to selective
Reflexive to deliberate
Overlapping of integrative
In performing PNF techniques, what muscle is considered as the agonist (weak/normal)?
Normal muscle = agonist
Weak = antagonist
BASIC PROCEDURES
Refers to how and where the therapist places his/her hands on the patient
Manual contact (MC)
BASIC PROCEDURES
Manual contact may be used for: (3)
Facilitatory mechanism
Give patient security in the presence of pain
Sensory cue (to understand the direction of anticipated movement)
BASIC PROCEDURES
Tone of voice may influence considerably the quality of response
Command and communication
BASIC PROCEDURES
The stretch stimulus is the placing of body segments in positions that lengthen the muscles
Stretch (STR)
BASIC PROCEDURES
Muscle responds with (greater/lesser) force after stretch
Muscle responds with greater force after stretch
BASIC PROCEDURES
How can you manually elicit the stretch reflex?
By “quickly” taking the part past the point of tension
BASIC PROCEDURES
Separating the joint surfaces to promote movement and inhibit pain (pulling action)
Traction (TR)
BASIC PROCEDURES
What is the indication for traction (TR)?
Stimulate afferent nerve endings → facilitate flexor muscles (mobilizing patterns)
BASIC PROCEDURES
Compressing the joint surfaces promotes stability, weight bearing or maintenance of posture (pushing action)
Approximation (AP)
BASIC PROCEDURES
What is the indication for approximation (AP)?
Stimulate afferent nerve endings → facilitate extensor muscles (stabilizing patterns)
BASIC PROCEDURES
Greatest amount of resistance possible that can be applied to an isotonic or active contraction → allowing full smooth ROM without pain
Maximal resistance (MR)
BASIC PROCEDURES
Movement performed against resistance of sufficient degree to demand maximal effort → increase in strength
Maximal resistance (MR)
BASIC PROCEDURES
Indications for maximal resistance (MR)? (2)
Weakness
Muscle imbalances
BASIC PROCEDURES
Sequence of distal to proximal muscle contraction that occurs in any motor activity → coordinated movement
Timing
BASIC PROCEDURES
Maximal resistance is superimposed upon patterns of facilitation with due regard for normal timing
Order that overflow/irradiation may occur from stronger to weaker muscles
Timing for emphasis
BASIC PROCEDURES
Indications for Timing (2)
Weakness
Incoordination
SPECIFIC TECHNIQUES
This set of interventions focuses on improving the strength and coordination of a target movement or pattern
Directed to agonist
BASIC PROCEDURES
This set of interventions focuses on the importance of coordinated agonist and antagonist muscle contractions (resist antagonistic pattern first)
Reversal of antagonist
BASIC PROCEDURES
This set of interventions focuses on training the patient to have control over hypertonia, spasticity, and muscle spasm
Relaxation
DIRECTED TO AGONIST
What are the four specific techniques? (4)
Repeated contraction
Rhythmic initiation
Hold relax active motion
Alternating isometrics
DIRECTED TO AGONIST
Repetition of activity is necessary for the learning process and the development of strength and endurance
Repeated contraction
DIRECTED TO AGONIST
Indications for Repeated Contraction (3)
Weakness
Muscle imbalances
Lack of endurance
DIRECTED TO AGONIST
Used to improve the ability to initiate movement
Rhythmic initiation
DIRECTED TO AGONIST
Indications for Rhythmic Initiation (5)
Spasticity
Rigidity
Inability to initiate movement (apraxia)
Motor learning deficits
Communication deficits (aphasia)
DIRECTED TO AGONIST
Technique of emphasis provides repetition of isotonic contraction without sustained effort
Hold relax active motion (HRA)
DIRECTED TO AGONIST
Indications for Hold Relax Active Motion (HRA)? (4)
Inability to initiate movement
Hypotonia
Weakness (lengthened range)
Marked imbalances between antagonists
DIRECTED TO AGONIST
Alternating holding contractions of opposing muscle groups
Alternating isometrics
DIRECTED TO AGONIST
Indications for Alternating Isometrics (4)
Instability in weight bearing and holding
Poor antigravity control
Weakness
Ataxia
REVERSAL OF ANTAGONISTS
What are the four specific techniques? (4)
Slow reversal
Slow reversal hold
Rhythmic stabilization
Quick reversal
REVERSAL OF ANTAGONISTS
Involves an isotonic contraction of the antagonist → isotonic contraction of the agonist
Slow reversal (SR)
REVERSAL OF ANTAGONISTS
Involves an isotonic contraction → isometric contraction of the antagonist → isotonic contraction of the agonist
Slow reversal hold (SRH)
REVERSAL OF ANTAGONISTS
Indications for Slow Reversal/Slow Reversal-Hold/Quick Reversal (5)
Inability to reverse directions
Muscle imbalances
Weakness
Incoordination
Lack of endurance
REVERSAL OF ANTAGONISTS
Rapidly alternating isotonic contractions of antagonists
Quick reversal (QR)
REVERSAL OF ANTAGONISTS
Progression of alternating isometrics; co-contraction of opposing muscle groups
Rhythmic stabilization
REVERSAL OF ANTAGONISTS
Indications of Rhythmic Stabilization (6)
Instability in weight-bearing and holding
Poor antigravity control
Weakness
Ataxia
LOM d/t muscle tightness
Painful muscle splinting
RELAXATION
What are the four specific techniques? (4)
Contract relax (CR)
Hold-relax (HR)
Slow reversal-hold-relax (SRHR)
Rhythmic rotation (RRO)
RELAXATION
Indication for Contract-Relax (CR)
Limitation of motion d/t tightness and spasticity
RELAXATION
A relaxation technique usually performed at the point of limited ROM in the agonist pattern
Hold-relax (HR)
RELAXATION
Indication of Hold-Relax (HR)
LOM d/t muscle spasm, pain, or tightness
RELAXATION
Under HR, _______ into the newly gained range of the agonist can also be performed and serves to maintain the inhibitory effects (through reciprocal inhibition)
Hold relax - active contraction (HRAC)
RELAXATION
Indication for Rhythmic Rotation
Hypertonia that results to LOM